A Historical Overview of the Field of Cardiac Electrophysiology (1872-1990)
© 2024 HMP Global. All Rights Reserved.
Any views and opinions expressed are those of the author(s) and/or participants and do not necessarily reflect the views, policy, or position of EP Lab Digest or HMP Global, their employees, and affiliates.
EP LAB DIGEST. 2024;24(3):18-20.
Kriegh Moulton, MD, Director/Faculty, Critical Care Education, Calistoga, California
This review outlines some of the important developments in the fields of electrocardiography and electrophysiology (EP). It is divided into 4 periods, ending with the emergence of radiofrequency (RF) catheter ablation.
Early Period (1870-1910)
This period began with the development of the capillary electrometer in 1872. Gabriel Lippmann, a physicist from Luxembourg who was best known for his development of color photography, devised it to record or verify electrical potential, much like a primitive voltmeter. From previous observations that a drop of mercury sitting in a puddle of weak sulfuric acid could “vibrate” when touched with a nail or if a small voltage difference was applied, Lippmann constructed a vertical glass capillary tube containing mercury and sulfuric acid. The interface between the 2 liquids within the capillary tube vibrated when exposed to small currents. A tiny photographic transducer aimed at the interface projected the meniscus’ cyclic movement onto moving paper which, in turn, portrayed the time course of the electrical event.
Lippmann did not think that the capillary electrometer would have value in human physiology, but in 1887, British physiologist Augustus Waller took an interest. He attached electrodes to the arms of a subject and connected them to each end of the mercury/H2SO4 column. The meniscus’ vibration at the interface between the 2 liquids corresponded with cyclic variations in the electromotive force or voltage differences appearing at the skin surface with each heartbeat. These experiments were performed on his dog Jimmie and his lab assistant.
Important anatomic discoveries involving the conduction system date back to 1845 with the first description of Purkinje fibers by Jan Evangelista Purkinje. These fibers were initially thought to be cartilage due to their whitish appearance.
Because the annulus is the site where the atria connect to the ventricles, it was, unsurprisingly, a region of interest to early anatomists. Accessory connections were described between 1876 and 1893, first by Giovanni Paladino and later by AF Stanley Kent. Also, in 1893, Wilhelm His first described the bundle of His. Ludwig Aschoff and Sunao Tawara provided the first descriptions of the atrioventricular (AV) node in 1906-1907. Arthur Keith and Martin Flack described the structure of the human sinus node in 1907. Thus, the discovery of the components of the conduction system unfolded in an order opposite to that taken by an impulse during the normal activation sequence.
Because the Purkinje system provided a direct connection between the AV node and ventricles, it was speculated there might be similar connections to the sinus node. Enter the internodal tracts. The concept of internodal tracts has held the attention of cardiologists for over 110 years despite a lack of any physiologic or histologic evidence.
Augustus Waller coined the term electrogram, referring to the deflection on the surface electrocardiogram (ECG) representing depolarization.
The string galvanometer was developed by Wilhelm Einthoven to improve the sensitivity to the recorded electrical potential variations on the skin surface, becoming the basis for the current electrocardiograph.
There is speculation about the origins of the naming for ECG waveforms. One proposed explanation is rooted in geometry; since the ECG represents the heart’s electrical activation displayed as a curvilinear waveform, their nomenclature was based on a centuries-old geometry convention. This convention names points on a circle (P, Q, R, S) rather than those describing the points on a line (A, B, C, D).
The Cambridge Instrument Company manufactured the first production model of the ECG in 1903. The first electrocardiograph in the US was given by Einthoven to Alfred E Cohn and was subsequently placed in the library museum at Tulane University in New Orleans.
Period of Electrocardiography (1905-1945)
The first electrocardiographs were large, heavy machines that could only be placed on the floor or a sturdy table. They became portable in 1928, sporting the fashionable color of the era’s automobiles: flat black.
The most obvious information the ECG provided applied to disorders in the cardiac rhythm, and, as a result, this was its initial focus. Meaningful diagnostic clues to specific types of underlying structural heart disease were not well understood or known, so descriptions of ECG markers for conditions such as hypertrophy, chamber enlargement, or myocardial ischemia/infarction would await the addition of more leads.
