

Clinical Performance of a Paclitaxel Drug-Coated Balloon in Real-World Percutaneous Coronary Intervention Practice: The PEARL Registry
Abstract
Background. Randomized controlled trials for in-stent restenosis (ISR) and de novo lesions in small-diameter vessels have shown promising results, but data on DCB use in real-world practice are still scarce. The aim of the PEARL (Paclitaxel-Eluting Angioplasty Balloon in the Real-World) registry was to evaluate the safety and efficacy of a paclitaxel DCB in real-world percutaneous coronary intervention (PCI) practice. Methods. Between 2014 and 2019, a total of 513 patients treated with the Protégé paclitaxel DCB (Wellinq) were prospectively included at 4 hospitals in the Netherlands. The primary endpoint was 2-year major adverse cardiac event (MACE), defined as cardiac death, target-vessel myocardial infarction, or target-lesion revascularization (TLR). Results. DCB was used for ISR in 382 patients and for de novo lesions in 131 patients. Acute coronary syndrome was the reason for presentation in 58.9% of patients. At lesion level, 34.1% of lesions were classified as type B2 and 36.1% as type C. Predilation was performed in 62.2% and noncompliant DCB was used in 40.7% of lesions. DCB-related procedural complications were infrequent (3.3%, mostly coronary dissection [2.3%]). Bailout stenting was required in 3.1%. MACE during 2-year follow-up occurred in 17.1% of patients treated for ISR and 9.7% of patients treated for de novo lesions. The incidence of TLR was 11.7% of ISR patients and 2.9% of de novo patients. History of coronary artery bypass grafting and lesion length were predictors of MACE in patients treated for ISR. Conclusion. The use of Protégé paclitaxel DCB for PCI of ISR and de novo lesions is safe and effective during 2-year follow-up.
Keywords: drug-coated balloon, in-stent restenosis, paclitaxel, percutaneous coronary intervention
Percutaneous coronary intervention (PCI) is often performed with implantation of a drug-eluting stent.1 However, stent implantation may be less desirable for recurrent in-stent restenosis (ISR) and for specific lesions characteristics such as small vessel diameters. For such indications, the drug-coated balloon (DCB) has emerged as a therapeutic alternative to stent implantation. Randomized controlled trials have shown promising results for the use of DCB,2 but data on DCB use in real-world practice are still scarce. Furthermore, a wide variety of different DCBs are currently available. Because of the different designs and characteristics of the available DCBs, it has been suggested that there is no class effect and that each DCB has to be evaluated individually.2 The Protégé DCB (Wellinq) is a paclitaxel-coated balloon that features an innovative balloon design in which the drug component is encapsulated in the balloon folds and is only exposed upon inflation, thereby preventing premature drug release. This DCB is available in compliant and noncompliant versions so that predilation of the lesion may not be required. The PEARL (Paclitaxel-Eluting Angioplasty Balloon in the Real-World) registry aims to evaluate the safety and efficacy of the Protégé DCB in real-world PCI practice.
Methods
Study population. The PEARL registry is a multicenter, observational study. Between November 2014 and November 2019, a total of 513 patients who underwent PCI using the paclitaxel-coated DCB were included in 1 of the 4 participating hospitals in the Netherlands. The inclusion criteria were broad and representative to real-world clinical practice. Indications for DCB use included ISR or de novo coronary lesions where the use of DCB was considered to be more favorable than stent placement. Very few exclusion criteria were applicable in order to ensure external generalizability: cardiogenic shock; allergies or contraindications to antiplatelet medication, contrast, or to balloon components that cannot be adequately treated; and life expectancy <1 year. This study was approved by the medical ethics committee and was performed in accordance with the criteria described in the Declaration of Helsinki. Written informed consent was obtained from all included patients.
Drug-coated balloon. The Protégé DCB is coated with paclitaxel in a dose of 3.0 µg/mm2 balloon surface area. It features a drug component that is encapsulated in wings that remain closed prior to inflation. The compliant version is available in 6 diameters (2-4 mm) and 4 lengths (10-30 mm). The noncompliant version is available in 7 diameters (2.5-4.5 mm) and 3 lengths (10-20 mm). The nominal inflation pressure is 6 atm for the compliant version and 12 atm for the non-compliant version. The recommended inflation duration is 30 seconds. The Protégé DCB can be used for a maximum of 3 inflations, with a total application time of 90 seconds. When necessary, a decision for bailout stenting for the treatment of DCB-related coronary dissection was left to the discretion of the operator.
