

Exacerbation of Postural Orthostatic Tachycardia Syndrome in a Patient With Ehlers-Danlos Syndrome Post-COVID-19 Infection
EP Lab Digest. 2023;23(2):16-18.
Ehlers-Danlos syndrome (EDS) is a connective tissue disorder that often presents with joint laxity and skin hyperelasticity. Dysautonomia symptoms are common among the EDS population. Additionally, current research suggests a link between long COVID-19 and dysautonomia.1,2 Patients with prior dysautonomia linked to EDS are more susceptible to symptomatic exacerbation following COVID-19 infection.2 We provide a brief case and update on our experience treating this patient population.
Case Presentation
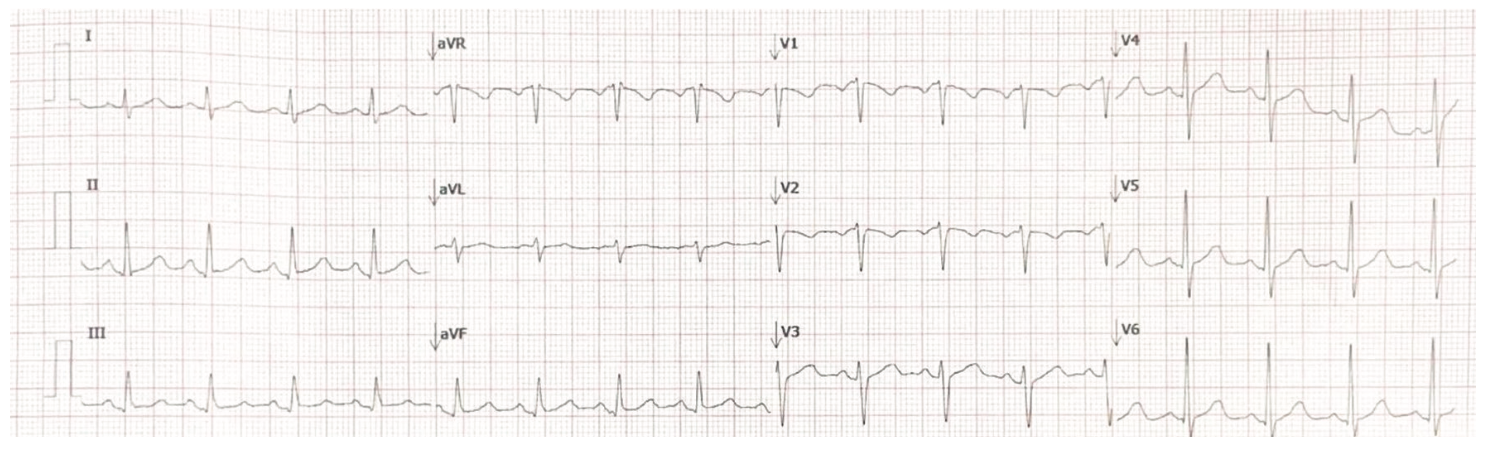
A 22-year-old woman with a past medical history of EDS was referred for cardiac evaluation and management of presyncope/syncope exacerbated by COVID-19 infection. The patient’s chief cardiac complaints included palpitations, chest pain and discomfort, and shortness of breath. Previous medical history consisted of asthma, attention-deficit/hyperactivity disorder, chronic migraines, generalized anxiety disorder, herniated cervical disc, and malabsorption. Her medications included albuterol, atomoxetine, eletriptan, rimegepant, lamotrigine, mirtazapine, and sertraline. Her physical examination revealed no acute distress with bilateral clear lungs and normal cardiac sounds without peripheral edema. Figure 1 demonstrates the patient’s 12-lead electrocardiogram (ECG), which demonstrated sinus tachycardia at 102 beats per minute (bpm) with a normal axis and borderline QTc prolongation (QTc = 458 msec). A previous 2-dimensional (2D) echocardiogram revealed trace mitral and tricuspid regurgitation with no evidence of mitral valve prolapse or aortic dilation. The patient underwent a head-up tilt test (HUTT) at 70 degrees for 20 minutes. Her baseline heart rate was 99 bpm, which went above 130 bpm within a 10-minute period while her blood pressure remained stable. While she described symptoms of presyncope, no syncopal episode occurred.
