


Assessing Global Ankle Instability
Chronic ankle instability (CAI) is a pathology arising from one of the most common orthopedic injuries, lateral ankle sprains.1 Ankle sprains classically damage the lateral compartment of the tibiotalar and subtalar joints.2 In fact, many clinicians and surgeons likely think of lateral ankle pathology as synonymous with ankle instability. Of the nearly 2 million ankle sprains that present to emergency departments in the United States annually, isolated medial ankle involvement is estimated at ~5%.3-4

However, damage to the medial structures may be underreported.3-6 Some reports mention a combined (lateral and medial/syndesmotic) ligament injury in ~23% of ankle sprains.7 The deltoid, or medial collateral, ligament is a key restraint to lateral and posterior translation of the talus.5 The superficial deltoid elements limit external rotation and the deep deltoid elements prevent eversion.5-6 Hintermann and colleagues were among the first to draw significant attention to medial ankle instability (MAI) over 20 years ago.4,6 This group did not analyze patients with combined medial and lateral ligament damage or instability. Literature regarding MAI has increased substantially in the last 5–10 years.7-11 The majority of the discussion around damage to the deltoid ligament complex focuses on acute injury in ankle fractures or chronic insufficiency in progressive collapsing foot deformity (PCFD).4-5 Renewed interest in deltoid ligament reconstruction in these arenas has likely led to a greater focus on medial ankle instability, although it remains poorly understood.8
With the exception of ankle fractures and end-stage PCFD, isolated MAI without a lateral component is likely rare.8-12 We have proposed that underappreciated MAI is a reason for poor recovery from ankle sprain(s) or failure of lateral ankle ligament surgical procedures.3,13 Combined medial and lateral instability, also termed rotational or global ankle instability (GAI), is a relatively new paradigm that warrants consideration in patients with an acute sprain or chronic instability.
Reviewing the Lateral Ankle Anatomy
Comprehensive details on the lateral ankle ligament complex is beyond the scope of this article but are a necessary understanding in the context of lateral ankle instability (LAI) and GAI. The medial ankle ligamentous complex is not as often categorized due to its less frequently injured nature. This complex is considered the deltoid ligament, talocalcaneal ligament, and calcaneonavicular ligament. The spring ligament plays a fundamental role in stabilization of the medial collaterals. The deltoid ligament consists of 2 deep and 4 superficial components14 as seen in Figure 1.
In a cadaver study of 40 specimens, sectioning of the deep deltoid allowed for an increase of medial clear space to 3.7 mm, compared with less than 2 mm in intact specimens.15 However, more recent cadaveric studies demonstrated equal responsibility of the superficial and deep components for limiting ankle valgus.4,15 One cannot overstate the importance of the medial ligamentous restraint to talar translation eversion. In fact, one study notes that medial ankle sprain progression of osteoarthritis was more rapid than lateral sided injuries.16 Thus, these injuries and their relation to global ankle instability warrants vigilance.
A Guide to Assessing Global Instability
We believe medial ligamentous laxity is overlooked in patients with LAI, and consequently is a reason for lack of improvement after conservative or surgical treatment.3,9-12 Conservative treatment for MAI or GAI is akin to CAI, which includes: rest/ice/compression/elevation principles, physical therapy, peroneal strengthening, proprioceptive training, orthotic modification, bracing and strapping.3 We have found the medial component of GAI may be subtle in comparison to its lateral counterpart. This is in part due to the limited valgus and posterior range of motion (ROM) of the tibiotalar joint versus the wide range seen with compensatory varus.
Given the importance of the medial soft tissue structures of the rearfoot and ankle, any foot and ankle specialist should have a heightened awareness of medial/global ankle instability. Below are our evaluation principles to rule in or out global ankle instability.
Conducting an Effective Clinical Exam
Clinicians should complete the workup for lateral ankle injury or instability as indicated.1-2 Similar patient complaints arise with GAI and include a sensation of “giving out” of the ankle and difficulty with uneven terrain or upward gradients.3,9-11 There may be a remote or acute history of ankle trauma involving an eversion and external rotation mechanism.7 Physical examination should include bilateral assessment of the lower limb while standing, walking, and resting. Localized pain and swelling at the medial ankle or gutter lacks sensitivity and specificity and thus may be unreliable.8,10-11 The patient may complain of pain at the anteromedial ankle joint.
Radiation from the lateral ankle could be subfibular impingement from hindfoot valgus with or without lateral ligament impairment. Any significant deformity warrants exploration. In chronic MAI and GAI, hindfoot valgus deformity is more likely to be seen as a cause of deltoid insufficiency. In the case of PCFD, corrective osteotomies or arthrodeses will likely be required to balance the foot and avoid ligamentous tension.

As such, one should be privy to posterior tibial tendonitis and syndesmotic injury.11-12 Two causes of reducible medial column collapse may include inadequacy of the posterior tibial tendon or deltoid ligament. If an inversion force remains and a single heel raise results in varus, the culprit is likely the deltoid ligament.10-11 In GAI, Ruiz and Hintermann have also remarked on a “pseudo–hallucis rigidus.”10 They surmise the pseudo–hallux rigidus is a consequence of a flexor hallucis longus hyperactivity as a means of protection against valgus/pronation deformity. Table 1 demonstrates the adapted clinical classification of MAI by Valderrabano and Hintermann.16
How to Conduct Clinical Stress Testing
- The “external rotation test” should be used to assess the integrity of the superficial deltoid ligament (Figure 1).