Study endpoints. Clinical follow-up was performed at 1, 6, 12, and 24 months and was focused on the occurrence of cardiovascular events. The study endpoints were adjudicated by a clinical event committee. The primary endpoint was major adverse cardiac event (MACE) during 2 years of follow-up. MACE was defined as cardiac death, target-vessel myocardial infarction, or target-lesion revascularization. Secondary endpoints included the individual components of the primary endpoint, all-cause mortality, any revascularization, and target-lesion thrombosis.
Statistical analysis. The results of the interim analysis in the first 200 patients have been published elsewhere.3 Continuous variables are presented as mean ± standard deviation. Categorical variables are presented as numbers and percentages. Patients lost to follow-up were considered at risk until the date of last contact, at which time point they were censored. Cumulative event rates were estimated according to the Kaplan-Meier method. Cumulative Kaplan-Meier event curves were compared with the log-rank test. The first MACE was counted as the primary endpoint in cases of multiple events. Cox proportional hazard regression analyses were performed to evaluate the associations between baseline characteristics and study endpoints. These results are presented as hazard ratio (HR) with 95% confidence interval (CI). All statistical analyses were performed at the patient level. Stratified analyses were performed on DCB indication (ISR and de novo coronary lesions). Associations between baseline characteristics and clinical outcome were assessed in patients treated for ISR by using Cox regression. Such analysis was not performed in patients treated for de novo lesions because of the small sample size. A 2-sided P<.05 was considered statistically significant. All analyses were performed using R statistical package, version 3.6.2 (R Foundation for Statistical Computing).