Einthoven devised the first ECG leads, I, II, and III, known as the “standard limb leads.” These bipolar leads lie within the frontal plane and, as such, reflect the composition of a wavefront of activation lying within that plane for all ECG waveforms. Together, the 3 leads comprise the “triaxial reference system” used to describe the mean frontal plane QRS axis: the general direction that which the ventricular impulse travels within the frontal plane. Knowing the mean QRS axis would provide valuable diagnostic information.
By 1932, Frank Wilson introduced the 6 precordial leads, adding another diagnostic dimension, the horizontal plane, with which implications about the structural condition of the heart could be expanded upon. In 1942, Emanuel Goldberger introduced the final complement of the 12 leads by adding the augmented unipolar limb leads (aVR, aVL, and aVF) to the frontal plane. Incorporating more leads increased the number of “perspectives” or views of electrical activation and recovery. The ECG could now be used to accurately regionalize information into the fundamental anterior, posterior, inferior, and lateral anatomical orientations allowing one to better define where in the heart a problem could be found.
Vectorcardiography, an attempt to provide a more 3-dimensional perspective of cardiac activation, was introduced but began to lose favor by the late 1960s because of its complexities, cumbersome technology, and the apparent lack of incremental benefit over the existing scalar ECG.
The most challenging aspect of arrhythmia analysis is understanding the role of the AV junction, both in its ability to conduct impulses antegradely and retrogradely, but also in how that may affect subsequent impulse formation or conduction. The limited understanding of the AV node’s anatomy and physiology, together with the transition to the ‘12-lead’ ECG, shifted focus towards analyzing the ECG’s component waveforms. This shift aimed to use these waveforms to identify conduction defects and structural heart diseases, including chamber enlargement, hypertrophy, and the impacts of myocardial infarction on the ECG. Today, the 12-lead ECG and chest X-ray remain critically important frontline medical tools, unlike any other early 20th-century diagnostic modality.
Period of Cellular and Applied EP (1949-Present)
Gilbert Ling and Ralph Gerard reported the first application of the microelectrode to record the cellular action potential using the large nerve fibers of the giant squid axon at the University of Chicago. Widespread application of their tool was immediate. Soon, the electrophysiology of any bioelectric cell could be described by impaling it with a microelectrode and recording its action potential.
Eventually, it became clear that transmembrane potential variations comprising the action potential were due to currents carried by specific ions into (inward currents) or out (outward currents) of the cell. Inward currents depolarize while outward currents repolarize. Energy-dependent pumps within the outer cell membrane were discovered to maintain the normal distribution of ions. Eventually, the effect of drugs and disease (particularly ischemia) on the behavior of these currents became a focal point of interest.
Following this time, the knowledge provided by cellular EP was translated into an understanding of how the cardiac impulse’s spread of excitation propagated throughout the heart: first in the canine model, then in the human. This notion represented a translational link between cellular and and extracellular electrical phenomena. Further advances in our understanding of normal excitation led to an inquiry into the basis for arrhythmia mechanisms, particularly reentry, which remained only a theoretical construct in the first half of the 20th century.
Reentry was confirmed as a mechanism of many common arrhythmias between the latter 1960s and early 1970s, including ventricular tachycardia (VT), AV reentry, and AV nodal reentry. Notably, Kenneth Rosen et al at the University of Illinois provided the first evidence for the basis of AV nodal reentry based on intracardiac catheter recordings (1972).
During the mid-1970s, Ben Scherlag, Nabil El-Sherif, Ed Berbari, and Jorge Gonzales, provided the first glimpse of the “continuous electrical activity” responsible for the initiation and perpetuation of sustained monomorphic VT in a canine infarction model. This was made possible using Scherlag’s “composite” electrode.
This electrode was constructed using masking tape and 4-0 non-insulated stainless steel sutures. Two or more parallel strands of the suture were sewn into a small (¾” x 1”) piece of masking tape such that the suture was intermittently exposed for contact with the epicardial surface. It was covered with a matching piece of tape, adhesive sides facing, as shown below.