- The “eversion stress test” should be used to assess the integrity of the deep deltoid ligament.
- The “combined eversion and external rotation stress test” can assess both the deep and superficial deltoid.
- The “anteromedial drawer test” can assess anteromedial subluxation.
- Identical stress testing can also take place under fluoroscopy to visualize potential medial clear space (MCS) widening or ankle valgus.

Insights on Radiographic Evaluation
First and foremost, standard 3-view weight-bearing ankle and foot plain film radiographs are key and should include hindfoot alignment (Saltzman) view(s). Plain films are invaluable to exclude MCS widening, avulsion fragments, syndesmotic lesions/instability, and fractures. Aforementioned stress fluoroscopy is contentious.10-11 Some note positive stress testing at greater than 3 mm of MCS and positive valgus stress at a difference from contralateral ankle of up to 19 degrees.11 Nevertheless, extreme positive lateral and medial findings on stress fluoroscopy are likely diagnostic for GAI.
Ultrasonography is also valuable in assessment of ankle ligaments. A parallel ultrasound probe features ligaments as hyperechoic. In the chronic ankle instability patient, ultrasonography is probably less useful. Up to 93.8% sensitivity and 100% specificity in detection of anterior talofibular ligament (ATFL) tears, even when compared to MRI, has only been verified in the setting of an acute injury.7,12 However, ultrasound enables dynamic assessment of soft tissue and can uncover bony impingement with stress testing. In our practice, we regularly display live ultrasonography to the patients to allow them to visualize their pathology in real time.
Computed tomography (CT) is not infrequently utilized.7-10 CT can identify associated pathologic conditions including but not limited to tibiotalar osteochondral pathologies, ankle osteoarthritis (OA), or hindfoot osteoarthritis. Discovery may lead to diagnostic injections. Symptomatic lesions or OA would change treatment protocol.
In our hands, magnetic resonance imaging (MRI) holds the highest value in the workup for global ankle instability. However, one must appreciate the distinctions between MRI evaluation of medial and lateral ligament morphology. Attenuation and frank tears of the ATFL and calcaneofibular ligament (CFL) are regularly observed; however, multiple studies have noted MRI is not sensitive for an elongated deltoid ligament.14-17 This is problematic because an elongated deltoid is often pathologic and a common criteria for MAI/GAI.13-14
An interesting study by Crim and colleagues reviewed 46 patients with ATFL tears on MRI but negative deltoid findings.15 All patients underwent surgery and 23%, 6%, and 43% had injury to the superficial, deep, or both deltoid components, respectively. Tears of the deltoid on MRI are identified at the origin or insertion.14-17 The proximal origin is most common.7,17

Because of the proximal origin of the deltoid on the medial malleolus, a tear here is typically identified at the level of the tibial plafond on an axial image. Deep deltoid fibers originate posteriorly and thus are better discerned on coronal images.
MRI also allows assessment of the spring ligament complex. Although thin and often difficult to distinguish, particularly on 1.5T MRI, the spring ligament may be perceived in sagittal images. Given these pitfalls, MRI lends itself to a limited sensitivity but high specificity for GAI diagnosis in our practice.
Utilizing Arthroscopy for Ankle Instability
Arthroscopy is a fundamental diagnostic and therapeutic tool in all types of CAI.12-13,16 While its use is routine to identify intra-articular pathology in LAI cases, arthroscopy can assist the diagnosis and treatment of deltoid or GAI pathology.3,15-16 Valderrabano and colleagues also created grading criteria for MAI based on arthroscopic findings (Table 2). At times, arthroscopic examination can detect MAI with negative imaging and clinical inspection.
We begin every case of chronic or global ankle instability with standard arthroscopy. With the patient in a leg holder, we complete typical sterile preparation and draping. After this, a 4.0 mm arthroscope is used through routine anterior portals with an amalgamation of arthroscopic equipment. Accurate diagnosis of GAI can be aided by combining the following arthroscopic findings with the aforementioned evaluation.