Results
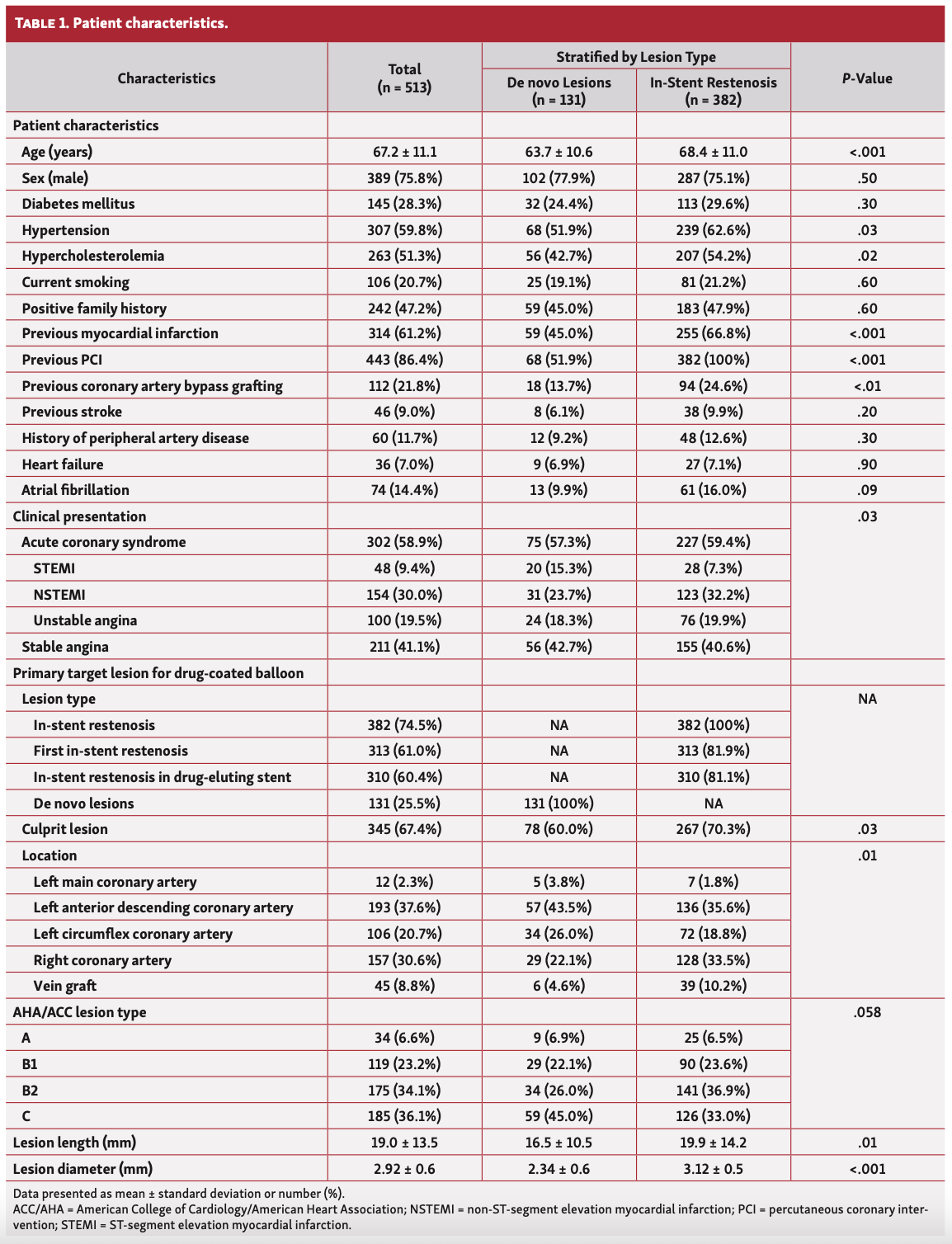
Baseline characteristics. The study population consists of 513 consecutive patients in whom a DCB was indicated at the discretion of the treating physician. Mean age was 67.2 ± 11.1 years and 75.8% were men (Table 1). Patients had a high cardiovascular risk profile, with diabetes in 28.3%, hypertension in 59.8%, history of myocardial infarction in 61.2%, history of PCI in 86.4%, and coronary artery bypass grafting in 21.8%. Clinical presentation was acute coronary syndrome in 58.9% of the patients. The majority of lesions had a high complexity with 34.1% classified as American College of Cardiology/American Heart Association (ACC/AHA) lesion type B2 and 36.1% classified as type C. The procedural characteristics are presented in Table 2. Predilation with a regular balloon without drug elution was performed in 62.2%. The noncompliant version of the DCB was used in 40.7%.
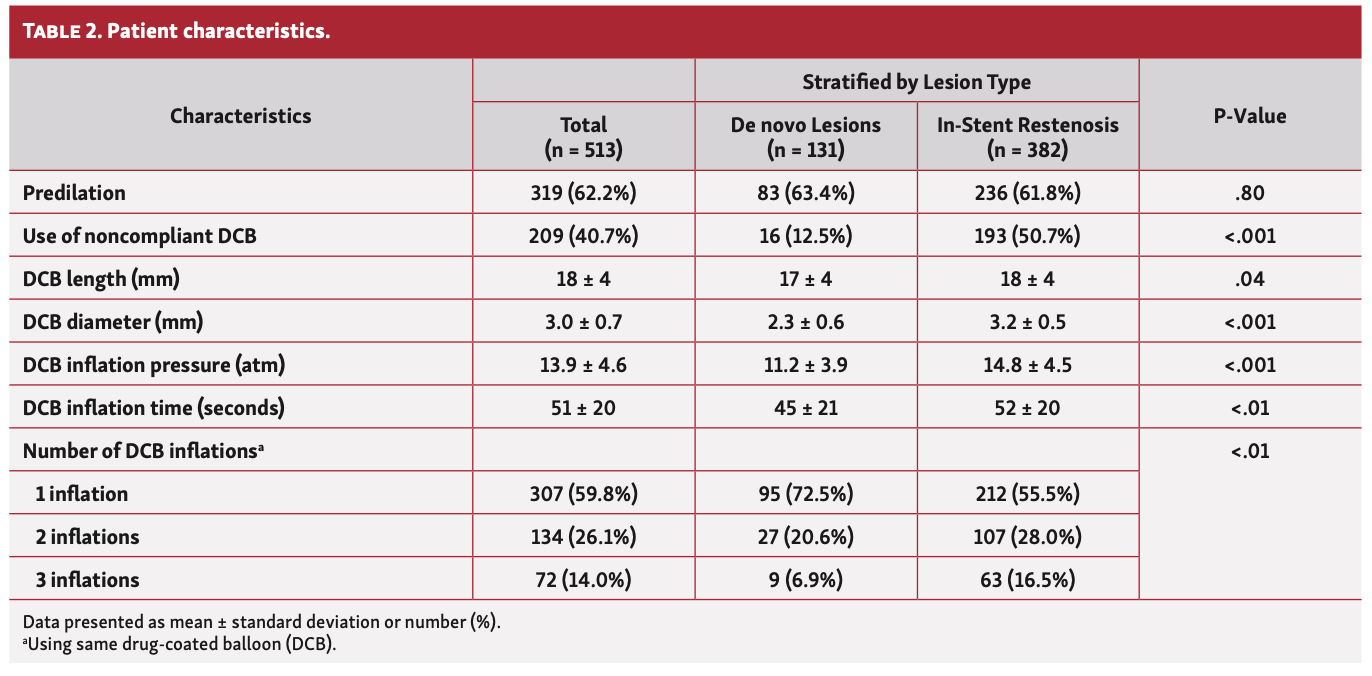
The DCB was primarily used for ISR in 382 patients and for treatment of de novo lesions in 131 patients. Significant differences in baseline and procedural characteristics were observed between these patient groups. Patients treated for ISR had a higher cardiovascular risk profile, with older age, more hypertension, more hypercholesterolemia, more previous myocardial infarction, and more previous coronary artery bypass grafting, and presented more often with acute coronary syndrome (Table 1). Furthermore, the primary target lesion for the DCB was more often identified as the culprit lesion; lesions were longer and had a larger reference diameter in the ISR group. For the treatment of ISR, the noncompliant version of the DCB was used more often, inflation pressure was higher, inflation time was longer, and multiple inflations using the same DCB occurred more often (Table 2).
