


Spontaneous Bilateral Achilles Tendon Ruptures After Fluoroquinolone Use
This article was created in partnership with the American Society of Podiatric Surgeons.
![]()
Tendinopathies and tendon ruptures are known side effects of fluoroquinolone use reported throughout the literature, beginning in the 1980s.1-3 Less than 1 percent of all Achilles tendon ruptures are bilateral,4 and the risk factors for such ruptures include fluoroquinolone or corticosteroid use, renal impairment, and diabetes mellitus.5,6 In this article, we report a case of this unusual occurrence that highlights the potential impact of these medications for patients.

When a Patient Presents With Bilateral Lower Leg Pain
A 71-year-old male presented to our urgent care center due to pain in the bilateral lower legs in the area of the Achilles tendons. He stated that 9 days prior, while walking in his room, he heard an audible “pop” before experiencing sudden pain in the left lower extremity. He limped around on the injury for another 6 days until he sought care at an outside emergency room. They diagnosed him with an Achilles tendon rupture and placed him in a posterior splint. He reported hearing another audible pop after getting out of bed two days later, with pain in his right Achilles. This led him to present to our facility one day later, concerned about issues with muscle strength and ambulating bilaterally.
The patient’s medical history was significant for chronic obstructive pulmonary disease (COPD), rheumatoid arthritis (RA), hypertension (HTN), and hyperlipidemia. He took 5 mg of prednisone daily chronically at baseline. Two days before the first injury, an outside emergency room gave him levofloxacin for COPD exacerbation and a methylprednisolone dose pack. He discontinued both the steroid and the levofloxacin once seen for the first Achilles tendon rupture. His social history included him living alone with no local support system.
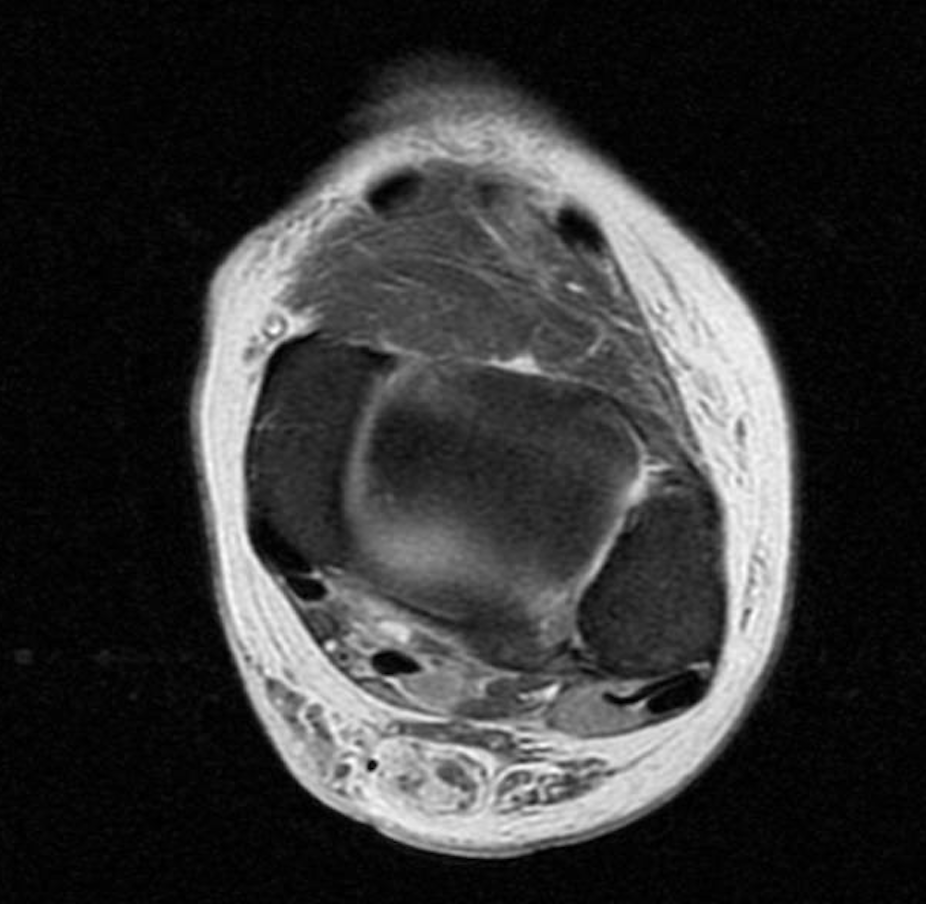
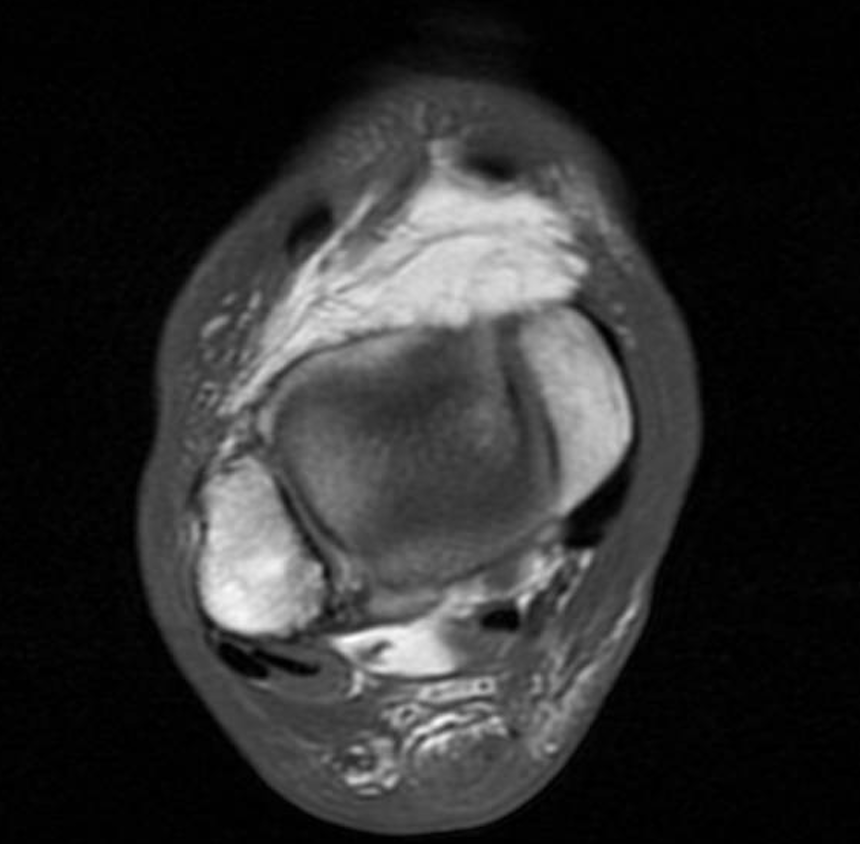
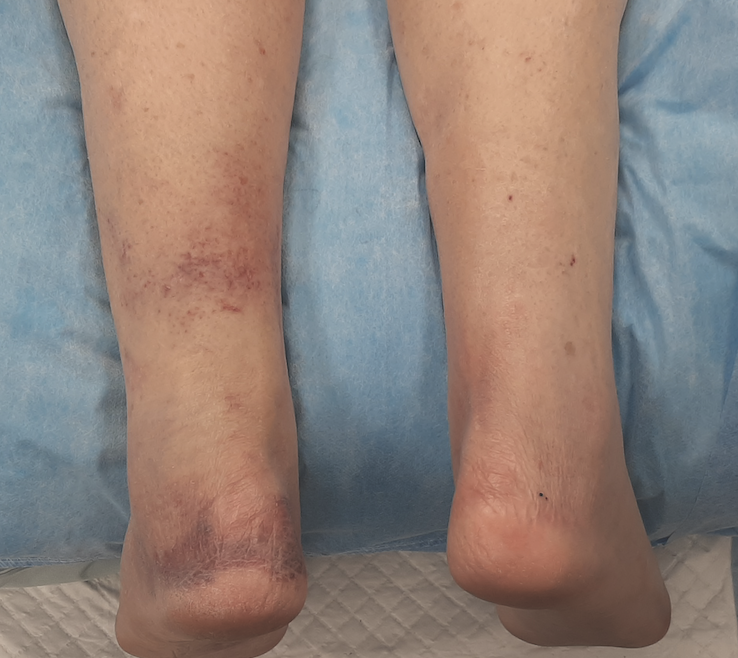
A physical exam revealed edema bilateral to the lower extremities with ecchymosis on the left side but not on the right lower extremity. The patient was neurovascularly intact, and the exam revealed a positive Thompson test on the bilateral lower extremities with no active ankle plantarflexion on the left and right sides. There was a palpable delve in the Achilles on both sides. An MRI that day on both lower legs revealed bilateral Achilles tendon ruptures with a left gap of 3.5cm and a right gap of 2.5 cm.
