


Total Vessel Imaging With the Gentuity High-Frequency Optical Coherence Tomography System
What is your background and experience in intravascular imaging?

I was an early adopter of optical coherence tomography (OCT). I participated in the development of the very first generation when OCT came to the United States and was involved with the image analysis efforts that were part of the first FDA approval. It has been a long journey with intravascular OCT in not only the research side, but also in the clinical arena. OCT has now been part of my day-to-day practice for more than a decade. My go-to intravascular imaging is OCT, with a small percentage of intravascular ultrasound (IVUS) use. I am currently working with the next-generation device, High-Frequency OCT (HF-OCT) (Gentuity). I had the privilege of doing the first-in-human case here at Tampa General Hospital and continue to enroll cases as we build on the first clinical experience. We are also enrolling patients in a second trial that involves side-by-side use of HF-OCT and pressure measurements.
What are the benefits of using intravascular imaging?
The use of intravascular imaging has allowed us to improve percutaneous coronary intervention (PCI) techniques and device selection. Starting with IVUS, intravascular imaging has been utilized in interventional cardiology since the late 1980s, and both IVUS and OCT have been instrumental in helping us to perfect stenting techniques. With IVUS, we learned that high-pressure post dilatation is important and as a result, we have been able to reduce stent under expansion and better adapt our use of anticoagulation. IVUS has also been instrumental in learning how atherectomy and other adjunctive devices work. With OCT, we moved away from cross-sectional analysis and now interact with the data in a volumetric fashion, with fully automated lumen segmentation, stent planning, and expansion evaluation readily available. Plaque characterization is also superior with OCT and helps to guide adjunctive therapies.
Over the last five to seven years, the biggest development has been a greater emphasis on pre-stent imaging for the purposes of procedural planning. We already know that intravascular imaging can impact operator decision making. Approximately 80% of the time, when operators are asked to commit to a strategy based on angiography, they change that strategy if intravascular imaging data is available.1,2 My generation grew up using intravascular imaging post stenting: we put in a stent, checked placement with intravascular imaging, and tweaked as needed. We incorporated the message that good stent expansion is important for the patient outcome. Now we are learning that we gain the most from intravascular imaging by using it pre intervention to decide whether the vessel needs additional preparation, whether with predilatation or use of an adjunctive device such as atherectomy or intravascular lithotripsy, and then for stent selection. We are guided by what is called the MLD MAX algorithm.3 The first three letters, MLD, refer to components to consider during the pre-stent phase (morphology, length, diameter) and the MAX refers to components of the post stent phase (medial dissection, apposition, expansion). OCT holds a special position for pre-stent imaging because the characterization of tissue, particularly calcium and lipid, is more precise and complete with OCT. OCT can provide parameters such as calcium thickness that cannot be obtained with IVUS.
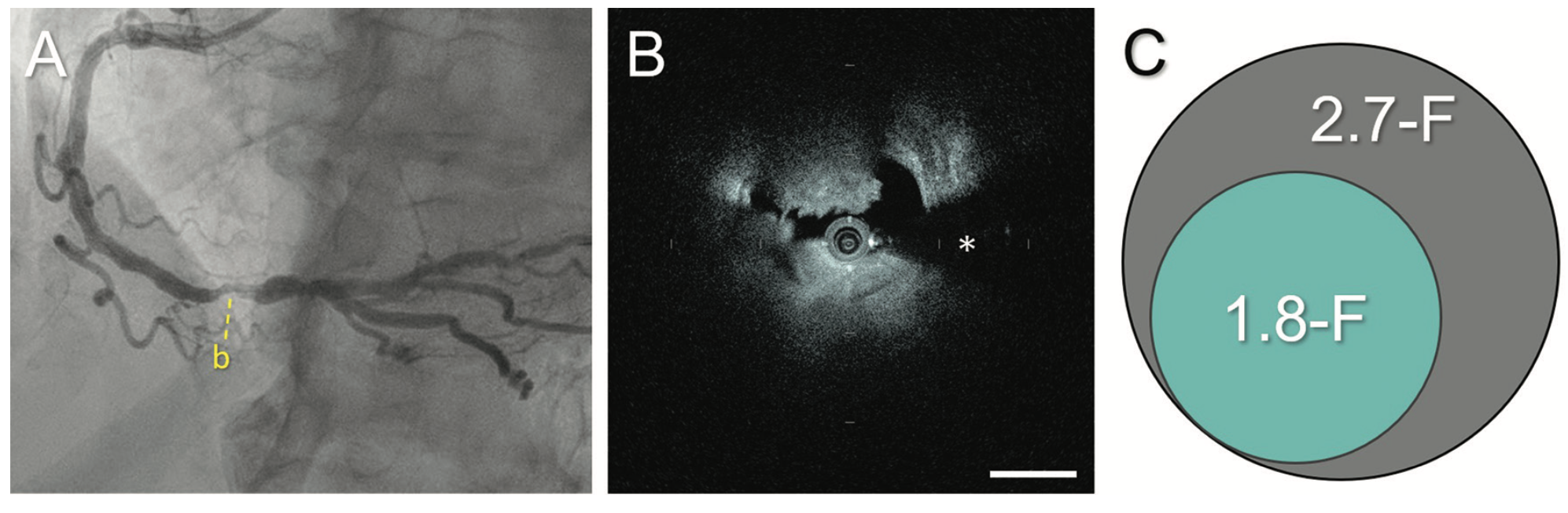
HF-OCT is even more appealing for pre-stent imaging because it has a very low-profile catheter that is almost 60% smaller than the standard OCT catheter, allowing it to cross tight lesions with greater ease. HF-OCT also features a 3X faster pullback. IVUS pullback is one millimeter per second, conventional OCT can reach 36 millimeters per second, and HF-OCT is 100 millimeters per second. In one second, HF-OCT provides a full image of the artery. We are saving seconds on the procedure with HF-OCT use, but this is not the most important benefit. With standard OCT, pullback takes approximately 3 seconds and the vessel continues moving, meaning OCT’s ability to quantify various aspects of the vessel is impacted as well as the ability to clear the blood. The combination of very fast pullback, longer pullback, and low crossing profile make HF-OCT an optimal imaging modality for pre-stent imaging. It performs equally well for post-stent imaging, but the main highlight is that the benefits of HF-OCT go hand-in-hand with the shift in the attention to pre-stent imaging.
Does an HF-OCT image differ in resolution from a standard OCT image?
The energy source is still the same: a laser that operates on the near-infrared range. The resolution is going to be very similar, but HF-OCT offers us an important improvement in terms of having a larger field of view and having the capability to image vessels with diameters all the way up to 6 millimeters (mm), including the left main.
How does the ability to capture a larger field of view affect the use of HF-OCT?
HF-OCT can capture any coronary size, including the left main coronary artery. The FDA has indicated HF-OCT for use in vessels from 1.8 mm to 6 mm in diameter. Gentuity was able to show that with HF-OCT’s smaller catheter, it can image smaller vessels, and with its larger scan range, it can image larger vessels. I do want to emphasize HF-OCT’s ability to image the left main, because that is where, in terms of clinical outcome, data support the use of image-guided intervention for left main disease, even supporting a reduction in mortality.4
Is HF-OCT the next generation of OCT or will these two devices co-exist?
I think HF-OCT has the potential to displace conventional OCT. IVUS could be preferable in some cases, like a chronic total occlusion case where there are limitations for imaging with OCT, but I don’t see the need for labs to have three intravascular imaging modalities like conventional OCT, HF-OCT, and IVUS.
How do you decide to use OCT versus IVUS?
My practice is 95% OCT and 5% IVUS use. The 5% of IVUS use is reserved for ostial left main and a subset of chronic total occlusions in which I cannot displace blood by antegrade injection. It is a very specific situation, because OCT requires blood displacement in order to visualize the artery. In an ostial left main, the flow is very high in the aorta and you don’t get a consistent image with OCT.

