


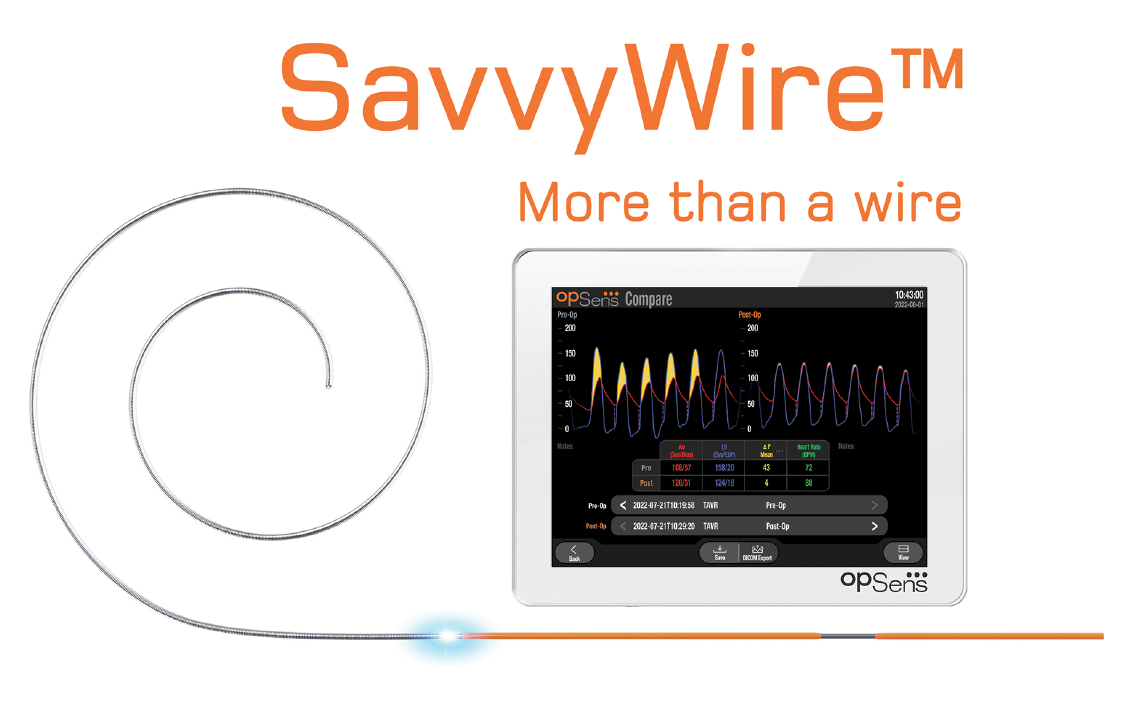
SavvyWire™: A Three-in-One Wire for Transcatheter Aortic Valve Replacement (TAVR)
The SavvyWire is a Guidewire, Provides Hemodynamic Measurement, and Offers Rapid Left Ventricular Pacing
The SavvyWire is a Guidewire, Provides Hemodynamic Measurement, and Offers Rapid Left Ventricular Pacing
Can you tell us about your practice?
I am part of a physician group called Midwest Cardiovascular Institute that works out of Edward Heart Hospital, located in the western suburbs of Chicago. The Heart Hospital itself has 8 cath labs. We were amongst the first centers to do transcatheter aortic valve replacement (TAVR), and our procedure mix includes Watchman (Boston Scientific), MitraClip (Abbott Vascular), tricuspid valve intervention, and patent foramen ovale (PFO) closures. We are fortunate to be a busy center, and have done a few thousand TAVRs and at least 500 Watchman procedures. The development of structural heart and other programs requires the hospital and physicians working together, not just on capital equipment and the cost of the devices, but in terms of coordination and agreement about how to grow a program. The administration and medical staff’s ability to work together has probably been our ‘secret sauce’. We are blessed in that our hospital works extremely well with us in terms of support.
We are hearing a lot about lifetime patient management, and the importance of hemodynamics with respect to TAVR procedures. What does this mean to you and your patients?