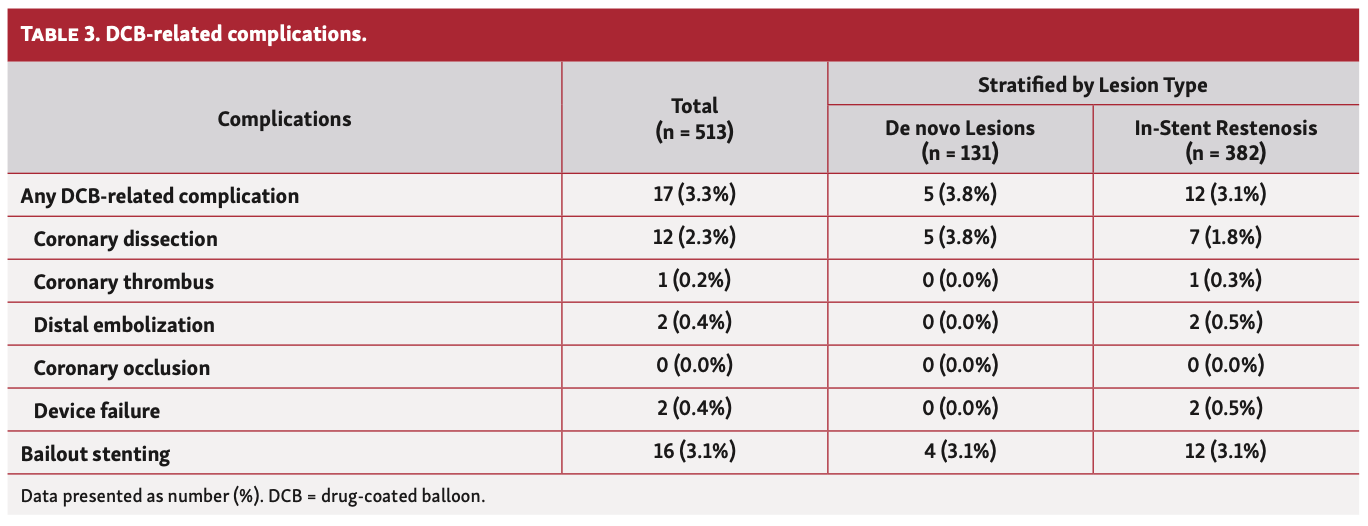
Clinical outcomes. The incidence of DCB-related procedural complications was 3.3% and mostly consisted of coronary dissection (2.3%) (Table 3). Device failure occurred in 2 patients, both because of balloon rupture. Bailout stenting was required in 3.1% of patients. Final angiographic and clinical success was achieved in all patients. No MACE occurred during the index procedure.