You mentioned a new trial. What will it tell us about the future of HF-OCT?
We are looking at combining physiologic and anatomic assessment, and are in an early stage of data collection. The fact that this trial has just started is quite exciting because I believe it may potentially disrupt workflow in the cath lab.
At present, the pressure wire is our go-to device in order to determine the physiological severity of a lesion and whether it needs to be treated. If treatment is required, then therapy can be guided with the use of OCT to technically achieve a better stenting result. In this study, we are performing a side-by-side assessment of the physiology and anatomy, similar to what was recently done with the FUSION trial, which also evaluated pressure wire and OCT use side by side. The ultimate goal is to create a one-stop shop, a single catheter that measures and provides physiology and anatomy in a single one-second pullback. The benefit is more than saving the use of one additional catheter or the time associated with measurement. It is about gaining the ability to have perfectly co-registered data of physiology and anatomy in our hands.
A common challenge we have in the cath lab is determining exactly how much stenting is needed. The first question in approaching this problem is a binary one: yay or nay for PCI. If the answer is yay, we often struggle to determine if we should spot stent, if we should treat a very diffuse lesion with a full metal jacket, and so on. Our hope is that the data from side-by-side use of HF-OCT and physiologic measurement will allow us to determine how much of an ischemic burden is left behind if one treatment approach is offered versus another. These are uncharted waters. Current data already support systematic post-stent pressure wire assessment. We often learn of and are disappointed to have a residual ischemic burden, which is correlated with patient outcome. Yet we don’t systematically use a pressure wire post stenting, because of time and cost, but also because it is difficult to know how to respond to that information. If this information can be consolidated into a single tool that has anatomy and physiology with a perfect co-registration, I forecast much more usable data, data we can interact with and act upon.
If you want to assess physiology before committing to a stent or a strategy, HF-OCT is an ideal platform from which to start. If you tell me as an operator that I am going to give you an image, but you need to spend some time correcting the lumen, in 10 seconds, you have lost my interest and attention. The process has to be fully automated so that ultimately, the computer can provide you with a measurement, and a prerequisite is pre-stent imaging. HF-OCT, because of its inherent characteristics — a small catheter profile, and very long and fast pullback — is an ideal platform for pre-stent imaging. In my early experience, even a severe 90% stenosis can easily be crossed prior to any kind of vessel instrumentation, and HF-OCT provides consistent, quality imaging. With this next-generation technology, we hope to enable even better treatment and optimization of PCI. It is a bright and exciting future.
This article is sponsored by Gentuity.
References
1. Stefano GT, Bezerra HG, Mehanna E, et al. Unrestricted utilization of frequency domain optical coherence tomography in coronary interventions. Int J Cardiovasc Imaging. 2013; 29: 741-752. doi: 10.1007/s10554-012-0135-0
2. Wijns W, Shite J, Jones MR, et al. Optical coherence tomography imaging during percutaneous coronary intervention impacts physician decision-making: ILUMIEN I study. Eur Heart J. 2015 Dec 14; 36(47): 3346-3355. doi: 10.1093/eurheartj/ehv367
3. Bezerra HG, Sheth T. Analysis of changes in decision-making process during OCT-guided PCI. Presented at the PCR e-Course 2020; June 25, 2020.
4. Kinnaird T, Johnson T, Anderson R, et al. Intravascular imaging and 12-month mortality after unprotected left main stem PCI: an analysis from the British Cardiovascular Intervention Society database. JACC Cardiovasc Interv. 2020 Feb 10; 13(3): 346-357. doi: 10.1016/j.jcin.2019.10.007