Perhaps the most useful arthroscopic sign is the “medial drive-through” sign. Similar to the more common diagnostic “drive-through” sign for shoulder instability, the medial drive-through sign can be applied to the ankle’s medial gutter.18 For this arthroscopic test, one attempts to gently place a 4.0mm shaver into the medial tibiotalar gutter. If there is minimal resistance or the shaver fits, with or without additional space, deltoid ligament insufficiency is likely. Hintermann and colleagues classified clinical lesions into types 1 and 2. This system for gross appearance may also be applied to arthroscopic appearance, where in type 1 instruments can pass partially and pass fully in type 2.4,6-7
The medial collateral ligament fascicles can also be directly visualized with arthroscopy and properly classified. Through the scope portal, the anterior fascicle is viewed at its attachment on the medial malleolus, but cannot be seen at its midportion or talar attachment.13 A Type 1 lesion is characterized by a partial tear or general wavy shape, whereas a Type 2 lesion is a complete injury/tear.19
What You Should Know About the Surgical Technique
We have published the senior author’s preferred technique for global ankle instability, which entails placing the tendon allograft from lateral ligament repair through the talar neck and into the medial malleolus.20
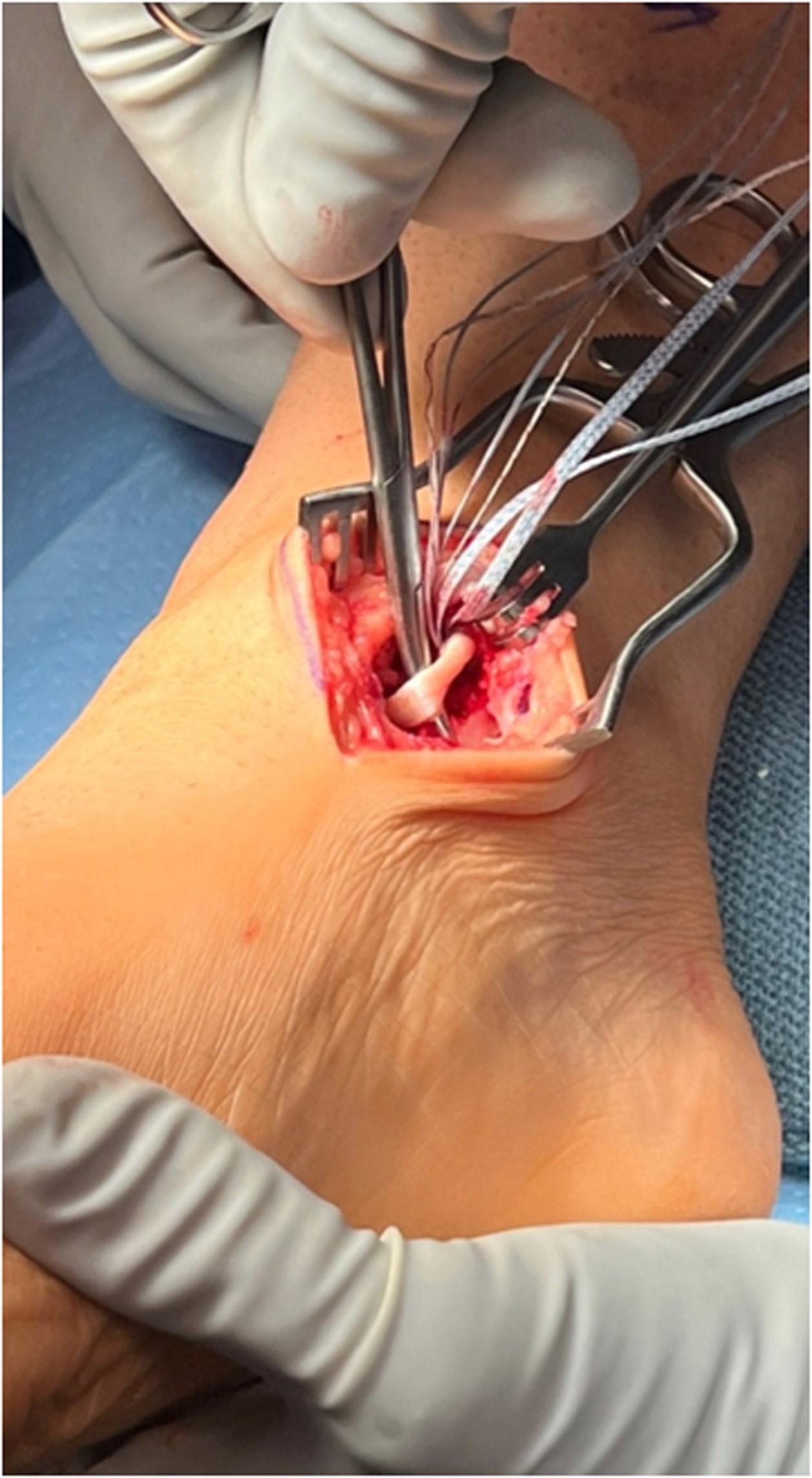
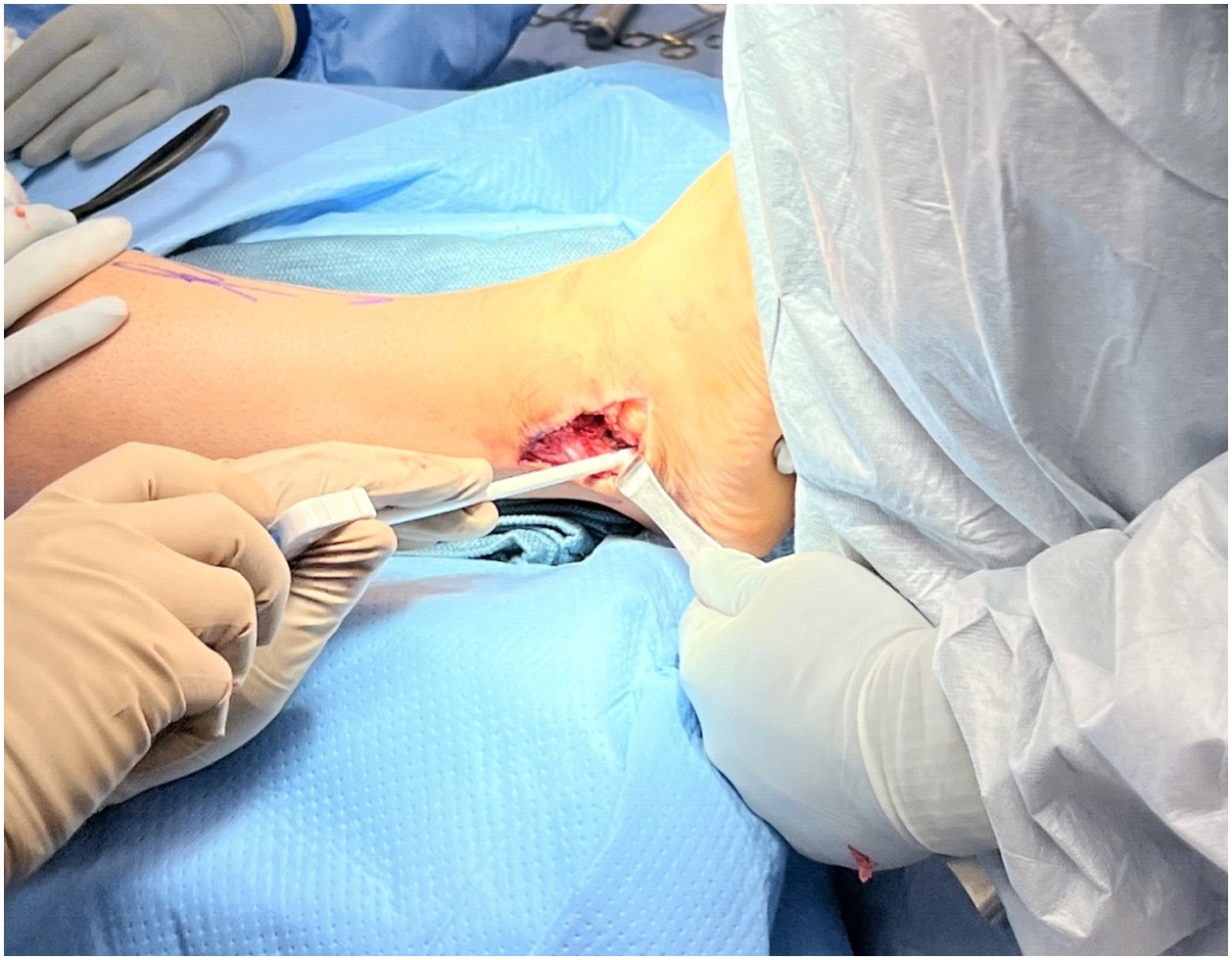
After initial arthroscopic debridement through standard medial and lateral ankle portals to address intra-articular pathology, we make an incision to access the deltoid ligament. Specifically, a 3cm linear incision accesses the medial malleolus, deltoid ligament and medial talar dome. Careful dissection avoids the saphenous vein and nerve. In this case, identification of the deltoid ligament (Figure 1) revealed noticeable hypertrophy and fraying along the anterior fibers. We then split the deltoid ligament transversely with careful dissection off the medial malleolus and medial talar neck. Using a rongeur, we decorticate the distal tip of the medial malleolus and introduce a guide wire to ream a canal for anchor placement. Measurement of the width of the tendon helps determine appropriate reaming diameter moving forward. We advise to ream at the same diameter as the tendon or 0.5mm greater than the diameter.
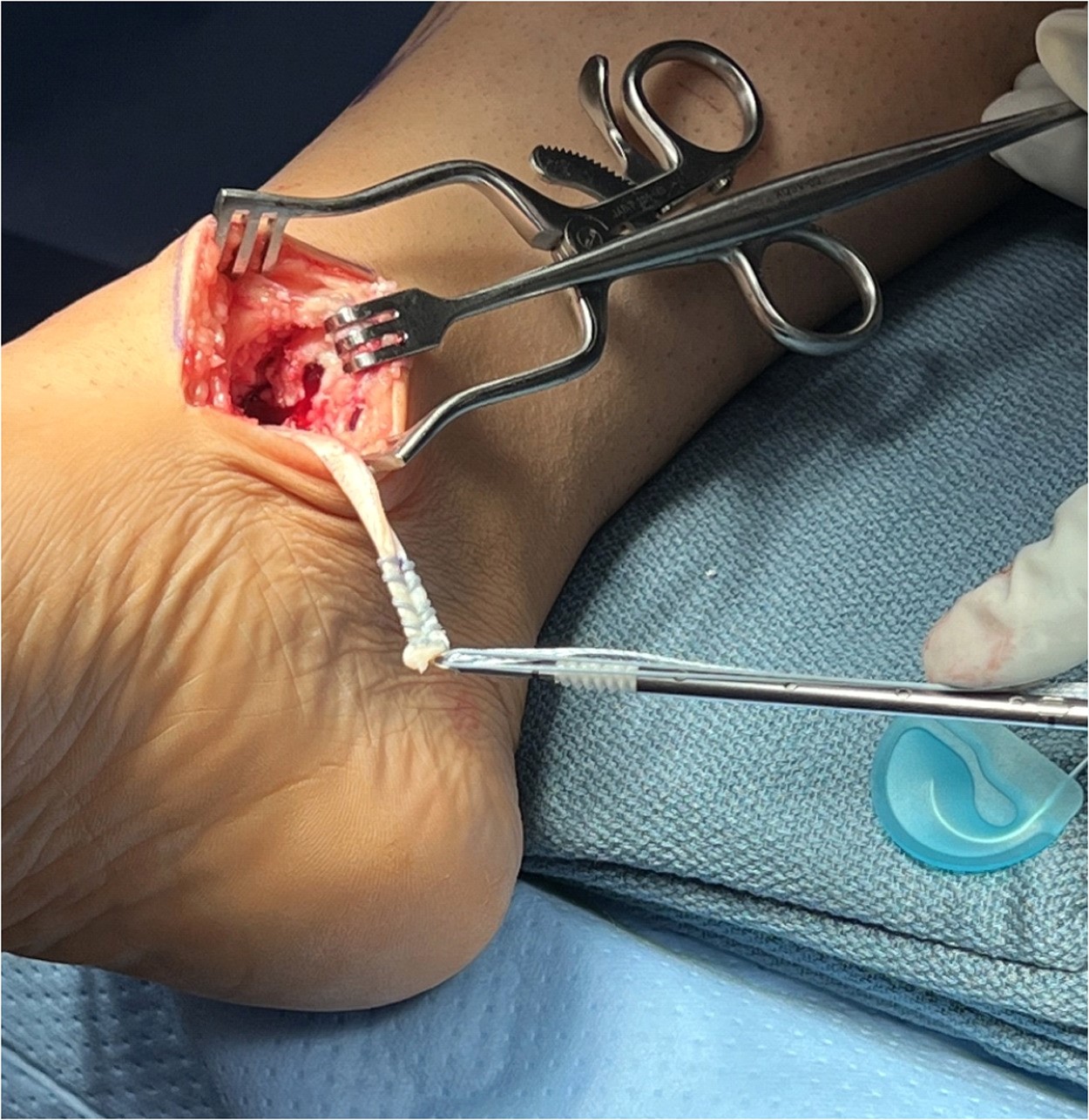
Typically, the allograft measures near 5.0mm, and reaming it done to 5.5mm followed by placement of a Bio-Tenodesis screw (Arthrex) (Figure 2). Then, we placed a Bio-Tenodesis screw with close to 20mm of the allograft tendon buried