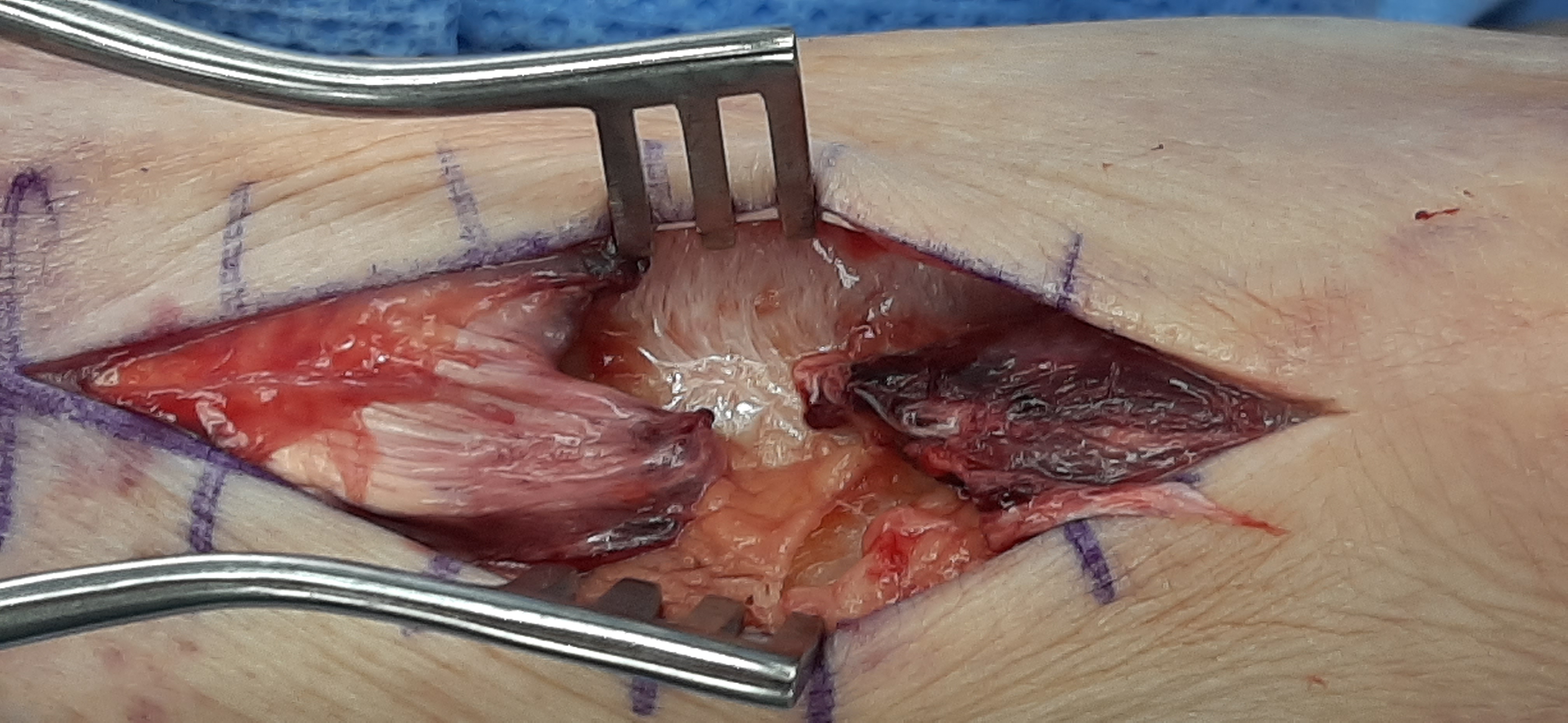
The next day, we took the patient to the OR for bilateral Achilles tendon repair.
