Early Podiatric Interventions for Patients With Alcohol Use Disorder
Alcohol remains one of the most widely used psychoactive substances in the world. Management of unhealthy drinking habits has been a public health priority for many years.1 In the US, 6.6% of adults engage in heavy drinking, of which 26.2% report at least one episode of binge drinking.2 Routine episodes of binge drinking may lead to alcohol use disorder (AUD), defined as a problematic pattern of alcohol use accompanied by clinically significant impairment or distress.3
Identifying and intervening for risky drinking early on is important to prevent development of an AUD, reduce health care costs, improve the overall mental health of patients, and ultimately prevent death.4,5 Globally, 5.9% of deaths connect to alcohol use. These deaths are typically related to cardiovascular disease, diabetes, injuries, gastrointestinal disease, and cancers.2
Moreover, alcohol use leads to conditions that commonly present in podiatric offices. These include alcohol-induced peripheral neuropathy, gait abnormalities with postural instability, alcohol-induced Charcot neuroarthropathy, traumatic injuries due to imbalance or loss of consciousness, and others.6 As a result, podiatrists will commonly care for those with conditions ranging from risky drinking to severe AUD. Podiatrists should therefore maintain a high clinical suspicion for alcohol use in patients with related podiatric complaints and be able to screen, identify, treat, and refer to a specialist when indicated.
In patients with risky drinking habits, the literature favors a screening and brief intervention (SBI) approach. As potentially the first to intercept these concerns, podiatrists can intervene very early in the course of the patient’s alcohol use. Early interventions carry less stigma and brief interventions over the course of multiple follow-ups allow for repetition and increased efficacy.5 With certain alcohol-related conditions, podiatrists may be the primary or only health care professional seen, putting podiatrists in a unique position to make early and impactful interventions. Additionally, many alcohol-related podiatric complaints—for example, alcohol-induced peripheral neuropathy—may prove reversible early in the course if the alcohol use is decreased or stopped.6
A Closer Look at the Podiatrist’s Role in Risk Stratification
Alcohol use exists on a spectrum from occasional, non-problematic use to risky/problematic use, to an AUD (mild to severe). In health care settings, AUD often goes unrecognized and untreated. When a clinician identifies AUD, typically patients simply receive advice to stop drinking, which by the definition of the disorder is not effective. They may also receive immediate referral to treatment by a specialist, which many patients fail to attend. Many physicians remain hesitant to treat AUD as they feel that patients will report a more severe problem than they are qualified to address. Treatments for AUD involve medications (disulfiram, naltrexone, and acamprosate) in conjunction with a psychosocial program. It is also important to manage comorbid mental health conditions and other use disorders. Hence, it is important for physicians to understand where on the spectrum of alcohol use the patient lies and stratify and act accordingly.
However, immediate referral to specialized treatment may not be suitable for many reasons, including:
1. Patients do not feel their alcohol use is severe enough to receive treatment of this magnitude
2. Patients feel they can control their alcohol use on their own
3. Patients may underestimate the consequences of their drinking and not feel they need treatment
4. Patients may view specialized treatment as a stigmatizing and will be lost to follow-up
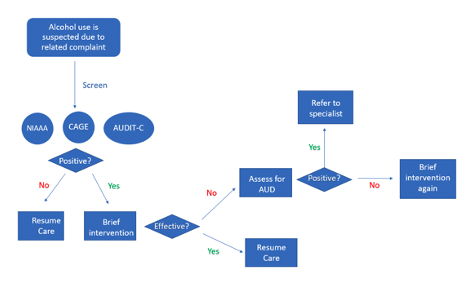
An alternative approach to immediately referring patients for specialized care involves clinicians such as podiatrists playing a greater role. We have created a flowchart of a representative systematic approach (Figure 1). This involves screening for risky drinking, assessing for the presence of an AUD, providing brief interventions and referring to a specialist when indicated.5
Details on a Potential Approach
Screen for risky drinking. To start, one should have a firm understanding of the terminology associated with alcohol use. The goal of obtaining the history should be to identify a screening tool to utilize in practice; use a screening tool, determine the level of risk; assess for AUD; provide brief intervention if indicated; or refer to a specialist if indicated. Three common screening tools are National Institute on Alcohol Abuse and Alcoholism (NIAAA), CAGE, and Alcohol Use Disorders Identification Test-Concise (AUDIT-C). These take less than 3 minutes to complete by either the clinician or patient.
NIAAA. The NIAAA screening tool is an empirically derived tool for identifying those at risk for AUD.7 It is one of the most profound and collective tools focused on Screening, Brief Intervention, and Referral to Treatment (SBIRT). By incorporating SBIRT, it is one of the most useful approaches for the delivery of early interventions and treatment in individuals who are drinking at risky levels and at risk for the development of an AUD. By using the NIAAA screen along with brief intervention, physicians are able to identify and help those at highest risk of developing an AUD. Additionally, there are guidelines and recommendations that practitioners can reiterate in order to successfully guide their patients. Note that a standard drink is defined as any beverage containing 14 grams of pure alcohol (equivalent of 0.6 fluid ounces). Based on the type of drink, the equivalent of standard drink will vary. Twelve ounces of 5% beer, 5 oz of 12% wine and 1.5 oz of 40% liquor are all 1 standard drink.