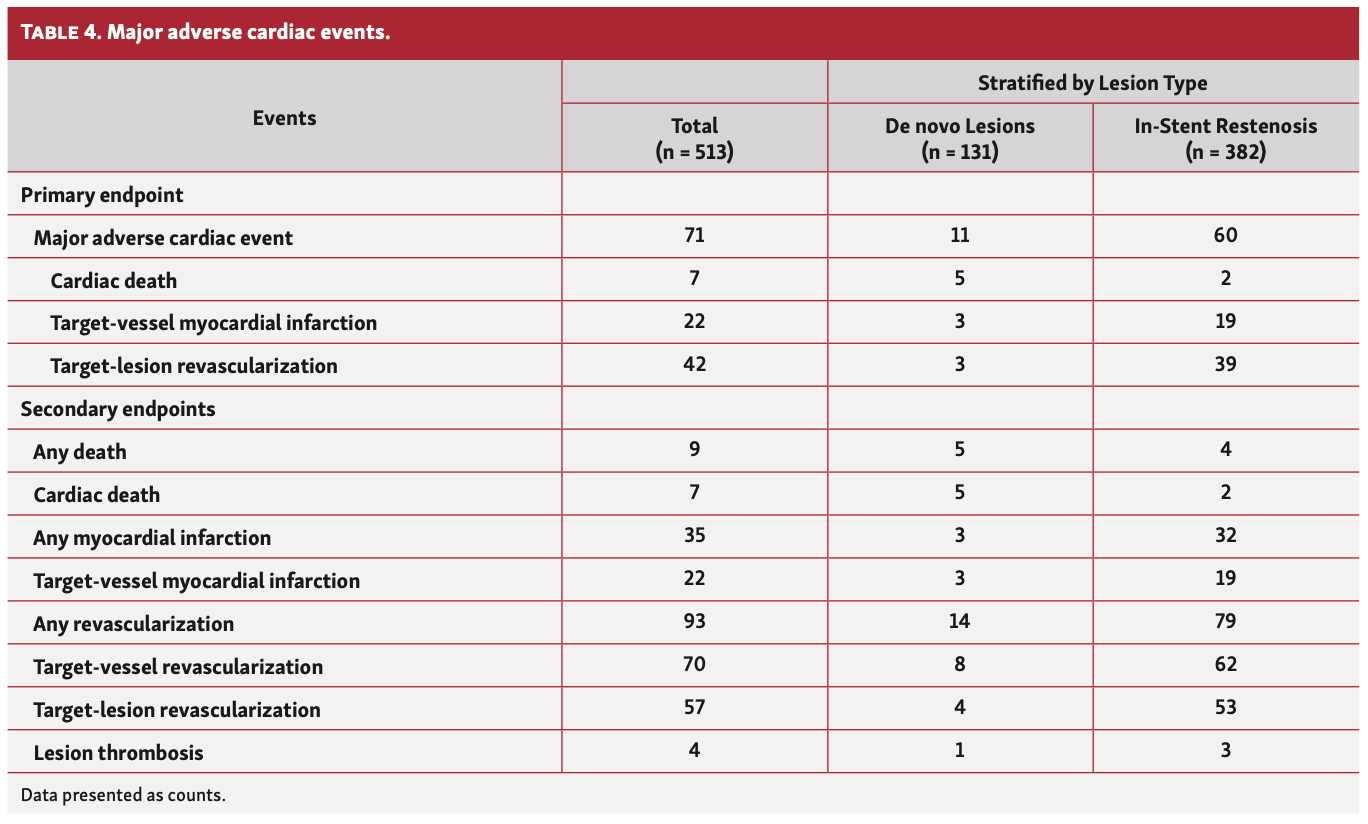
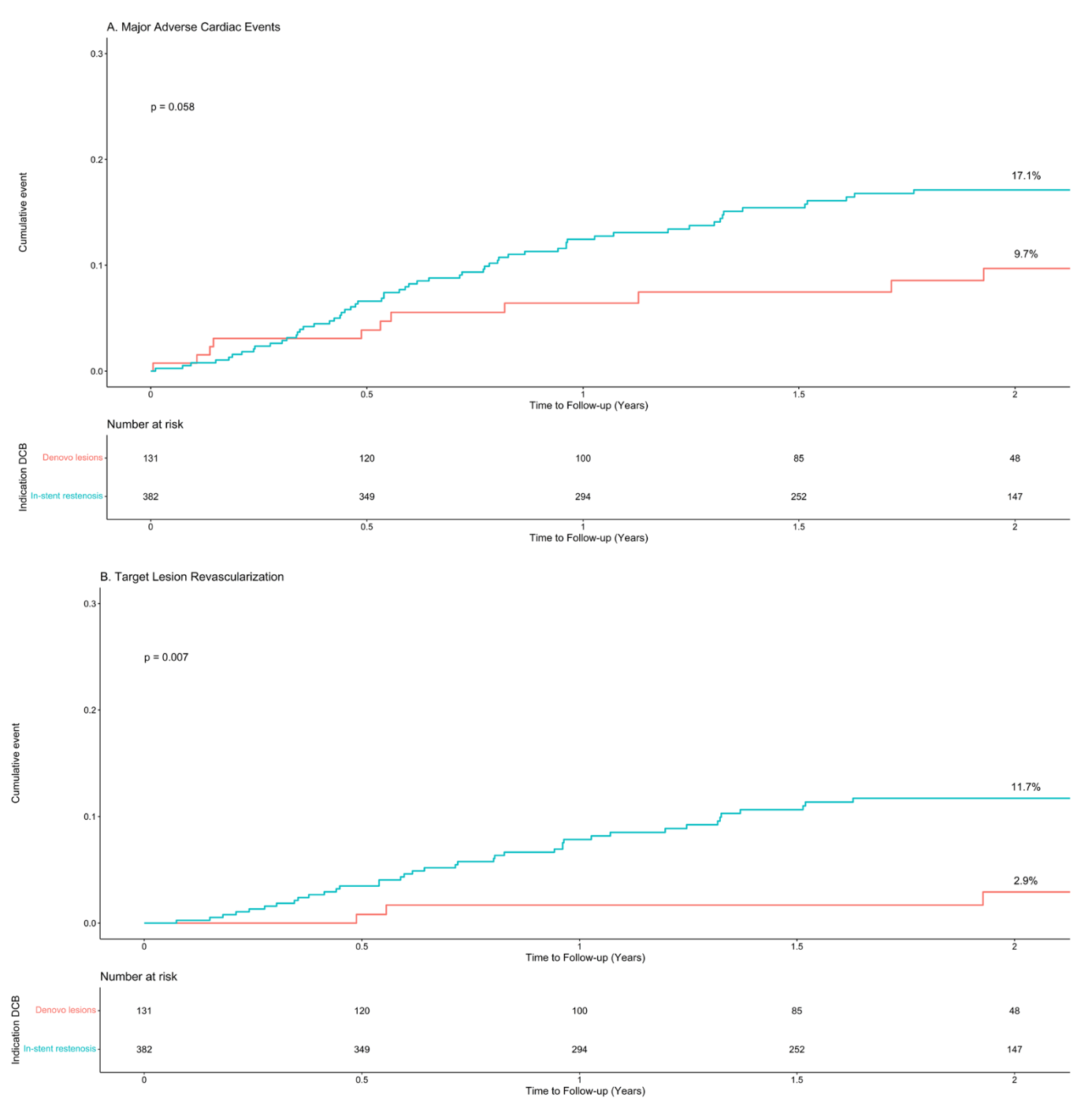
The mean follow-up time was 1.75 years. During follow-up, 71 patients had at least 1 event (Table 4). The cumulative Kaplan-Meier incidence of 2-year MACE was 17.1% in patients treated for ISR and 9.7% in patients treated for de novo lesions (Figure 1). MACE was mainly driven by target-lesion revascularization in patients treated for ISR (11.7%), which was significantly higher than in patients treated for de novo lesions (2.9%; P<.01).
Predictors of major adverse cardiac events. In patients treated for ISR, a history of coronary artery bypass grafting (HR, 1.85; 95% CI, 1.14-2.99; P=.01) and lesion length (HR, 1.02 per mm; 95% CI, 1.00-1.03; P<.01) were associated with higher incidence of MACE during follow-up. Additionally, presentation with acute coronary syndrome (HR, 1.59; 95% CI, 0.96-2.62; P=.07) and high lesion complexity (AHA/ACC lesion type B2/C: HR, 1.63; 95% CI, 0.93-2.83; P=.09) also tended toward higher incidence of MACE, although not significantly. After adjustment for patient characteristics, a history of coronary artery bypass grafting (HR, 1.84; 95% CI, 1.11-3.05; P=.02) and lesion length (HR, 1.02 per mm; 95% CI, 1.01-1.04; P<.01) remained significant predictors of MACE. Other baseline and procedural characteristics were not associated with MACE. Specifically, predilation (HR, 0.88; 95% CI, 0.55-1.41), use of the noncompliant version of the DCB, DCB inflation time, and multiple inflations using the same DCB were not associated with MACE.
Discussion
The potential advantage of DCB coronary angioplasty over stent implantation includes the lack of leaving a permanent implant, while a quick and homogeneous release of the antiproliferative drug to the vessel wall attenuates the process of neointimal hyperplasia. The lack of leaving a permanent implant is especially relevant in recurrent ISR and in small