Discussion
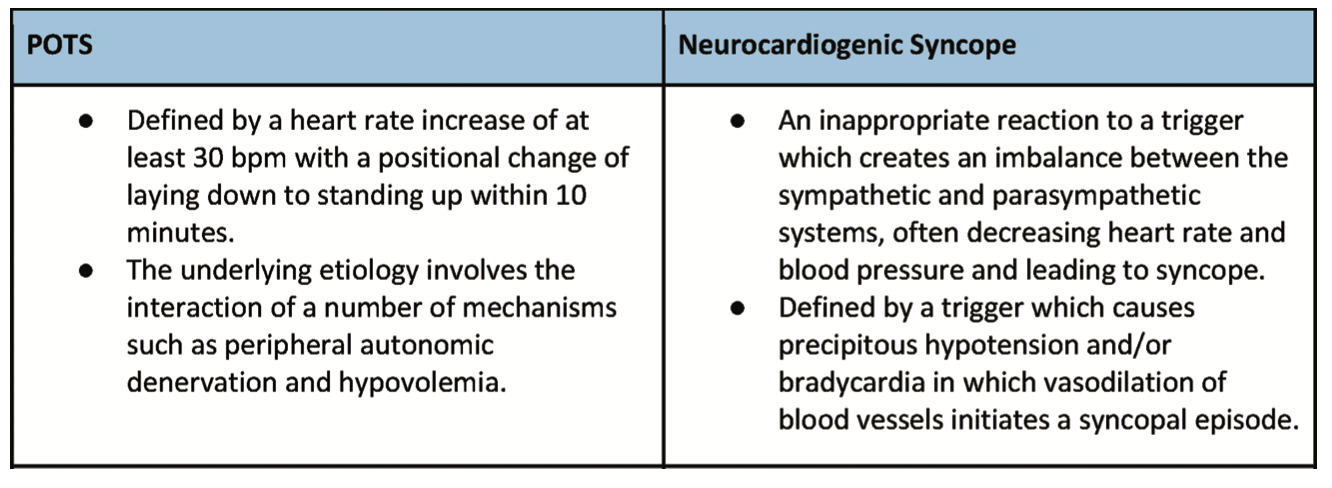
NYITCOM’s EDS/Hypermobility Treatment Center works closely with the Long Island Heart Rhythm Center to provide specialty cardiology services and evaluate patients with EDS and hypermobility syndrome. In the last 4 years, we have treated nearly 100 patients. Figure 2 shows common characteristics of these patients.3 Typically, most patients are female and between 18-50 years in age. Hypermobility and associated joint pain is almost universal. A detailed history, physical examination, and ECG are essential first steps in the workup. Patients commonly experience sinus tachycardia and some have a short PR interval due to enhanced atrioventricular conduction; however, preexcitation syndromes are uncommon. Many of these patients also complain of palpitations and presyncope/syncope. The latter are often related to postural orthostatic tachycardia syndrome (POTS) and confirmed with a positive HUTT, in which the heart rate increases by 30 bpm or more within 10 minutes of standing.4 The tilt table test is useful in this population to help clarify the diagnosis of POTS vs neurocardiogenic syncope. Figure 3 lists the differences between the pathophysiology and definition of POTS and neurocardiogenic syncope.5-7 POTS has specific diagnostic requirements and is positional in nature, whereas neurocardiogenic syncope is often triggered with blood pooling in the lower extremities.7 Oftentimes, the latter results in hypercontractility of the left ventricle and activation of the mechanoreceptor fibers, resulting in unmyelinated C fiber release, which can stimulate a vagal response.7 There is considerable overlap and interaction between the 2 conditions. Many of the treatments for POTS and neurocardiogenic syncope are similar. Specifically, POTS is managed with hydration (such as electrolyte solutions), compression stockings, and increasing salt intake.8 Additionally, patients are counseled to minimize exposure to settings that could exacerbate POTS-related symptoms (such as heat and stress).8 If these conservative measures fail, a cardioselective beta-blocker may be recommended to blunt tachycardic symptoms.8 Other medications such as midodrine and fludrocortisone might occasionally be incorporated in the management of POTS and neurocardiogenic syncope. Calf contraction is particularly helpful in neurocardiogenic syncope. As a last resort, in refractory POTS patients, intravenous hydration can be regularly administered following port insertion. Overall, patient education is important for both conditions.