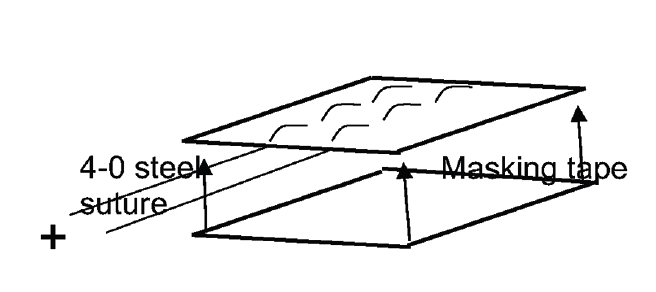
The intermittent exposure of the metal suture on one side of the patch provided multiple contact points on the epicardial surface, enabling multiple sites near each other to be recorded. Completed patches were sewn to the epicardium in a central ischemic zone, a border zone, and a normal zone. This approach disclosed “continuous electrical activity” unique to the border zone and provided proof that an impulse involved in VT remained active throughout diastole. This eventually led to the description of the “figure-of-8” model for reentry once a multipolar electrode design became available. The large epicardial recording area underlying the patch also disclosed “late potentials” within the border zone, allowing Berbari to develop the technique of signal averaging.
Early observations regarding the role of abnormal calcium currents made by Andrew Wit and Paul Cranefield led to the description of “triggered activity.” Abnormalities involving phase 2’s inward calcium current and the Na-Ca exchange system were shown to impair “calcium handling” formulating the basis for early and delayed afterdepolarizations as new mechanisms of arrhythmias.
Period of Clinical Cardiac EP (1967-Present)
Electrophysiologic Testing
The technique of programmed stimulation or extrastimulus testing was described independently in 1967 by Dirk Durrer and Philippe Coumel as a means of initiating or terminating the reciprocating tachycardia associated with Wolff-Parkinson-White (WPW) syndrome. Arrhythmias whose mechanism depended on reentry could be started and stopped by delivering a timely premature stimulus, allowing for systematic study.
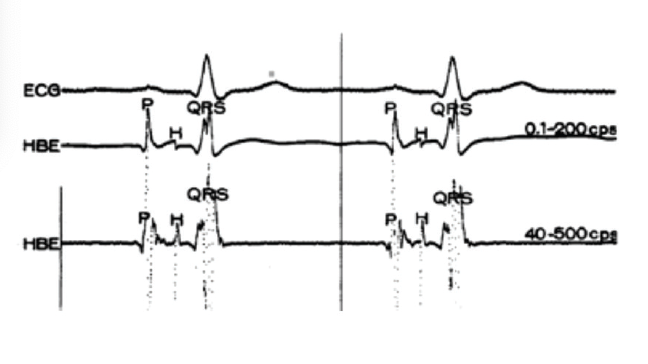
Working with Anthony Damato at the US Public Health Service (USPHS) facility in Staten Island, Scherlag described the technique of His bundle recording in man for the first time in 1969. This recording technique and the advent of programmed stimulation essentially opened the field of clinical cardiac EP.
Many of the patients participating in this research program were volunteers from the nearby Danbury prison in Connecticut. Their procedures were known as “special studies.” The His bundle recording of a prisoner named Max is depicted below. He voluntarily returned for catheterizations many times and his tracing is shown below.
Damato is considered the “father of modern cardiac EP” because the USPHS in Staten Island served as a unique training center supplying the single largest group of electrophysiologists to the United States in the mid-1960s.
The Berry Plan, introduced during the Vietnam War, allowed postdoctoral trainees to continue pursuing their advanced medical training. The NIH has a long list of notable electrophysiologists who received training at the USPHS under Dr Damato and who subsequently established centers of excellence throughout the United States. The American Board of Internal Medicine formally recognized clinical cardiac EP in 1992.
The Implantable Cardioverter-Defibrillator (ICD)
Coronary care units were established in the late 1960s, an idea spirited at Harbor General in Torrance, California. It was clear that ventricular tachyarrhythmias were the cause of sudden death among post-myocardial infarction patients. Guided by the response to programmed stimulation, antiarrhythmic drugs were put to task and reached their heyday by the mid-1980s. However, it was evident that the benefit conferred by these drugs was inadequate. Michel Mirowski and Morton Mower believed that defibrillation, the only effective means of terminating VT or ventricular fibrillation (VF), could be applied to the general population using a miniaturized and implanted version of a defibrillator.