coronary vessels. Most of the DCB studies have been performed for these indications.2 Consequently, the role of DCBs for the treatment of ISR is acknowledged in the 2018 European Society of Cardiology/European Association for Cardio-Thoracic Surgery (ESC/EACTS) guidelines on myocardial revascularization with a class I (level of evidence A) recommendation.1 The rationale for using DCBs is based on the concept that with highly lipophilic drugs, even short contact times between the balloon surface and the vessel wall are sufficient for effective drug delivery.1 Paclitaxel, a highly lipophilic, antiproliferative, and chemically stable drug after tissue delivery, is still the most commonly used drug, while sirolimus has more recently been investigated.4 A recent propensity-matched comparison between paclitaxel- and sirolimus-coated balloons did not find significant differences in MACE at 12 months of follow-up.5
ISR in drug-eluting stents is histologically different from restenosis in bare-metal stents, with different phenotypes of smooth muscle cells proliferating at a low rate.6 On the basis of randomized trial data published in a large meta-analysis, DCBs are similarly effective as drug-eluting stents in the reduction of revascularization for bare-metal stent ISR, whereas they have somewhat lower efficacy in drug-eluting stent ISR.7 The reported incidence of target-lesion revascularization after DCB angioplasty for drug-eluting stent ISR was approximately 15% at 2 years of follow-up.7 Interestingly, in our study, DCB angioplasty was also mainly performed for drug-eluting stent ISR and the incidence of target-lesion revascularization still seems to be slightly lower (11.7%). This observation is even more intriguing given the fact that our data reflect everyday clinical practice, and not a carefully selected randomized controlled trial population. The latter is usually associated with lower event rates.