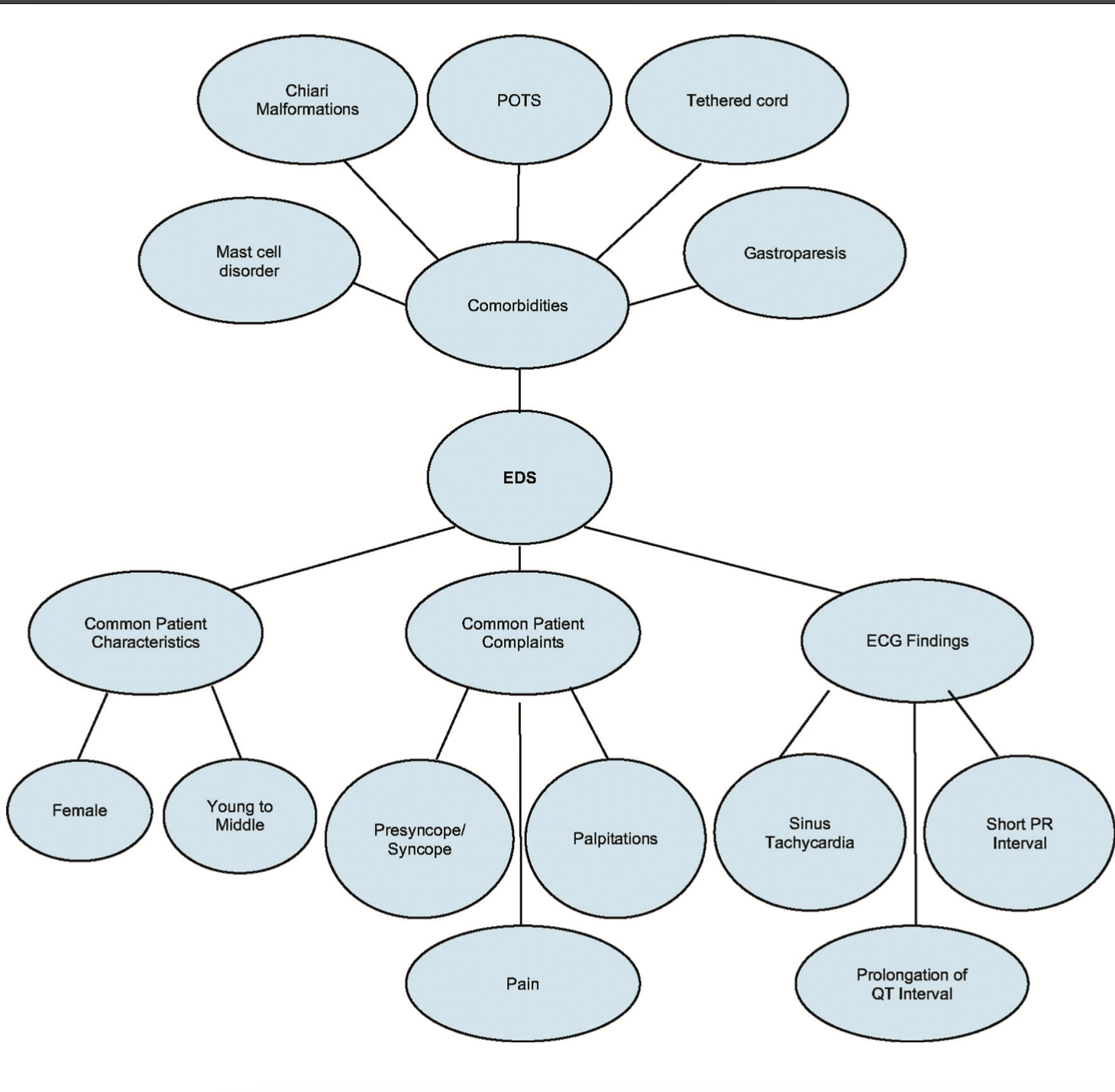
A typical cardiac workup in symptomatic EDS patients begins with noninvasive cardiac testing such as external cardiac monitoring (for preferably 7-14 days) and a 2D echocardiogram (to identify mitral valve prolapse and/or aortic dilation). Although they are quite rare, the latter 2 disorders have still been reported in this condition (less than 5% of our patients). Nonspecific cardiac chest pain is often seen, and exercise stress testing may be helpful at noninvasively ruling out cardiac ischemia as well as diagnosing musculoskeletal pain. Common comorbidities include mast cell disorder, Chiari malformations, gastroparesis, and tethered cord. Rarely, other potentially unrelated cardiac conditions may be identified. In those with unexplained syncope, we typically first insert an implantable loop recorder to aid in the diagnosis. Long-term follow-up often identifies POTS as the mechanism for the patients’ unexplained syncope/presyncope and sinus tachycardia. Only a small percentage of patients are found to have nonphysiologic tachycardias such as ventricular tachycardia, atrial fibrillation, atrial flutter, symptomatic premature ventricular contractions, and paroxysmal supraventricular tachycardia (SVT).
Since the COVID-19 pandemic, we have seen a fair number of EDS patients with an exacerbation of POTS symptoms, similar to the case described here. These symptoms may persist and require treatment with more vigorous electrolyte replenishment as well as other supportive and educational measures. Compliance with hydration and support stockings is essential. One hypothesis suggests that SARS-CoV-2 infection-induced stress may activate the sympathetic nervous system and cytokine system.9 An overaction of these systems may play a role in a prolonged POTS exacerbation in this population.