into the medial malleolar canal (Figure 2). Before moving on to the next stage of the repair, a standard linear incision measuring 4cm allows dissection of the lateral ankle to obtain access to the distal fibula and lateral talus. Care is taken during dissection to avoid the intermediate dorsal cutaneous nerve. After identifying the ATFL, careful dissection through vertical transection of that ligament and the ankle capsule is next, just off the ATFL attachments along the fibula. Careful periosteal dissection carried down through the fibula will reveal its anterior ridge.
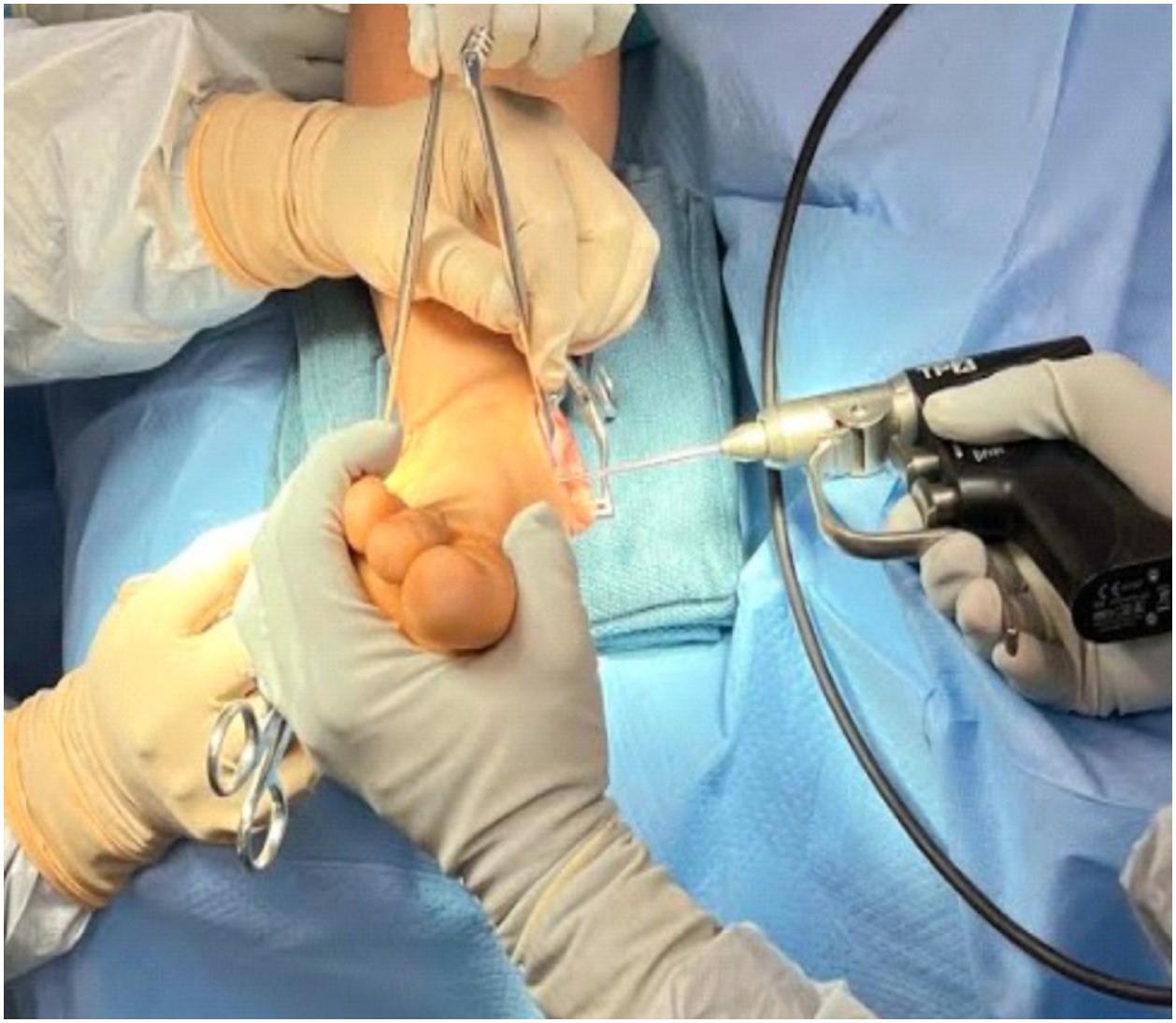
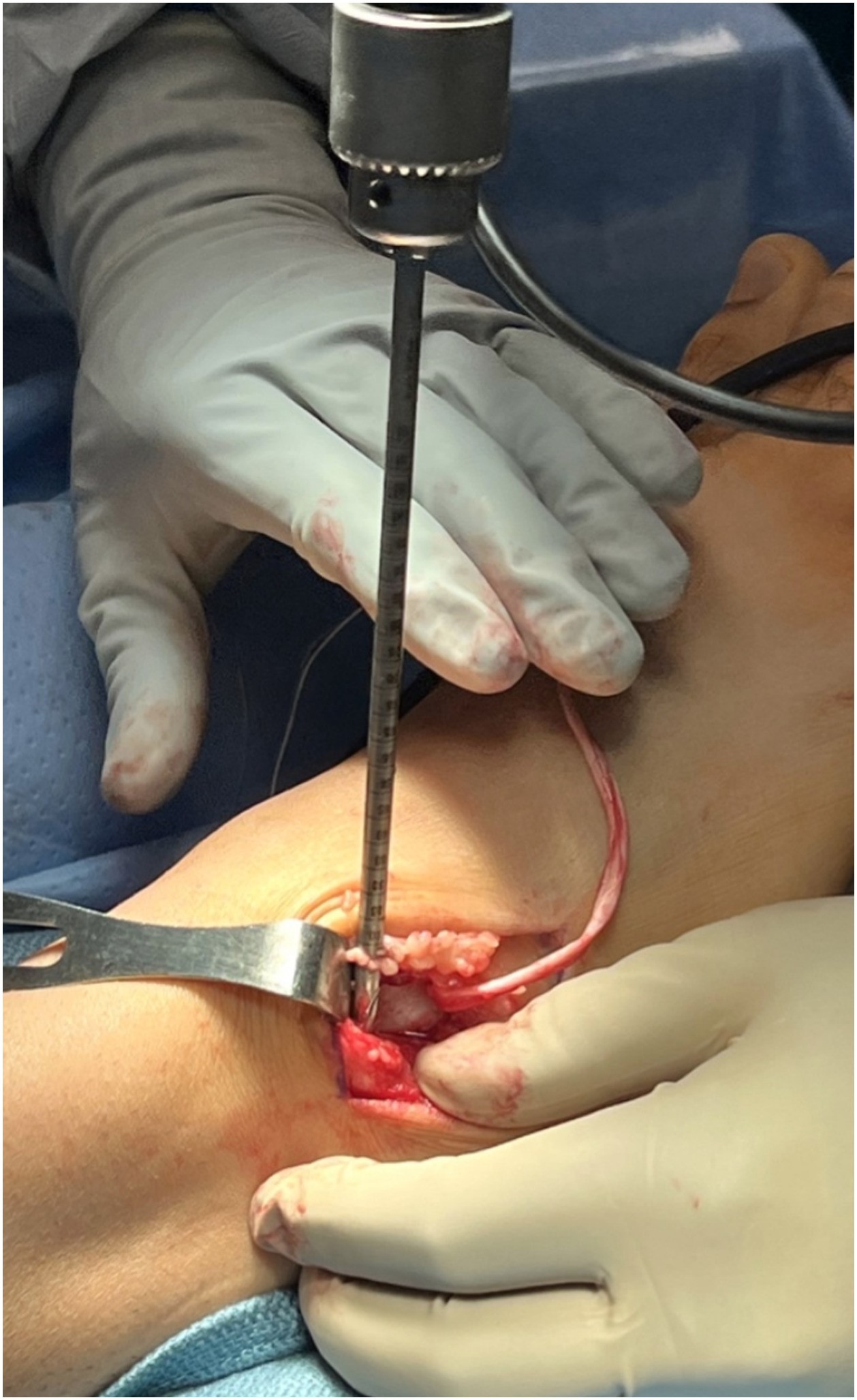
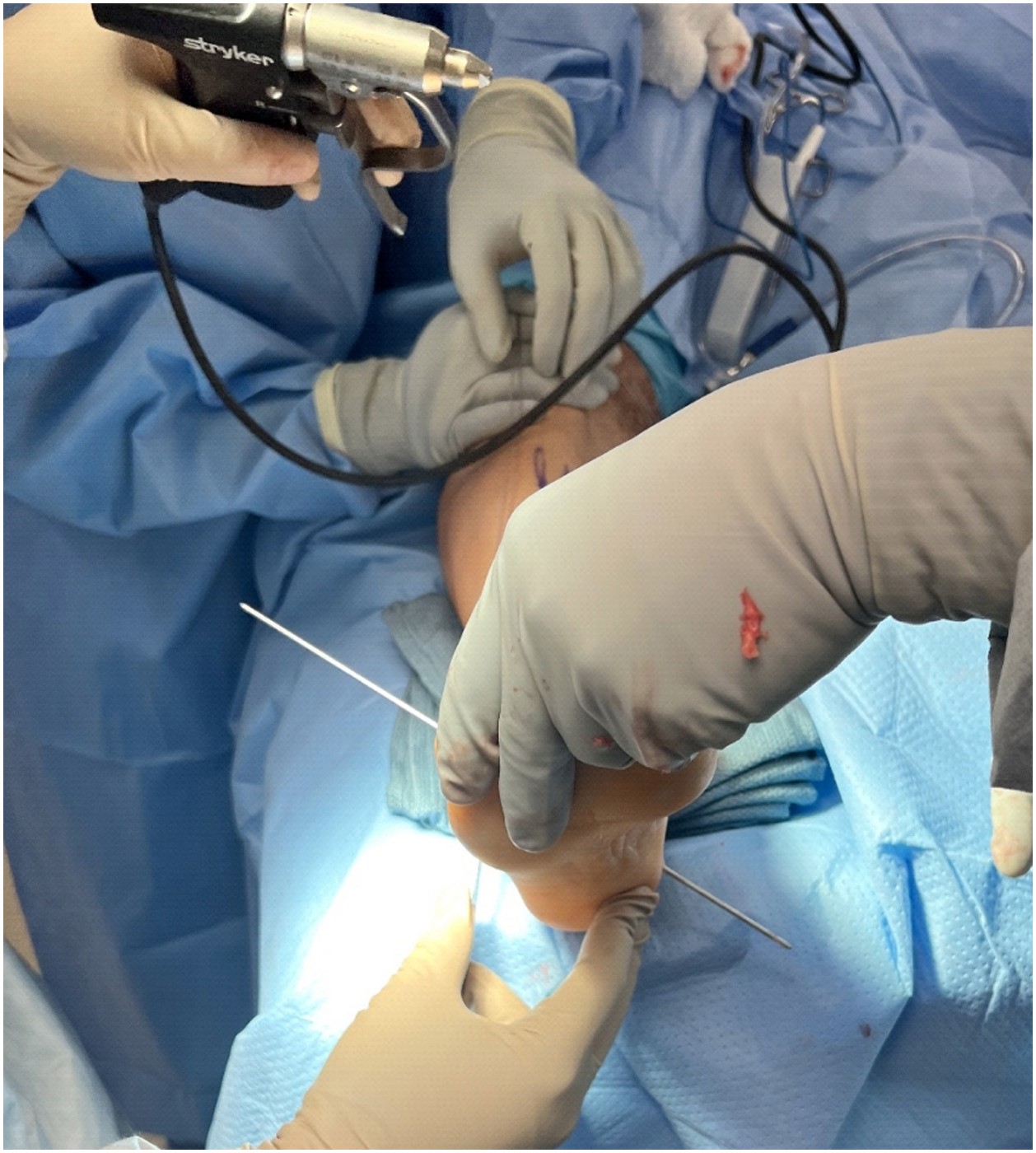
Next, we direct attention to the medial aspect of the talus, where we insert a guide wire for the reamer past the lateral cortex of the talus. The starting place for this wire should be at the junction between the articular dome of the talus and the talar neck. One should also direct this parallel to the weight-bearing surface of the foot (Figure 3). This start point and directionality allows the surgeon to remain in a wide enough portion of the talus to potentially utilize two anchors if necessary. A 5.5mm reamer is again the choice to ream the far cortex of the lateral talus to allow the full allograft to pass in