Bioresorbable Vascular Scaffolds: A Disappearing Technology, But Should We Let It Vanish?
J INVASIVE CARDIOL 2023;35(3):E151.
Key words: bioresorbable vascular scaffold, BVS, computed tomography coronary angiogram, CT-CA
A 72-year-old gentleman presented with angina. He had previously undergone percutaneous coronary intervention (PCI) to the right coronary artery and left circumflex artery (LCX) with drug-eluting stents. Coronary angiography revealed a long segment of moderate stenosis in the proximal to mid left anterior descending artery (LAD) (Figure 1A). This was treated with Absorb bioresorbable vascular scaffolds (BVS; Abbott Vascular) (Figure 1B) with the use of intravascular ultrasound to confirm adequate stent expansion. He represented 5 years after his PCI with atypical symptoms. A computed tomography coronary angiogram showed the BVS were no longer visible and only the platinum markers were seen (Figure 1C). The scaffolds had been completely reabsorbed, allowing the use of non-invasive imaging to obtain high-quality diagnostic images not affected by artefact, as seen with the DES in the LCX (Figure 1D) preventing the vessel being assessed with the same clarity.
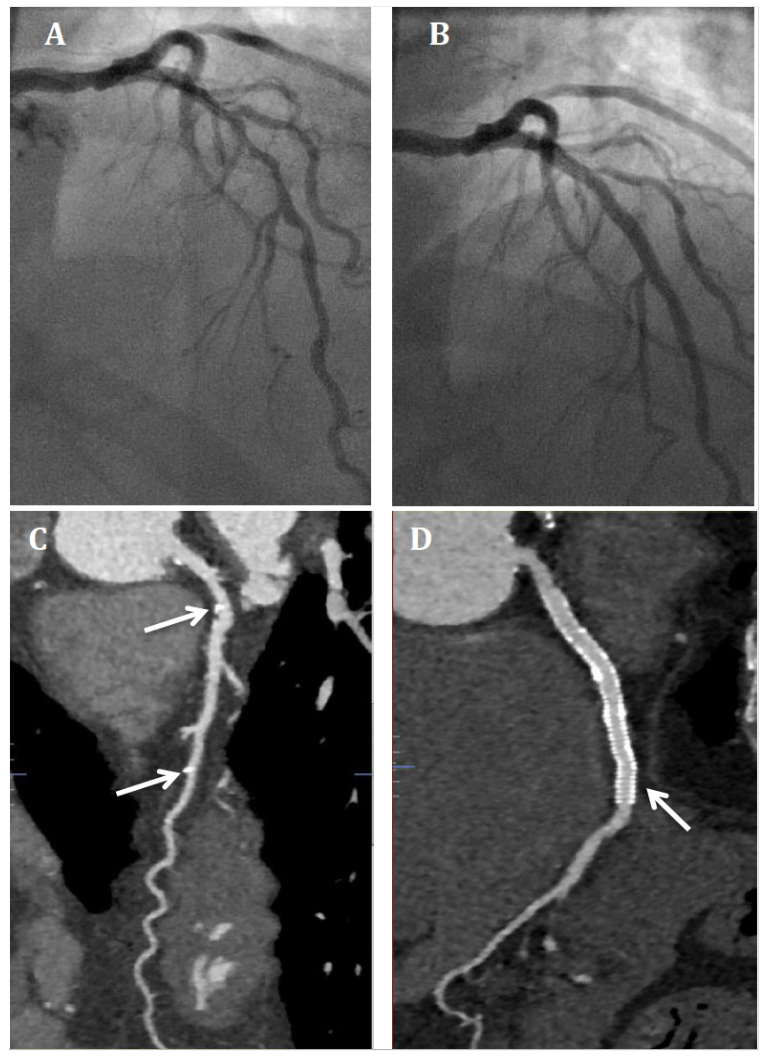
The BVS was designed to overcome the limitations imposed by drug-eluting stents; however, the Absorb BVS showed a 2% very late thrombosis rate. Suboptimal implantation technique has been proposed as a mechanism for the higher BVS thrombosis rate, one posthoc analysis suggested adequate pre and post dilation in addition to proper sizing could reduce BVS thrombosis rates by 70%. This case acts as a proof of concept demonstrating advantages of BVS, namely, the ability to image the target vessel non-invasively and revascularise percutaneously or surgically if required. We advocate continued research and development in this technology given the attractive advantages, particularly in younger patients who are likely to require future coronary intervention and imaging.
Affiliations and Disclosures
From the 1Cardiovascular Division, King’s College London, London, United Kingdom; and 2Dorset Heart Centre, Royal Bournemouth Hospital, Bournemouth, United Kingdom.
Disclosure: The authors have completed and returned the ICMJE Form for Disclosure of Potential Conflicts of Interest. The authors report no conflicts of interest regarding the content herein.
The authors report that patient consent was provided for publication of the images used herein.
Manuscript accepted June 23, 2022.
Address for correspondence: Saad Ezad, MB BCh, Cardiovascular Division, Rayne Institute, St Thomas’ Hospital, Westminster Bridge Road, London, SE1 7EH. Email: saad.ezad@kcl.ac.uk