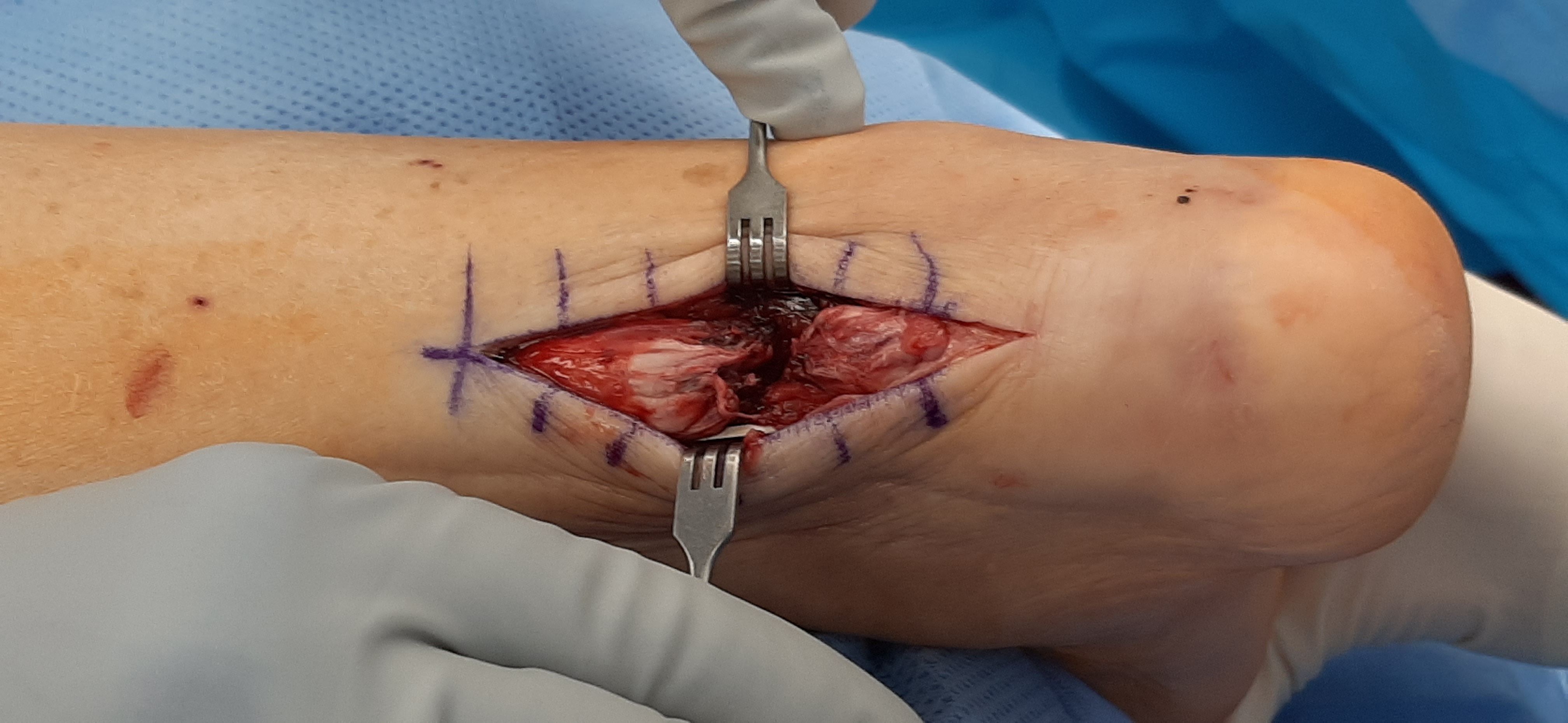
Anesthesia performed bilateral popliteal blocks. We made a typical linear mid-Achilles incision on both sides and performed an end-to-end repair with 2 Orthocord (DePuy-Synthes) in a Krakow fashion. The plantaris was still intact on both sides. After placing the patient in bilateral “L” and “U” splints and admitting him overnight, we transferred him to a skilled nursing facility for recovery and care. We made this decision because he lived alone and would be unable to bear weight bilaterally. At 3 weeks postop, we removed his sutures, and at 4 weeks, he transitioned to weight-bearing as tolerated in controlled ankle motion (CAM) boots with 9mm heel lifts. He began physical therapy, and at 6 weeks postop, he returned home, where he continued to receive in-home physical therapy. By 9 weeks, he was back in regular shoes, and by 14 weeks, he completed physical therapy, back to all regular activities with no deficits. One year after the surgery, he had no further complications and continued all baseline activities.