QT prolongation may occasionally be seen in EDS and hypermobile patients (as was observed in our case), which is often due to polypharmacy. Management of this finding includes limiting specific medications that have this adverse synergistic effect. The multidisciplinary care team should be aware of the interplay of antibiotics, antihistamines, antidepressants, pain medications, and other drugs that might prolong the QT interval. Despite this issue, we have not yet observed drug-induced torsades de pointes in this population; however, a larger cohort might be more conclusive. In general, it is recommended to avoid multiple drugs with definitive QT-prolonging effects.
Conclusion
This article illustrates some of the cardiac findings associated with EDS and hypermobility disorders. The case presented here is typical of those with EDS and POTS. There is a higher incidence of orthostatic intolerance within EDS patients than the general population.10 Although the exact association between EDS and POTS is difficult to determine due to different study methodologies as well as new criteria for diagnosis, a consistent finding of 40% or higher between joint hypermobility and orthostatic intolerance symptoms has been noted.11-14
Long COVID refers to the long-term sequelae that have been recorded following COVID-19 infection. One such example includes POTS or POTS-like symptoms following COVID-19 infection reported in a number of patients.15 In the case presented, COVID-19 infection exacerbated POTS symptoms. Understanding the pathophysiologic link between dysautonomia present in POTS and EDS may drive future research and treatment options for both populations. Invasive cardiac and electrophysiology procedures are rarely needed in these patients. Specifically, recurrent syncope while supine (and without postural changes) might be a sign for more aggressive investigation for paroxysmal SVT and/or ventricular arrhythmias in these patients. If the patient has other cardiac comorbidities such as coronary disease, cardiomyopathy, and/or arrhythmogenic-related conditions, additional cardiac and electrophysiology workup may be warranted.