PCI of lesions in small coronary vessels remains challenging. In small-diameter vessels, the late lumen loss occupies a higher percentage of the respective vessel diameter, leading to higher rates of ISR and clinical events.2,8 The BASKET-SMALL 2 study and the RESTORE SVD study showed that DCB angioplasty resulted in similar MACE rates compared with drug-eluting stent implantation.9,10 The reported incidences of MACE during 1-year of follow-up were 8% and 9.6%, respectively. In our study, the MACE rate at 2 years after DCB angioplasty for de novo lesions was 9.7%.
A previous study has shown that angiographically inadequate lesion preparation before DCB treatment was an independent predictor of target-lesion revascularization.11 However, since the Protégé DCB is also available in a noncompliant version, it was hypothesized that predilation of the lesion may not always be necessary. This hypothesis was confirmed by our finding that lack of predilation was not associated with MACE in this study.
The large sample size and prospective follow-up of an all-comers, routine clinical care population are among the strengths of the current analysis of the PEARL registry. The 2-year follow-up results provides additional value. Although the pooled DAEDALUS analysis reported 3-year follow-up,7 it has to be emphasized that only ISAR-DESIRE 3 (Intracoronary Stenting and Angiographic Results Drug Eluting Stent In-Stent Restenosis: 3 Treatment Approaches) with 61 patients and RIBS IV (Restenosis Intra-Stent of Drug-Eluting Stents: Drug-Eluting Balloons vs Everolimus-Eluting Stents) with 133 patients actually provided 3-year outcomes.12,13 Consequently, the need for follow-up data on DCB results beyond 1 year of follow-up has been advocated.
Study limitations. Some limitations of this study must be acknowledged. First, intravascular imaging as recommended by the ESC/EACTS guidelines1 was not routinely applied for the evaluation of the mechanism of drug-eluting stent ISR or for the evaluation of the final result after the DCB in our registry of routine clinical care. Second, nonrandomized, real-world registries are potentially subject to bias and confounding factors, problems that are controlled in randomized, blinded trials. However, real-world registries more accurately reflect the setting of everyday clinical practice and therefore our study has a broader generalizability compared with randomized, controlled trials. Finally, stratified analyses were performed on patients treated for ISR and patients who were treated for de novo lesions because of significant heterogeneity. This has resulted in a smaller subgroup sample size, especially in the de novo lesion group. Because of this smaller subgroup sample size, we were not able to assess the predictors of MACE in patients treated for de novo lesions.
Conclusion
This real-world registry shows that the Protégé paclitaxel DCB is safe and effective for PCI of ISR and de novo lesions. The patients in the registry had a high cardiovascular risk profile, including frequent presentation with acute coronary syndrome and with the majority of the lesions classified as highly complex. Nevertheless, 2-year clinical outcome was favorable, with a MACE rate of 17.1% in patients treated for ISR and 9.7% in patients treated for de novo lesions.
Affiliations and Disclosures
From the 1Albert Schweitzer Hospital, Department of Cardiology, Dordrecht, The Netherlands; 2Amphia Hospital, Department of Cardiology, Breda, The Netherlands; 3Jeroen Bosch Hospital, Department of Cardiology, Den Bosch, The Netherlands; 4Zuyderland Hospital, Department of Cardiology, Heerlen, The Netherlands; and 5Erasmus MC, Department of Cardiology, Rotterdam, The Netherlands.
Disclosure: The authors have completed and returned the ICMJE Form for Disclosure of Potential Conflicts of Interest. The authors report no conflicts of interest regarding the content herein.
Manuscript accepted October 13, 2021.