a pull-through technique. Introduction of a 5.5mm anchor into this medial talar canal follows, and we hold the ankle under anatomic tension with the allograft in a taut position during insertion. Deltoid ligament repair in a “pants-over vest” type technique then tightens the once attenuated ligament (Figure 4).
Next we drew our attention to the lateral malleolus at the now decorticated anterior ridge of the fibula. A 5.5mm Bio-Tenodesis screw placed along the lateral talar canal completes the talar involvement of the allograft tendon (Figure 6). We use the standard placement for an anterior fibular anchor in this technique, which is 1–1.5cm proximal from the distal tip of the lateral malleolus and midline to avoid infiltrating the ankle joint. The directionality should be interior without any deviation in the medial-to-lateral direction. A guide wire is placed with these tenets in mind, utilizing one singular tunnel in this technique instead of the two convergent tunnel technique (Figure 7). A 5.5mm reamer then helps create a tunnel from the anterior to posterior fibula, fully through the far cortex, to allow for a pull-through technique. The allograft tendon is now pulled through fully (Figures 6–7). Now we introduce a 5.5mm anchor into the anterior portion of the fibular canal. During insertion of the Bio-Tenodesis screw, one should hold the ankle at anatomic tension while the allograft is held in a taut position. This completes the ATFL portion of the repair (Figure 8).
Finally, the last ligament to reconstruct is the CFL. One identifies and visualizes the subtalar joint and peroneal tendons to avoid during these next steps. The anterior-most portion of the posterior facet of the subtalar joint serves as the insertion site for the guide wire. The surgeon aims this guide wire toward the plantar medial tuberosity of the calcaneal tubercle (Figure 9). This again is reamed with a 5.5mm reamer all the way to the far cortex of the plantar calcaneus. One now passes the allograft tendon in a pull-through technique, and, under anatomic tension, places the final anchor. The CFL has now been repaired. A stab incision is made along the final exit point of the suture and tendon and cut at the level of the skin (Figures 9-10). Postoperative protocol consists of 2 weeks non-weight-bearing in a Jones compression splint followed by 4 weeks of non-weight-bearing in a cast. This equals 6 total weeks of non-weight-bearing, followed by an additional 4 weeks of protected weight-bearing in a tall surgical boot with physical therapy. At 3 months from the date of surgery, the patient may perform activities without limitations.