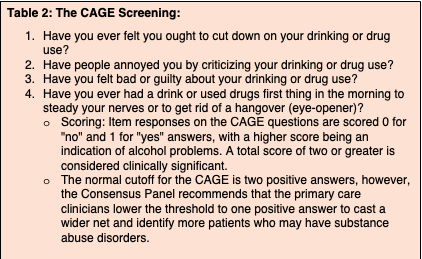
CAGE. The CAGE assessment was first developed by Dr. John Ewing in 1970 to screen patients for AUD. The CAGE assessment is a combination of 4 questions based on the acronym CAGE: Cut down, Annoyed, Guilty, and Eye-opener. The 4 questions are listed in Table 2 (below). The sensitivity for the performance of the CAGE questionnaire in screening patients with current alcohol abuse or dependence was nearly 91%. The probability of a positive result on the CAGE questionnaire that indicated the presence of abuse was under 20%, although the score reached 50% for dependence. In contrast, the negative predictive value (NPV) for CAGE for not presenting alcohol abuse/dependence was more than 90%, reaching 99.2% for abuse.5 Thus, a positive CAGE indicates that either a brief intervention should be initiated, or further questioning is needed to determine the presence of an AUD and to guide treatment recommendations and possible referral to a specialist.
AUDIT-C. The Alcohol Use Disorders Identification Test-Concise (AUDIT-C) is a modified version of the original AUDIT-10 instrument, first developed by the World Health Organization and published in 1998. It is a validated instrument consisting of 3 questions related to alcohol use. The AUDIT-C is scored on a scale of 0–12. Each AUDIT-C question has 5 answer choices ranging from 0 points to 4 points. In men, a score of 4 or more is considered positive, and in women, a score of 3 or more is considered positive. Generally, the higher the score, the more likely it is that a person’s drinking is affecting his or her safety and increasing the likelihood of an AUD.2,9
What are the Criteria for AUD?
A positive screen should prompt clinicians to either initiate a brief intervention or perform a more thorough clinical interview to determine the presence of an AUD. Alcohol use disorder is defined by 11 total criteria, with the number of criteria indicating the severity. The 11 DSM-5 criteria for an AUD are as follows: hazardous use, social or interpersonal problems related to use, neglected major roles to use, withdrawal, tolerance, used larger amounts/longer, repeated attempts to control use or quit, much time spent using, physical or psychological problems related to use, activities given up to use, and craving.
A minimum of 2 of the criteria is necessary to define an AUD. The presence of an AUD or failed attempts at a brief intervention indicate need for specialist referral. Additionally, it is important to recognize the presence of alcohol withdrawal symptoms, which may necessitate Emergency Department referral rather than an outpatient appointment. While waiting for an appointment, patients can be encouraged to attend Alcoholics Anonymous (AA). This is a mutual self-help resource, and many patients derive significant benefit. Hearing stories from others in similar situations could start them on the path to sobriety.
Available Treatment Options
Screening and brief intervention (SBI) is evidence-based and widely utilized for the prevention and early intervention of risky drinking. It consists of utilizing the above screening tools followed by a brief intervention for those who surpass recommended drinking limits.5 It is helpful for the unhealthy use of alcohol and other substances.
When administering SBI, it is important to be aware of stigma, physician bias, and the socioeconomic status (SES) of the patient. Alcohol use disorders are highly stigmatized. To undergo treatment could damage their self-esteem and imply an identity change from stable citizen to a more negative characterization.5 Additionally, physician bias may impact on how they provide care. Finally, an understanding that these patients come from different SES and with lower educational backgrounds is critical when providing proper treatment. Keeping these concepts in mind, implementation of SBI in primary care helps to decrease self-reported alcohol use among adults identified by screening.5
The 15-Method. The 15-Method provides structure for treatment of alcohol use disorders in the primary care setting, with evidence supporting its effectiveness.5,10 It involves 2 primary aspects: the length of the sessions is 15 minutes, and the patients score above 15 on the AUDIT. The model consists of 3 steps as follows. First, patients are screened, and a brief intervention occurs for those who score positive. Second, an assessment focusing on consequences of alcohol use is provided. Finally, there are 4 subsequent sessions focusing on cognitive-behavioral therapy and motivational interviewing.5
We feel that DPMs can consider performing this in the office setting via their medical assistants while patients are waiting in the waiting room/or waiting to see their doctor. Essentially, this will help start the process so when these patients are referred, initial screening is completed.