From our standpoint, the holy grail is figuring out how to optimize hemodynamics at the time of the procedure. Hemodynamics is ultimately at the core of what we are doing, whether it is improving the hemodynamics of the valve, flow through a coronary artery, or managing heart failure (managing stiffness of the ventricle). After the actual deployment of the valve, we want to know if it is necessary to post dilate to either change the gradient or decrease the amount of insufficiency. Prior to the SavvyWire (OpSens Medical), it has been cumbersome to make that decision. It requires taking your wire out, measuring pressure, measuring gradient, et cetera. We want to obtain the best immediate result to give the patient the best long-term result. Particularly from a TAVR standpoint, our focus is on how to get the single best result during the procedure, including hemodynamics, low pacemaker rate, and the least amount of aortic insufficiency possible.
Can you tell us about your use of the SavvyWire?
You could argue that there haven’t been many recent improvements in the TAVR procedure other than the move to conscious sedation. The procedure itself has been fairly standard the last 5 to 7 years. The SavvyWire can improve the efficiency, save a step, and lead to better outcomes by the measurement of hemodynamics in a real-time fashion. We can not only perform left ventricular (LV) pacing with the SavvyWire, but measure the hemodynamics of the valve pre, when we cross the valve, and post, when we are done. The Sapien 3 (Edwards Lifesciences) transcatheter aortic valve requires rapid pacing when you go up with the balloon. Even with use of the Evolut (Medtronic), there are times that pacing is required until the valve is fully deployed and functional. Everyone is looking to improve the efficiency of our procedures and, in theory, improve the quality as well as decrease the cost. If you have to access the vein and put in a pacemaker, it doesn’t seem like a lot, but it does take time and sometimes the pacer doesn’t go up the way you want it to. There are the occasional right ventricular perforations from the pacemaker wire. All these concerns can be eliminated by pacing through the SavvyWire, which is a straightforward process. You cross the valve, put in your pigtail, and put in the SavvyWire, which is, in my experience, probably about equal to a Safari wire (Boston Scientific) in terms of stiffness. Then you can pace, but the SavvyWire also allows you to measure the gradient pre and post valve placement on that same wire. The advantage is not just that the SavvyWire saves time, but we can also measure hemodynamics in real time to obtain a hemodynamic fingerprint of the patient’s new valve. Do we need to post dilate or is that gradient more than acceptable? Do we need to fracture a valve or not when cracking a previously implanted valve? Having continuous hemodynamics differentiates the SavvyWire from the typical routine. Without having to change out a pigtail or flush a catheter, we can find out the resting gradient on the table when we are done, in real time. It is zeroed already and all we have to do is measure the gradient. We have been using SavvyWire now for a little over a month. We have switched to its use as part of our routine.
Before the SavvyWire was available, what was your process?
Some centers measure a gradient on every case. Some centers don’t measure any. It varies from site to site. We were probably somewhere in between, measuring if we had a concern about either a small valve or, if we were doing a valve-in-valve, measuring if we had a concern about whether it was necessary to fracture the valve. In these cases, we would measure the gradients pre and post. If we thought it would change our management, we were going to measure the gradient. For something like a 29 mm Sapien 3 valve put in a relatively straightforward 78-year-old patient, we probably were not routinely measuring a gradient. Now, with the SavvyWire, we can measure and correlate it the next morning. The echo the following morning will always be a slightly higher gradient than what we get on the table because of sedation. It really takes no additional time, while providing additional information. Now we can measure not just the patients we think we are going to act on, but everyone in general. It is so nice to know before they go.
How does the SavvyWire compare in terms of the wire stiffness and deliverability to what you were using prior to its introduction?
