


Prophylactic Foot Surgery In Patients With Diabetes: Is It Worth The Risk?
Lower extremity complications associated with diabetes present a special challenge to any physician contemplating surgical management. Prophylactic foot surgery can be described as a procedure to prevent ulceration or re-ulceration in patients with diabetes without significant vascular compromise. This concept is part of a larger classification system, which stratifies the risks associated with various types of foot surgery.1 Why and when would you consider prophylactic surgery? A history of previous ulceration and/or amputation is an important consideration when assessing a patient for prophylactic surgery.2 Patients with diabetes are clearly at a higher risk for non-traumatic lower extremity amputation if they exhibit peripheral neuropathy, structural deformity, vascular disease, ulceration and infection.3 Patients with peripheral neuropathy and structural deformity without critical limb ischemia may be candidates for prophylactic intervention. The annual incidence of diabetic ulceration is between 5 and 7.5 percent when neuropathy is present.4 Peripheral neuropathy and mechanical stress play central roles in diabetic foot ulcerations. Components of distal symmetric polyneuropathy include sensory and motor neuropathy. Motor neuropathy may lead to bony deformities such as hammertoes with areas of high pressure. When combined with limited joint mobility, these areas can eventually become pre-ulcerative sites with the potential for skin breakdown. Patients are unable to detect any discomfort in these areas due to the loss of protective sensation. As a result, repetitive pressure leads to local ischemic necrosis.4,5 Although researchers have shown that therapeutic shoes can be effective in reducing the recurrence rates of ulcers in patients with diabetes, these rates can range from 28 percent at 12 months to 100 percent at 40 months.6,7 When attempts at conservative therapy fail, one should consider surgical intervention.
Pertinent Advice From Classification Systems On Diabetic Foot Surgery
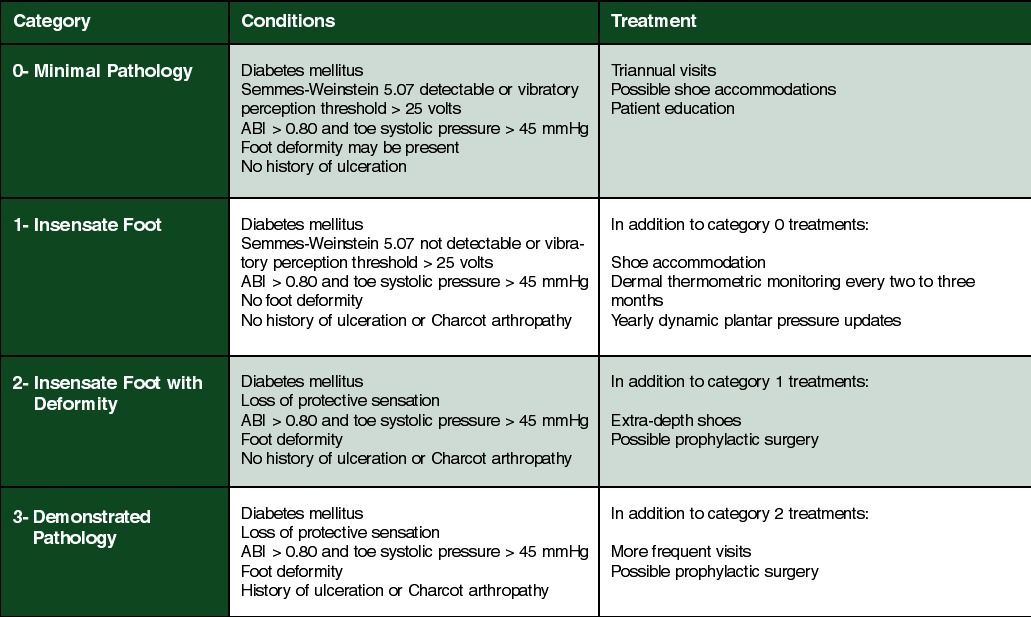
Armstrong and Frykberg published the following risk-based classification system for foot surgery in patients with diabetes.1 Class I: Elective. This procedure alleviates pain or limitation of motion in people without a loss of protective sensation. There is a very low risk of a high-level amputation. Class II: Prophylactic. This reduces the risk of ulceration or re-ulceration in a patient with a loss of protective sensation but without an open wound. There is a low risk of high-level amputation. Class III: Curative. This procedure assists in healing an open wound and carries a moderate risk of a high-level amputation. Class IV: Emergent. This procedure limits the progression of an acute infection and carries a high risk of high-level amputation. Armstrong, et al., also published a treatment-based classification system for the diabetic foot.2 (See “A Guide To Treatment Options For The Diabetic Foot” below) Within this classification system, physicians may consider prophylactic surgery for patients who have an insensate foot with deformity (category 2 patients) or those who have demonstrated pathology (category 3 patients). Both categories share the presence of sensory neuropathy, foot deformity and adequate vascular supply (ankle brachial index >0.80 and toe systolic pressure > 45 mmHg). However, category 3 patients have a previous history of ulceration and/or Charcot joint.
What The Literature Reveals About Prophylactic Surgery
Researchers have investigated various types of prophylactic surgery including digital arthroplasty, flexor tenotomy, tendo-Achilles lengthening (TAL), exostectomy and first metatarsophalangeal joint (MPJ) arthroplasty.8-13 In one study, researchers found that the TAL procedure reduced the ulcer recurrence rate by 75 percent at seven months and 52 percent at two years in comparison to conservative treatment.11 Flexor tenotomies for clawtoe deformity yielded favorable results in healing and preventing the recurrence of distal ulcers.9,10 In a randomized controlled study of non-infected neuropathic ulcers, surgical intervention reduced the re-ulceration rate to 14 percent whereas conservative treatment resulted in a re-ulceration rate of 42 percent at the six-month follow-up.12 In a study by Armstrong, et al., digital arthroplasty procedures in diabetic and non-diabetic patients showed no significant difference in postoperative infection rates and the recurrence of ulcers at the six-month follow-up.8 In patients with hallux interphalangeal joint wounds, however, Armstrong, et al., showed a significantly lower ulcer recurrence rate with surgical treatment (4.8 percent) in comparison to conservative treatment (35 percent) at the six-month follow-up.13 Despite some reported favorable outcomes, there are needs for more randomized clinical trials aimed at procedure specific results and long-term data in order to further elucidate clinical efficacy.
