Atypical Desmoplastic Melanoma in an African American Man
Desmoplastic melanoma is a rare subtype of malignant melanoma, characterized histologically by the presence of spindled melanocytes and prominent stromal fibrosis.1 Typically, desmoplastic melanoma presents as an amelanotic plaque or nodule on sun-exposed areas of the skin. Due to its subtle presentation, lacking typical features of melanoma, diagnosis is often delayed. Desmoplastic melanomas may develop de novo, in conjunction with other forms of melanoma, such as lentigo maligna or acral lentiginous melanoma, or, in rare cases, in mucosal sites.1 Here, we present a case of desmoplastic melanoma at an atypical site in an African American man.

Case Presentation
A 90-year-old African American man with dementia and no personal or family history of skin cancer presented with a 2-year history of a left lower abdominal lesion following a left hip ablation in 2021. According to the patient’s daughter, the lesion had grown from the size of a quarter to over 3 cm and had become firmer. On initial examination, a firm, indurated, smooth, 5-cm, violaceous nodule was noted on the left lower abdomen (Figure 1). The area was non-fluctuant, lacked warmth or surrounding erythema, and showed no signs of drainage, bleeding, or significant tenderness. An ultrasound was ordered to assess the growth, and the patient was prescribed 100 mg of doxycycline twice daily, with plans for a follow-up biopsy in 3 weeks. However, due to subsequent hospital admissions and rehabilitation after a fall, the patient did not return for the biopsy until several months later.
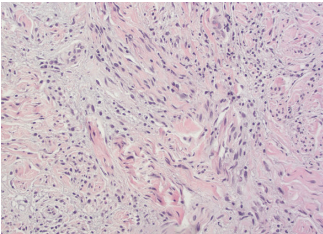
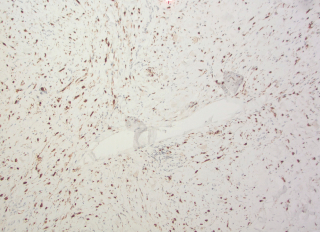
A punch biopsy revealed pleomorphic spindle cells infiltrating the deep dermis, positive for S100, vimentin, and SOX10, and negative for epithelial markers and other controls (Figure 2 and Figure 3). A second biopsy was S100 and SOX10 positive and Melanin-A and HMB45 negative (Figure 3). The case was subsequently sent to the Joint Pathology Center, which confirmed spindle cell proliferation and suspicion for desmoplastic melanoma. An 18F-FDG positron emission tomography-computed tomography scan showed a subcutaneous mass (6.7 x 2.5 cm) in the left mid-abdominal wall. The case was discussed at the Melanoma/Skin Cancer Tumor Board Conference, and the family opted for palliation, agreeing to a wide local excision with possible skin graft but declining sentinel lymph node dissection.
Discussion
Desmoplastic melanoma comprises 1% to 4% of primary cutaneous melanomas.2,3 It has 2 subtypes: the pure form, with greater than 90% desmoplasia, and the mixed form, with less than 90% desmoplasia.1-4 Recent studies suggest better prognosis for desmoplastic melanoma compared to non-desmoplastic melanoma, with pure desmoplastic melanoma showing the best survival rates.2,4 However, desmoplastic melanoma is associated with a higher rate of local recurrence.2 Desmoplastic melanoma is highly mutated, with common mutations linked to ultraviolet light exposure, including NF1, ERBB2, MAP2K1, MAP3K1, EGFR, MET, TERT, NFKBIE, PIK3CA, and PTPN11.2,4
Desmoplastic melanoma typically presents as a firm, skincolored nodule, papule, or plaque on chronically sun-damaged skin, particularly in older individuals. It can occasionally overlap with lentigo maligna.1-3 The majority of desmoplastic melanoma cases are found on the head and neck (50%), with 25% on the trunk and 25% on the extremities.2,3 Early clinical and histologic presentations may lack atypical features, leading to diagnostic delays.1,2
Excisional biopsy is crucial for diagnosis. Differential diagnoses include cutaneous metastasis, abscess, soft tissue tumors, and sarcoma. As such, biopsy becomes critical for establishing a definitive diagnosis and is considered the mainstay of care when desmoplastic melanoma is among the differential.3
Treatment usually involves wide local excision of the lesion, with consideration for sentinel lymph node biopsy based on the lesion’s thickness.1-3 Other treatment options include immunotherapy and radiation therapy.1-3
Conclusion
This atypical presentation of desmoplastic melanoma on the lower abdomen is one of the few documented cases in a patient of African descent.5 A report on 3 African American patients with desmoplastic melanoma noted the absence of an intraepidermal melanoma component (in situ) and solar elastosis, leading the authors to suggest a cause not linked to chronic sun exposure.5 Patients with desmoplastic melanoma are usually fair-skinned individuals with chronic sun exposure.1-5 This case emphasizes the importance of obtaining a biopsy, particularly when the diagnosis is uncertain.
Juliana O’Reilly is a fourth-year medical student in the Felix Edward Hébert School of Medicine at Uniformed Services University of the Health Sciences in Bethesda, MD. Dr Khanna is a resident doctor in the department of dermatology at Howard University College of Medicine in Washington, DC. Dr Maiberger and Dr Aziz are dermatologists and Dr Chen is a pathologist at the Washington DC Veterans Affairs Medical Center in Washington, DC.
Disclosure: The authors report no relevant financial relationships.
Disclaimer: The views expressed in this article are those of the authors and do not reflect the official policy of the Uniformed Services University of the Health Sciences, Department of Army/Navy/Air Force, Department of Defense, or US Government.
References
1. Zaba LC, Wang JY, Swetter SM. Melanoma. In: Bolognia JL, Schaffer JV, Cerroni L, eds. Dermatology. 5th ed. Elsevier; 2024:2009-2044.
2. Hughes TM, Williams GJ, Gyorki DE, et al. Desmoplastic melanoma: a review of its pathology and clinical behaviour, and of management recommendations in published guidelines. J Eur Acad Dermatol Venereol. 2021;35(6):1290-1298. doi:10.1111/jdv.17154
3. Nicolson NG, Han D. Desmoplastic melanoma. J Surg Oncol. 2019;119(2): 208-215. doi:10.1002/jso.25317
4. Shain AH, Garrido M, Botton T, et al. Exome sequencing of desmoplastic melanoma identifies recurrent NFKBIE promoter mutations and diverse activating mutations in the MAPK pathway. Nat Genet. 2015;47(10):1194-1199. doi:10.1038/ng.3382
5. Busam KJ, Ariyan C, Coit DC. Desmoplastic melanoma in African American patients. Arch Dermatol. 2010;146(7):796-797. doi:10.1001/archdermatol.2010.149