The pharmaceutical industry summarily dismissed the concept, and in 1974, Bernard Lown and Julius Axelrod co-wrote a letter to the editor of Circulation demonizing the “very idea” of an ICD, suggesting that those patients “would be much better served being medicated in a coronary care unit.”
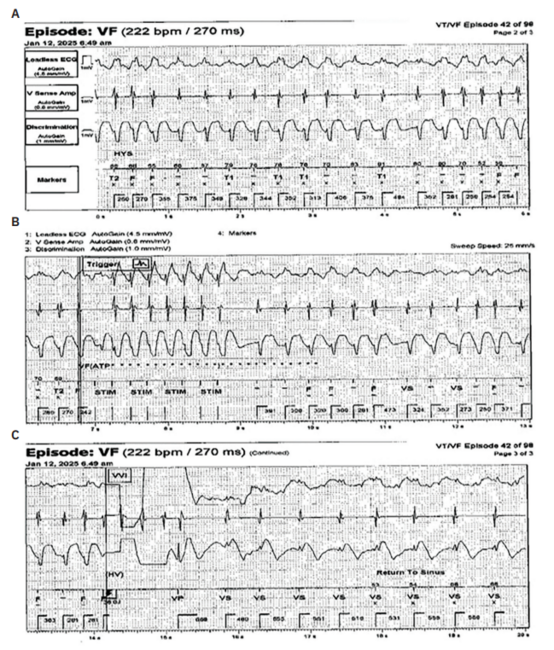
Mirowski and Mower presented the results of a conscious animal study in which VF was terminated using an implantable defibrillator. The abstract was delivered as a movie at the American Heart Association Scientific Sessions in 1978.
The 5-minute, 35-mm black-and-white film highlighted the value of a prototypical ICD, implanted in a mixed-breed dog resembling a German Shepherd. The upper portion of the film’s frame depicts the dog’s real-time rhythm. An implanted AC fibrillator induced VF, followed by the dog sitting down and gently collapsing. Detection and therapy depicted along the frame’s upper border showed the defibrillator to promptly restore sinus rhythm. The dazed dog then struggled upright, shook, and delivered an unexpected but well-formed bowel movement.
The presentation was very well received. The publication of the first human experience appeared in the New England Journal of Medicine (NEJM) in 1980, featuring the first 3 implants by Roger Winkle at Sequoia Hospital in Redwood City, California.
Catheter Ablation
In 1979, while Robert Frank was performing EP testing for VT-related syncope, hemodynamically unstable VT was induced, and amid resuscitative efforts, the subclavian multipolar right ventricular apical catheter slipped back to the region of the AV node. Unbeknownst to anyone, the exposed catheter pin plugs were left lying on the patient’s bare chest, beneath one of the paddles. The 100-joule shock not only restored sinus rhythm, making it the first case of intracardiac cardioversion, but it also caused complete AV block and the first case of AV junctional ablation. This was the beginning of catheter ablation.
Jacques Vedel and Robert Frank’s publication appeared to receive little attention, but within a matter of months, their experience was being replicated in animal studies at the University of Michigan and the University of California-San Francisco to validate the approach. The first clinical manuscripts on catheter ablation using direct current (DC) appeared in the January 1982 issue of NEJM (Gallagher, Duke) and the August 1982 issue of the Journal of the American Medical Association (JAMA) (Scheinman, UCSF).
Eight years of poor outcomes involving DC catheter ablation turned the attention to RF current, a more forgiving energy form already widely used as electrocautery in surgery or as diathermy in physical medicine. The collaboration between Paul Nardella, who later founded the American Catheter Ablation Corporation, Will Webster, then-president and founder of Webster Laboratories, and Sonny Jackman, an electrophysiologist at the University of Oklahoma, led to the development and refinement of the technique of RF catheter ablation between 1987 and 1991.
By 1990, over 120 electrophysiologists visited the EP laboratory at Oklahoma Memorial Hospital to watch the beginning of a new era known as interventional EP. Since 1990, RF catheter ablation has represented the most commonly performed potentially curative procedure in cardiology. n
Disclosure: The author has completed and returned the ICMJE Form for Disclosure of Potential Conflicts of Interest, and reports no conflicts of interest regarding the content herein.
Related Content