Case Study One: When A Diabetic Patient Has A Hammertoe Deformity
A 45-year-old woman with a past medical history of type 2 diabetes, hypertension and coronary artery disease underwent treatment for hammertoes of her right foot. Despite serial debridements and proper shoes, her digital deformities continued to show no improvement around the pre-ulcerative sites. The second digit did ulcerate to full thickness but did not involve the joint or the bone. Once the ulceration was healed, I performed proximal interphalangeal joint arthroplasties. The patient showed no signs of mechanical stress on the toes a year after the procedure.
Case Study Two: When A Diabetic Patient Has Distal Preulcerative Lesions
A 60-year-old woman with a past medical history of type 1 diabetes, peripheral neuropathy and distal bypass received treatment for recurrent callus formation at the distal end of the toes of her right foot. She developed this contracture following a traumatic incident to her anterior and lateral leg several years ago. In addition to quarterly visits for palliative foot care, she received ankle foot orthoses and custom-made shoes with inserts. Despite the conservative efforts, the distal pre-ulcerative sites showed no significant improvement. I performed prophylactic surgery to correct the rigid deformity. One year after the procedure, the patient continues to wear her accommodative shoes and does not show any signs of skin irritation at the distal ends of the digits.
In Conclusion
Prophylactic foot surgery is a relatively new concept that has received greater attention in the last 10 years. In regard to this type of surgery, our goals are reducing mechanical stress on bony areas and preventing ulceration. For each patient, one must weigh the risks and benefits before rendering any invasive treatment. A clearer understanding of risk factors associated with diabetes has led to several classification systems that may provide the foundation for clinical guidelines and future research. Several studies have shown promising results that prophylactic foot surgery may be safe and effective in preventing recurrent foot ulcerations. Dr. Baek is in private practice at Laurel Lake Foot and Ankle Center in Laurel, Md. Dr. Baek is an Associate of the American College of Foot and Ankle Surgeons, and is a member of the American Podiatric Medical Association. Dr. Steinberg is an Assistant Professor in the Department of Plastic Surgery at the Georgetown University School of Medicine in Washington, D.C. Dr. Steinberg is a Fellow of the American College of Foot and Ankle Surgeons.
References:
1. Armstrong DG, Frykberg RG. Classifying diabetic foot surgery: toward a rational definition. Diabet Med. 2003 Apr; 20(4): 329-31.
2. Murray HJ, Young MJ, Hollis S, Boulton AJ. The association between callus formation, high pressures and neuropathy in diabetic foot ulceration. Diabet Med. 1996 Nov; 13(11): 979-82.
3. Armstrong DG, Lavery LA, and Harkless LB. Treatment-based classification system for assessment and care of diabetic feet. J Am Podiatr Med Assoc 1996 86: 311-316.
4. Boulton AJ, Kirsner RS, Vileikyte L. Clinical practice. Neuropathic diabetic foot ulcers. N Engl J Med. 2004 Jul 1; 351(1): 48-55.
5. Giacalone VF, Krych SM, Harkless LB. The University of Texas Health Science Center at San Antonio: experience with foot surgery in diabetics. J Foot Ankle Surg. 1994 Nov-Dec; 33(6): 590-7.
6. Cavanagh PR, Lipsky BA, Bradbury AW, Botek G. Treatment for diabetic foot ulcers. Lancet. 2005 Nov 12;366(9498):1725-35.
7. Busch K and Chantelau E. Effectiveness of a new brand of stock ‘diabetic’ shoes to protect against diabetic foot ulcer relapse. A prospective cohort study. Diabetic Medicine 2003 20(8):665–669.
8. Armstrong DG, Lavery LA, Stern S, Harkless LB. Is prophylactic diabetic foot surgery dangerous? J Foot Ankle Surg. 1996 Nov-Dec;35
9. Tamir E, McLaren AM, Gadgil A, Daniels TR. Outpatient percutaneous flexor tenotomies for management of diabetic claw toe deformities with ulcers: a preliminary report. Can J Surg. 2008 Feb;51(1):41-4.
10. Laborde JM. Neuropathic toe ulcers treated with toe flexor tenotomies. Foot Ankle Int. 2007 Nov;28(11):1160-4.
11. Mueller MJ, Sinacore DR, Hastings MK, Strube MJ, and Johnson JE. Effect of Achilles tendon lengthening on neuropathic plantar ulcers: a randomized clinical trial. J Bone Joint Surg Am. 2003;85:1436-1445
12. Piaggesi A, Schipani E, Campi F, Romanelli M, Baccetti F, Arvia C, Navalesi R. Conservative surgical approach versus non-surgical management for diabetic neuropathic foot ulcers: a randomized trial. Diabet Med. 1998 May;15(5):412-7.
13. Armstrong DG, Lavery LA, Vazquez JR, Short B, Kimbriel HR, Nixon BP, Boulton AJ. Clinical efficacy of the first metatarsophalangeal joint arthroplasty as a curative procedure for hallux interphalangeal joint wounds in patients with diabetes. Diabetes Care. 2003 Dec;26(12):3284-7.


{kind=link}
{kind=link}
{kind=link}
{kind=link}