Disclosures: The authors have completed and returned the ICMJE Form for Disclosure of Potential Conflicts of Interest. They have no conflicts of interest to report regarding the content herein.
References
1. Mathias CJ, Owens A, Iodice V, Hakim A. Dysautonomia in the Ehlers-Danlos syndromes and hypermobility spectrum disorders-with a focus on the postural tachycardia syndrome. Am J Med Genet C Semin Med Genet. 2021;187(4):510-519. doi:10.1002/ajmg.c.31951
2. Dani M, Dirksen A, Taraborrelli P, et al. Autonomic dysfunction in ‘long COVID’: rationale, physiology and management strategies. Clin Med (Lond). 2021;21(1):63-67. doi:10.7861/clinmed.2020-0896
3. Cohen TJ, Riley B, Choi D, et al. Cardiology and electrophysiology considerations of Ehlers-Danlos syndrome and variants, including hypermobile syndromes. EP Lab Digest. 2019;19(11):25-27.
4. Freeman WP, Wieling W, Axelrod FB, et al. Consensus statement on the definition of orthostatic hypotension, neurally mediated syncope and the postural tachycardia syndrome. Clin Auton Res. 2011;21(2):69-72. doi:10.1007/s10286-011-0119-5
5. Anderson JB, Willis MW. Differentiating between postural tachycardia syndrome and vasovagal syncope. Pediatrics. 2017;139(4):e20164161. doi:10.1542/peds.2016-4161
6. Cohen TJ. Practical Electrophysiology, Third Edition. Malvern, PA: HMP Communications; 2016.
7. Centeno EH, Mayuga KA, Fouad-Tarazi F, Shoemaker L, Jaeger F. Syncope. Cleveland Clinic. Published September 2018. Accessed November 16, 2022. https://www.clevelandclinicmeded.com/medicalpubs/diseasemanagement/cardiology/syncope/
8. Raj SR. The postural tachycardia syndrome (POTS): pathophysiology, diagnosis & management. Indian Pacing Electrophysiol J. 2006;6(2):84-99.
9. Al-Kuraishy HM, Al-Gareeb AI, Qusti S, et al. Covid-19-induced dysautonomia: a menace of sympathetic storm. ASN Neuro. 2021;13:17590914211057635. doi:10.1177/17590914211057635
10. Roma M, Marden CL, De Wandele I, Francomano CA, Rowe PC. Postural tachycardia syndrome and other forms of orthostatic intolerance in Ehlers-Danlos syndrome. Auton Neurosci. 2018;215:89-96. doi:10.1016/j.autneu.2018.02.006
11. Gazit Y, Nahir AM, Grahame R, Jacob G. Dysautonomia in the joint hypermobility syndrome. Am J Med. 2003;115(1):33-40. doi:10.1016/s0002-9343(03)00235-3
12. De Wandele I, Calders P, Peersman W, et al. Autonomic symptom burden in the hypermobility type of Ehlers-Danlos syndrome: a comparative study with two other EDS types, fibromyalgia, and healthy controls. Semin Arthritis Rheum. 2014;44(3):353-361. doi:10.1016/j.semarthrit.2014.05.013
13. Miglis MG, Schultz B, Muppidi S. Postural tachycardia in hypermobile Ehlers-Danlos syndrome: a distinct subtype? Auton Neurosci. 2017;208:146-149. doi:10.1016/j.autneu.2017.10.001
14. Miller AJ, Stiles LE, Sheehan T, et al. Prevalence of hypermobile Ehlers-Danlos syndrome in postural orthostatic tachycardia syndrome. Auton Neurosci. 2020;224:102637. doi:10.1016/j.autneu.2020.102637
15. Ormiston CK, Świątkiewicz I, Taub PR. Postural orthostatic tachycardia syndrome as a sequela of covid-19. Heart Rhythm. 2022;19(11):1880-1889. doi:10.1016/j.hrthm.2022.07.014
Related Reading