The stiffness of the wire is a little greater than a Safari, but not to the extent of a Lunderquist (Cook Medical). There are two different sizes at the end that are pre shaped. One is small in case you have a very small apex of the ventricle, like for a very hypertrophic ventricle, and here you can use the smaller circle at the end. The other shape is more normal in size. Deliverability hasn’t been an issue. We haven’t had any loss of capture or any problems with pacing. A natural question might be, suppose the person goes in asystole afterwards, what do you do? It is simple. We turn the pacemaker back on and wait a little. If the patient remains in asystole and they are going to need a pacemaker, we access the vein and put in a temporary pacemaker until the electrophysiology service can put in a permanent pacemaker. Interestingly, this has already happened. Fortunately, we had already talked about it as a team on the very first case. We said, “Let’s pretend as if we had asystole. What would we do?” Then we went through the steps of where we would clamp the wire, how we would pace, and who would do what. On our third case, we did have asystole. The person didn’t need a pacemaker, but for our team, it was effortless and there was no panic in the room. In fact, the person didn’t lose capture for more than 5 seconds until sinus rhythm was restored. I find the SavvyWire makes us more efficient. We don’t have to access the vein, we don’t have to put in a pacemaker, and we can get in and out of the case more efficiently than we did before. Before we started using the SavvyWire, I was excited to try it, because it is innovative and at least worth a shot. Now, at this point, we haven’t done a case without a SavvyWire since we started use. We are not sitting in our TAVR meeting on a Thursday asking, “Are we going to use a SavvyWire or not?” It has migrated into part of the standard of how we do the procedure.
How many minutes do you think are being saved with the use of the SavvyWire?
We don’t have our numbers yet. We decided after our first 10 cases to do a quarter’s worth of numbers to determine our mean, because it is hard to determine time saved on a case-to-case basis. At this point, however, my sense is that we are probably saving about 10 to 12 minutes per case due to fewer exchanges and not needing venous access.
Do you have advice for another center that might be interested in trying the SavvyWire?
Any time you get a new product, go through its use first, before you go in the room. There is a different sequence of steps that is easy to learn, but they are different. Ask, what are the new steps? What are the pitfalls? Rehearse once, before you use it. If the patient goes asystole, who is going to do what? There is a clamp that you have to put on the wire: who is going to clamp that on? Who is going to activate the pacemaker? It is easier to handle a problem having first walked through the problem and anticipated it.
I don’t want to say that the SavvyWire is idiot- proof, but it is fairly straightforward. I would encourage anyone to try it. I think it will speed up your case and you can definitely eliminate right ventricular (RV) perforations. When we first started, we did not use it with Evolut cases, because sometimes you have to pull the wire back and we were concerned about maintaining LV wall contact. However, that has not been an issue for us and now there are not any concerns about using the SavvyWire in Evolut cases. Other than wrong sizing and calcium, the biggest issues of TAVR are the length of pacing runs. How do you keep it short when you have different nurses or technologists handling the temporary pacemaker? Having your pacing fairly simple and predictable with the SavvyWire, no matter who is in the room, only adds to the safety of the procedure.
Any final thoughts?
Has there been a problem? No. Would I go back to the old way? No. I think probably the biggest potential complication would be related to loss of capture, which we have not seen. Pacing and wall contact with the SavvyWire have been well-thought out and it is designed well from an engineering standpoint. We do keep the milliamperes (mA) at the highest output during the pacing run, whereas before, when we had a temporary pace, we put the mA down to five or 10. I don’t see any major negatives at this point. Also, being able to measure hemodynamics means somewhere down the road people will be able to apply fuzzy logic as to when you should try and crack a valve or when you shouldn’t, as opposed to just taking these raw numbers as we do currently. As data are collected, we will be able to determine, in the long run, how people do over X period of time with Y amount of gradient, and whether they have higher, better outcomes or lower outcomes. I expect it will allow for more predictive analysis as we go forward.
This article is supported by OpSens Medical.
Click here to learn more about SavvyWire.
Mark Goodwin, MD
Midwest Cardiovascular Institute
Edward-Elmhurst Health,
Naperville and Elmhurst, Illinois
Keep Reading:
Hemodynamics That Can Make For a Lifesaving Decision in the Cath Lab
A Brief Review of Hemodynamics for Structural Interventions, Part 1: Mitral Regurgitation