Making a Referral to Treatment
It is critical for the provider to know when a patient should be referred to a specialist. This should occur if there is confidence that the patient already has an AUD (and not just drinking at risky levels) or when the above interventions have been implemented with no improvement. Providers should discuss specialty care with the patient and answer questions prior to the referral. This may include a discussion about potential pharmacotherapy and psychosocial interventions. This will decrease the mystery and stigma associated with treatment for AUD. DPMs should also collaborate with the patient’s primary care physician or provide screening results if concerns arise.
In Conclusion
Podiatrists have an opportunity to intervene early and possibly make a huge difference in the trajectory of alcohol use disorder. Early intervention may prevent problematic drinking from turning into an AUD. Additionally, it may prevent the progression of an already established AUD and decrease/improve medical conditions associated with alcohol use. Connecting with patients in this way serves to open conversations, normalize the condition, decrease stigma, and has many other benefits. By incorporating the aforementioned screening, intervention and referral protocol in podiatric practice, patients with alcohol usage disorder may benefit tremendously.
Dr. Rashid practices in the Department of Podiatric Medicine and Surgery at Yale New Haven Health in New Haven, CT.
Dr. Cheung practices in the Department of Podiatric Medicine and Surgery at Yale New Haven Health in New Haven, CT.
Dr. Aleem practices in the Department of Podiatric Medicine and Surgery at Beth Israel Deaconess Medical Center in Boston.
Dr. Paracha practices in the Department of Internal Medicine at Yale New Haven Health in New Haven, CT.
Dr. Vyce is the Chair of the Department of Podiatric Surgery and Residency Director at Yale New Haven Health in New Haven, CT.
Dr. Fuehrlein practices in the Department of Psychiatry of Yale University in New Haven, CT.
References
- Babor TF, Ritson EB, Hodgson RJ. Alcohol-related problems in the primary health care setting: a review of early intervention strategies. Br J Addict. 1986 Feb;81(1):23-46. doi: 10.1111/j.1360-0443.1986.tb00291.x. PMID: 3457598.
- Kranzler HR, Soyka M. Diagnosis and pharmacotherapy of alcohol use disorder: a review. JAMA. 2018;320(8):815–824. doi:10.1001/jama.2018.11406
- American Psychiatric Association. (2013). Diagnostic and Statistical Manual of Mental Disorders (5th ed.). https://doi-org.ezproxy.frederick.edu/10.1176/appi.books.9780890425596
- McCambridge J, Saitz R. Rethinking brief interventions for alcohol in general practice. BMJ. 2017; 356 :j116 doi:10.1136/bmj.j116
- Glass JE, Andréasson S, Bradley KA, et al. Rethinking alcohol interventions in health care: a thematic meeting of the International Network on Brief Interventions for Alcohol & Other Drugs (INEBRIA). Addict Sci Clin Pract. 2017 May 10;12(1):14. doi: 10.1186/s13722-017-0079-8. PMID: 28490342; PMCID: PMC5425968.
- Maiya RP, Messing RO. Peripheral systems: neuropathy. Handb Clin Neurol. 2014;125:513-25. doi: 10.1016/B978-0-444-62619-6.00029-X. PMID: 25307593.
- Meca A, Tubman JG, Regan T, et al. Preliminary evaluation of the NIAAA/AAP Brief Alcohol Use Screener. Alcohol Alcohol. 2017 May 1;52(3):328-334. doi: 10.1093/alcalc/agx009. Erratum in: Alcohol Alcohol. 2017 May 1;52(3):334. PMID: 28430936; PMCID: PMC6213085.
- Do Amaral RA, Malbergier A. Effectiveness of the CAGE questionnaire, gamma-glutamyltransferase and mean corpuscular volume of red blood cells as markers for alcohol-related problems in the workplace. Addict Behav. 2008 Jun;33(6):772-81. doi: 10.1016/j.addbeh.2007.12.006. Epub 2007 Dec 27. PMID: 18337017.
- Bradley KA, Williams EC, Achtmeyer CE, Volpp B, Collins BJ, Kivlahan DR. Implementation of evidence-based alcohol screening in the Veterans Health Administration. Am J Manag Care. 2006 Oct;12(10):597-606. PMID: 17026414.
- Wallhed Finn S, Hammarberg A, Andreasson S, Jirwe M. Treating alcohol use disorders in primary care - a qualitative evaluation of a new innovation: the 15-method. Scand J Prim Health Care. 2021 Mar;39(1):51-59. doi: 10.1080/02813432.2021.1882079. Epub 2021 Feb 15. PMID: 33586596; PMCID: PMC7971313.
- Julian T, Glascow N, Syeed R, Zis P. Alcohol-related peripheral neuropathy: a systematic review and meta-analysis. J Neurol. 2019 Dec;266(12):2907-2919. doi: 10.1007/s00415-018-9123-1. Epub 2018 Nov 22. PMID: 30467601; PMCID: PMC6851213.
- Shibuya N, La Fontaine J, Frania SJ. Alcohol-induced neuroarthropathy in the foot: a case series and review of literature. J Foot Ankle Surg. 2008 Mar-Apr;47(2):118-24. doi: 10.1053/j.jfas.2007.12.009. PMID: 18312919.