Understanding the Risks of Fluoroquinolone Use
Fluoroquinolone use has a significant risk of tendon rupture. In 2008, the United States added a black box warning regarding this risk to product labels of all fluoroquinolone antibiotics. Drug-induced tendinopathy is a known class side effect of fluoroquinolones, with rates of tendinopathy at 3.21000 in all patients and 6.21000 in patients over 60.7 Kahen and colleagues reported a tendon rupture rate of 4 per 1,000,000 in patients taking fluoroquinolones.8 Ninety-five percent of tendinopathies and ruptures secondary to fluoroquinolone use involve the Achilles tendon.9 Multiple risk factors increase the risk of tendon rupture in patients given fluoroquinolones; these include age greater than 60, renal disease, diabetes, hyperparathyroidism, rheumatic disease, trauma, male sex, and corticosteroid use. Obesity is protective to some degree.10 Our patient had most of these risk factors. He did not have renal disease or hyperparathyroidism.
Incidences of tendinopathies and ruptures occur anywhere from 2 days to 90 days after the administration of the fluoroquinolones, averaging 13 days.9,11 Our patient had his first Achilles tendon rupture two days after starting the fluoroquinolone, and his second rupture 10 days after starting and two days after discontinuing the levofloxacin. Although all fluoroquinolones have implications for tendon issues, the most commonly associated in descending order are pefloxacin, ofloxacin, norfloxacin, and ciprofloxacin.12 Levofloxacin is an enantiomer of ofloxacin. More recent literature shows that ciprofloxacin has the highest rate of tendon injury of any of the fluoroquinolones.13
What Does the Literature Reveal About Tendon Ruptures?
Bilateral Achilles tendon ruptures, such as those presented in our patient, are extremely rare. In 2012 Ellanti and colleagues presented 30 cases reported in the English language of bilateral Achilles tendon ruptures either with or without fluoroquinolone use.14 Fewer than 20 cases in the literature have a connection to fluoroquinolones.15 Many of these case studies did not mention if the ruptures occurred simultaneously or on different days, as was with our patient. Nearly all of the cases caused by fluoroquinolone use underwent surgical treatment.4,6,14-22
Parmar, Kawtharani, Gottschalk, and their respective teams reported cases treated conservatively, with Gottsckalk’s patient dying 11 weeks after injury due to myocardial infarction, sepsis, and kidney failure.5, 22-23 We decided to treat our patient surgically to
reduce the rate of rerupture. Conservative treatment, including aggressive outpatient physical therapy, would have been very challenging for him as he lived alone and did not have support to drive him to appointments. After surgery, being admitted to a skilled nursing facility made his recovery possible and successful. Surgically treating Achilles tendon ruptures is superior to conservative treatment in several sources, 24-27 although new literature is starting to call this assumption into question for centers with early range of motion protocols.28-30
The literature notes that even with the number of cases reported, the
pathophysiology of fluoroquinolone inducing tendon rupture is not clear. The proposed theory is that quinolones cause inhibition of phosphorylation of focal adhesion kinase. Once this occurs, there is an inhibition of tenocyte migration necessary for tendon repair and response to injury.31,32
Concluding Thoughts
Although tendinopathy and tendon ruptures, especially Achilles tendon ruptures, are known side effects of fluoroquinolone use, a bilateral Achilles tendon rupture is a rare condition. Our patient had multiple risk factors, including age greater than 60, male sex, chronic steroid use, rheumatoid arthritis, and low BMI which made him particularly vulnerable to adverse effects of fluoroquinolones and tendon ruptures. He ultimately had a good outcome after surgical repair, but avoidance of levofloxacin in patients of his risk level is a wise choice to avoid the need for surgery and the natural sequelae of such ruptures.