Address for correspondence: Alexander J.J. IJsselmuiden, MD, PhD, Amphia Hospital, Department of Cardiology, Breda, The Netherlands. Email: sijsselmuiden@amphia.nl
Related Articles
- Two-Year Clinical Outcomes of the REVELATION Study: Sustained Safety and Feasibility of Paclitaxel Coated Balloon Angioplasty Versus Drug-Eluting Stent in Acute Myocardial Infarction
- Paclitaxel Drug-Coated Balloon After Bare-Metal Stent Implantation, an Alternative Treatment to Drug-Eluting Stent in High Bleeding Risk Patients (The Panelux Trial)
- Paclitaxel Drug-Coated Balloon for the Treatment of De Novo Small-Vessel and Restenotic Coronary Artery Lesions: 12-Month Results of the Prospective, Multicenter, Single-Arm PREVAIL Study
References
1. Neumann FJ, Sousa M, Ahlsson A, et al. 2018 ESC/EACTS Guidelines on myocardial revascularization. Eur Heart J. 2019;40(2):87-165. doi:10.1093/eurheartj/ehy394
2. Jeger RV, Eccleshall S, Wan Ahmad WA, et al. Drug-coated balloons for coronary artery disease: third report of the International DCB Consensus Group. JACC Cardiovasc Interv. 2020;13(12):1391 -1402. doi:10.1016/j.jcin.2020.02.043
3. Vlieger S, Cheng JM, Dello S, et al. Interim analysis of the Protégé paclitaxel-eluting balloon in real-world practice (PEARL) registry. Clin Cardiol Cardiovasc Interv. 2021;4(3):1-2. doi:10.31579/2641-0419/133
4. Cortese B, Testa L, Di Palma G, et al. Clinical performance of a novel sirolimus-coated balloon in coronary artery disease: EASTBOURNE registry. J Cardiovasc Med (Hagerstown). 2021;22(2):94-100. doi:10.2459/JCM.0000000000001070
5. Cortese B, Caiazzo G, Di Palma G, De Rosa S. Comparison between sirolimus and paclitaxel-coated balloon for revascularization of coronary arteries. The SIRPAC (SIRolimus-PAClitaxel) study. Cardiovasc Revasc Med. 2021;28:1-6. Epub 2021 Apr 17. doi:10.1016/j.carrev.2021.04.013
6. Chieffo A, Foglieni C, Nodari RL, et al. Histopathology of clinical coronary restenosis in drug-eluting versus bare metal stents. Am J Cardiol. 2009;104(12):1660-1667. doi:10.1016/j.amjcard.2009.07.041
7. Giacoppo D, Alfonso F, Xu B, et al. Paclitaxel-coated balloon angioplasty vs. drug-eluting stenting for the treatment of coronary in-stent restenosis: a comprehensive, collaborative, individual patient data meta-analysis of 10 randomized clinical trials (DAEDALUS study). Eur Heart J. 2020;41(38):3715-3728. doi:10.1093/eurheartj/ehz594
8. Biondi-Zoccai G, Moretti C, Abbate A, Sheiban I. Percutaneous coronary intervention for small vessel coronary artery disease. Cardiovasc Revasc Med. 2010;11(3):189-198. doi:10.1016/j.carrev.2009.04.007
9. Jeger RV, Farah A, Ohlow MA, et al. Drug-coated balloons for small coronary artery disease (BASKET-SMALL 2): an open-label randomised non-inferiority trial. Lancet. 2018;392(10150):849-856. doi:10.1016/S0140-6736(18)31719-7
10. Tang Y, Qiao S, Su X, et al. Drug-coated balloon versus drug-eluting stent for small-vessel disease: the RESTORE SVD China randomized trial. JACC Cardiovasc Interv. 2018;11(23):2381-2392. doi:10.1016/j.jcin.2018.09.009
11. Tanaka A, Latib A, Jabbour RJ, et al. Impact of angiographic result after predilatation on outcome after drug-coated balloon treatment of in-stent coronary restenosis. Am J Cardiol. 2016;118(10):1460-1465. doi:10.1016/j.amjcard.2016.08.006
12. Kufner S, Cassese S, Valeskini M, et al. Long-term efficacy and safety of paclitaxel-eluting balloon for the treatment of drug-eluting stent restenosis: 3-year results of a randomized controlled trial. JACC Cardiovasc Interv. 2015;8(7):877-884. doi:10.1016/j.jcin.2015.01.031
13. Alfonso F, Perez-Vizcayno MJ, Cuesta J, et al. 3-year clinical follow-up of the RIBS IV clinical trial: a prospective randomized study of drug-eluting balloons versus everolimus-eluting stents in patients with in-stent restenosis in coronary arteries previously treated with drug-eluting stents. JACC Cardiovasc Interv. 2018;11(10):981-991. doi:10.1016/j.jcin.2018.02.037














{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}