In Summary
Deltoid ligament injury and medial ankle instability should be in a differential diagnosis for any foot and ankle specialist evaluating an acute ankle sprain or a chronic ankle instability patient failing to improve with conservative care. Combined medial and lateral ankle instability is coined “global” or “rotational” instability. Criteria for global instability are not yet standardized. Patient clinical presentation includes a feeling of the ankle giving way with inversion or eversion and pain over both ankle gutters. Given the medial component, a hindfoot valgus deformity associated with tibialis posterior tendon-muscle pathology is common. In a patient with LAI or an acute sprain, one should have a heightened suspicion for global/rotational instability patterns if there is failure with conservative measures, persistence of clinical instability, increased deformity, and limitation of recreational activities. Reconstruction options are appropriate for the deltoid ligament as discussed elsewhere.20 Corrective osteotomies are more commonly needed with deltoid reconstructive work to reduce strain on the medial ligamentous complex. Any associated injuries should be also addressed.
Dr. Sakkab is a Fellow at Phoenix Foot & Ankle Institute Fellowship in Scottsdale, AZ.
Dr. McAlister is the Program Director at Phoenix Foot & Ankle Institute Fellowship in Scottsdale, AZ.
References
- Hertel J. Functional anatomy, pathomechanics and pathophysiology of lateral ankle instability. J Athl Train. 2002;37(4):364
- Ajis A, Maffulli N. Conservative management of chronic ankle instability. Foot Ankle Clinics. 2006;11(3):531-7.
- Youngblood S, Anderson R, Ellington K, et al. Global ankle instability: clinical and functional assessment at average 26-month follow-up. J Foot Ankle. 2015;9:1-5.
- Hintermann B. Medial ankle instability. Foot Ankle Clin. 2003;8(4):723-38.
- van den Bekerom MP, Mutsaerts EL, et al. Evaluation of the integrity of the deltoid ligament in supination external rotation ankle fractures: a systematic review of the literature. Arch Orthop Traumat Surg. 2009;129:227-35.
- Hintermann B, Valderrabano V, Boss A, et al. Medial ankle instability: an exploratory, prospective study of fifty-two cases. Am J Sports Med. 2004;32(1):183-90.
- Hintermann B, Knupp M, Pagenstert GI. Deltoid ligament injuries: diagnosis and management. Foot Ankle Clin. 2006;11:625-637.
- Alshalawi S, Galhoum AE, Alrashidi Y, et al. Medial ankle instability: the deltoid dilemma. Foot Ankle Clin. 2018;23(4):639-57.
- Savage-Elliott I, Murawski CD, Smyth NA, et al. The deltoid ligament: an in-depth review of anatomy, function, and treatment strategies. Knee Surg Sports Traumatol Arthrosc. 2013;21:1316-27
- Crim JR, Beals TC, Nickisch F, et al. Deltoid ligament abnormalities in chronic lateral ankle instability. Foot Ankle Int. 2011;32(9):873-8.
- Ruiz R, Hintermann B. Clinical appearance of medial ankle instability. Foot Ankle Clin. 2021;26(2):291-304.
- Gopinath R, Pigott M, Lindsey B, et al. Medial ankle instability: review of anatomy, evaluation, and treatment. Foot Ankle Spec. 2022;15(6):573-8.
- Aicale R, Maffulli N. Rotational ankle instability: A current concept review. J Orthop Surg. 2023;31(2):10225536231182347.]
- Milner CE, Soames RW. Anatomy of the collateral ligaments of the human ankle joint. Foot Ankle Int. 1998 Nov;19(11):757-60.
- Rasmussen O, Kromann-Andersen C, Boe S. Deltoid ligament: functional analysis of the medial collateral ligamentous apparatus of the ankle joint. Acta Orthopaedica Scandinavica. 1983 Jan 1;54(1):36-44.
- Valderrabano V, Hintermann B. Diagnostik und Therapie der medialen Sprunggelenkinstabilitat. Arthroskopie. 2005;18:112–8.
- Yu G-R, Zhang M-Z, Aiyer A, et al. Repair of the acute deltoid ligament complex rupture associated with ankle fractures: a multicenter clinical study. J Foot Ankle Surg. 2015;54(2):198–202.
- Gentile MA, Rigby RB, Fleming J, Taylor S, Lamba C. Chronic medial ankle instability medial drive through sign and surgical repair technique. Foot Ankle Surg Tech Reports Cases. 2022;2(3):100225.
- Vega J, Karlsson J, Kerkhoffs GM, DalmauPastor M. Ankle arthroscopy: the wave that’s coming. Knee Surg Sports Traumatol Arthrosc. 2020 Jan;28(1):5-7.
- Duelfer KA, McAlister JE, Bauer R, Warren S. The delta-snook ankle ligament reconstruction for combined deltoid insufficiency and lateral ankle instability. Foot Ankle Surg Tech Reports Cases. 2023 Jun 1;3(2):100292.






{kind=link}
{kind=link}