Dr. Jones is the Chairman and a Fellow of the American Society of Podiatric Surgeons, as well as a Fellow of the American College of Podiatric Medicine. He practices in Spokane, WA.
Sue Y. Cole, PA-C is the President and a Fellow of the Washington Academy of Physician Assistants as well as a Fellow of the American Academy of Physician Assistants. She practices in orthopedics in Spokane, WA.
References
1. Bailey RR, Kirk JA, Peddie BA. Norfloxacin-induced rheumatic disease. NZ Med J. 1983;96:590.
2. McEwan SR. Davey PG. Ciprofloxacin and tenosynovitis. Lancet. 1988;2:900.
3. Hutson KA. Achilles tendinitis and tendon rupture due to fluroquinoloneantibiotics. N Engl J Med. 1994;331:748.
4. Habusta SF. Bilateral simultaneous rupture of the Achilles tendon: a rare traumatic injury. Clin Orthop Relat Res. 1995;320:231-234
5. Gottschalk A, Bachman J. Death following bilateral complete Achilles tendon rupture in a patient on fluoroquinolone therapy: a case report. J Med Case Rep. 2009;3:1.
6. Ureten K, Ozturk MA, Ozbek M, Unverdi S. Spontaneous and simultaneous rupture of both Achilles tendons and pathological fracture of the femur neck in a patient receiving long-term hemodialysis. Int Urol Nephrol. 2008;40(4):1103-1106.
7. van der Linden PD, Sturkenboom MCJM, Herings RMC, Leufkens HGM, Stricker BHCh. Fluroquinolones and risk of achilles tendon disorders: case control study. BMJ. 2002;324(7349):1306-1307.
8. Kahn JB. Latest industry information on the safety profile of levofloxacin in the US. Chemotherapy. 2001;47(suppl 3):32-37.
9. Casparian JM, Luchi M, Moffat R, Hinthorn D. Quinolones and tendon ruptures. South Med J. 2000;93(5):488-491.
10. Wise BL, Peloquin C, Choi H, Lane NE, Zhang Y. Impact of age, sex, obesity and steroid use on quinolone-associated tendon disorders. Am J Med. 2012;125(12):1128.
11. Vander Linden PD, van Puijenbroek EP, Feenstra J, et al. Tendon disorders attributed to fluoroquinolones: a study on 42 spontaneous report in the period 1988-1998. Arthritis Rheu. 2001;45:235-239.
12. Mathis AS, Chan V, Gryszkiewicz M, Adamson RT, Friedman GS. Levofloxacin-associated Achilles tendon rupture. Ann Pharmacother. 2003;37(7-8):1014-1017.
13. Nyyssonen T, Lantto I, Luthje P, Selander T, Kroger H. Drug treatments associated with achilles tendon rupture. A case-control study involving 1118 Achilles tendon ruptures. Scand J Med Sci Sports. 2018;28(12):2625-2629.
14. Ellanti P, Davarinos N, Burke TE, D’Souza LG. Long-term functional outcome of bilateral spontaneous and simultaneous Achilles tendon ruptures. Foot Ankle Spec. 2012;5(5):318-320.
15. Khanzada Z, Rethnam U, Widdowson D, Mirza A. Bilateral spontaneous non-traumatic rupture of the Achilles tendon: a case report. J Med Case Rep. 2011;5:263
16. Kowatari K, Nakashima K, Ono A, Yoshiahra M, Amano M, Toh S. Levofloxacin induced bilateral Achilles tendon rupture: a case report and review of the literature. J Orthop Sci. 2004;9(2):186-190.
17. Akali AU, Niranjan NS. Management of bilateral Achilles tendon rupture associated with ciprofloxacin: a review and case presentation. J Plast Reconstr Aesthet Surg. 2008;61(7):830-834.
18. Lewis T. A rare care of ciprofloxacin-induced bilateral rupture of the Achilles tendon. BJM Case Rep. 2009. Doi: 10.1136bcr.08.3008.0697.
19. Filippucci E, Farina A, Bartolucci F, Spallacci C, Busilacchi P, Grassi W. Levofloxacin-induced bilateral rupture of the Achilles tendon: clinic and sonographic findings. Reumatismo. 2003;55(4):267-269.
20. Panigrahi R, Longcroft-Wheaton G, Laji K. Bilateral ankle pain and quinolone use: a case of tendon rupture secondary to quinolone use. Br J Hosp Med (Lond). 2008;69(3):168-169.
21. Pantalone A, Abate M, D’Ovidio C, Carnevale A, Salini V. Diagnostic failure of ciprofloxacin-induced spontaneous bilateral achilles tendon rupture: case-report and medical-legal considerations. Int J Imm Pharm. 2011;24(2):519-522.
22. Parmar C, Meda KP, Hennessy M. Achilles tendon rupture associated with combination therapy of levofloxacin and steroid in four patients and a review of the literature. Foot Ankle Int. 2007;28(12):1287-1289.
23. Kawtharani F, Masrouha KZ, Afeiche N. Bilateral Achilles tendon ruptures associated with ciprofloxacin use in the setting of minimal change disease: Case report and review of the literature. J Foot Ankle Surg. 2016;55:276-278.
24. Deng S, Sun Z, Zhang C, Chen G, Li J. Surgical treatment versus conservative management for acute Achilles tendon rupture: a systematic review and meta-analysis of randomized controlled trials. J Foot Ankle Surg. 2017;56(6):1236-1243.
25. Reda Y, Farouk, A, Abdelmonem I, Shazly OAE. Surgical versus non-surgical treatment for acute Achilles’ tendon rupture. A systematic review of literature and meta-analysis. Foot Ankle Surg. 2020;26(3):280-288.
26. Khan RJ, Fick D, Keogh A, Crawford J, Brammer T, Parker M. treatment of acute achilles tendon ruptures. A metaanalysis of randomized, controlled trials. J Bone Joint Surg Am. 2005;87:2202-2210.
27. Bhandari M, Guyatt GH, Siddiqui F, et al. Treatment of cute achilles tendon ruptures; a systematic overview and meta-analysis. Clin Orthop Relat Res.2002;400:190-200.
28. Soroceanu A, Sedhwa F, Aarabi S, Kaufman A, Glazebrook M. Surgical versus nonsurgical treatment of acute Achilles tendon rupture: a meta-analysis of randomized trials. J Bone Joint Surg Am. 2012;94(23):2136-2143.
29. van der Eng DM , Schepers T, Goslings JC, Schep NWL. Rerupture rate after early weightbearing in operative versus conservative treatment of Achilles tendon ruptures: a meta-analysis. J Foot Ankle Surg. 2013;52(5):622-628.
30. Zhang H, Tang H, He Q, et al. Surgical versus conservative intervention for acute Achilles tendon rupture: a prisma-compliant systematic review of overlapping meta-analyses. Medicine. 2015;94(45):e1951.
31. Shakibaei M, Staklmann R. Ultrasound of Achilles tendon from rats after treatment with fleroxacin. Arch Toxicol. 2001;75(2):97-102.
32. Tsai WC, Hsu CC, Chen HC, et al. Ciprofloxacin-mediated inhibition of tenocyte migration and down regulation of focal adhesion kinase phosphorylation. Eur J Pharmacol. 2009;607:23-26.






