Milia en Pickle: A Case of Pickleball-Induced Milia en Plaque
© 2025 HMP Global. All Rights Reserved.
Any views and opinions expressed are those of the author(s) and/or participants and do not necessarily reflect the views, policy, or position of the Dermatology Learning Network or HMP Global, their employees, and affiliates.
Milia en plaque (MEP) is an uncommon dermatologic condition characterized by a localized erythematous plaque with embedded milia. While the etiology of MEP is generally idiopathic, trauma to the skin has been identified as a contributing factor in some instances. Trauma-induced MEP has been previously linked to injuries including, but not limited to, burns, cosmetic procedures, and physical trauma; the lesion typically appears weeks to months after the inciting trauma.1-3 In these cases, trauma disrupts the skin’s pilosebaceous unit, leading to the entrapment of keratin and subsequent cyst formation. Herein, we present a case of MEP following sports trauma.

Case Presentation
A 57-year-old woman presented to dermatology for a lesion on the right cheek that developed after being hit with a pickleball while playing the sport (Figure 1). She had not previously had any lesions at this location. The injury initially appeared like a blister with minimal bleeding on the edge. She applied a topical combination antibiotic containing neomycin, polymyxin B, and bacitracin to the wound. Besides the initial impact, the lesion was not painful or pruritic. However, it did not resolve with time and 3 to 4 weeks later, she presented with a thickened spot on her cheek. She had no history of prior injuries healing in this way. On exam, a well-defined, tan 2-cm x 1.5-cm plaque with white-cystic structures was seen at the site of injury on the right zygomatic cheek. Given diagnostic uncertainty, a punch biopsy was performed.
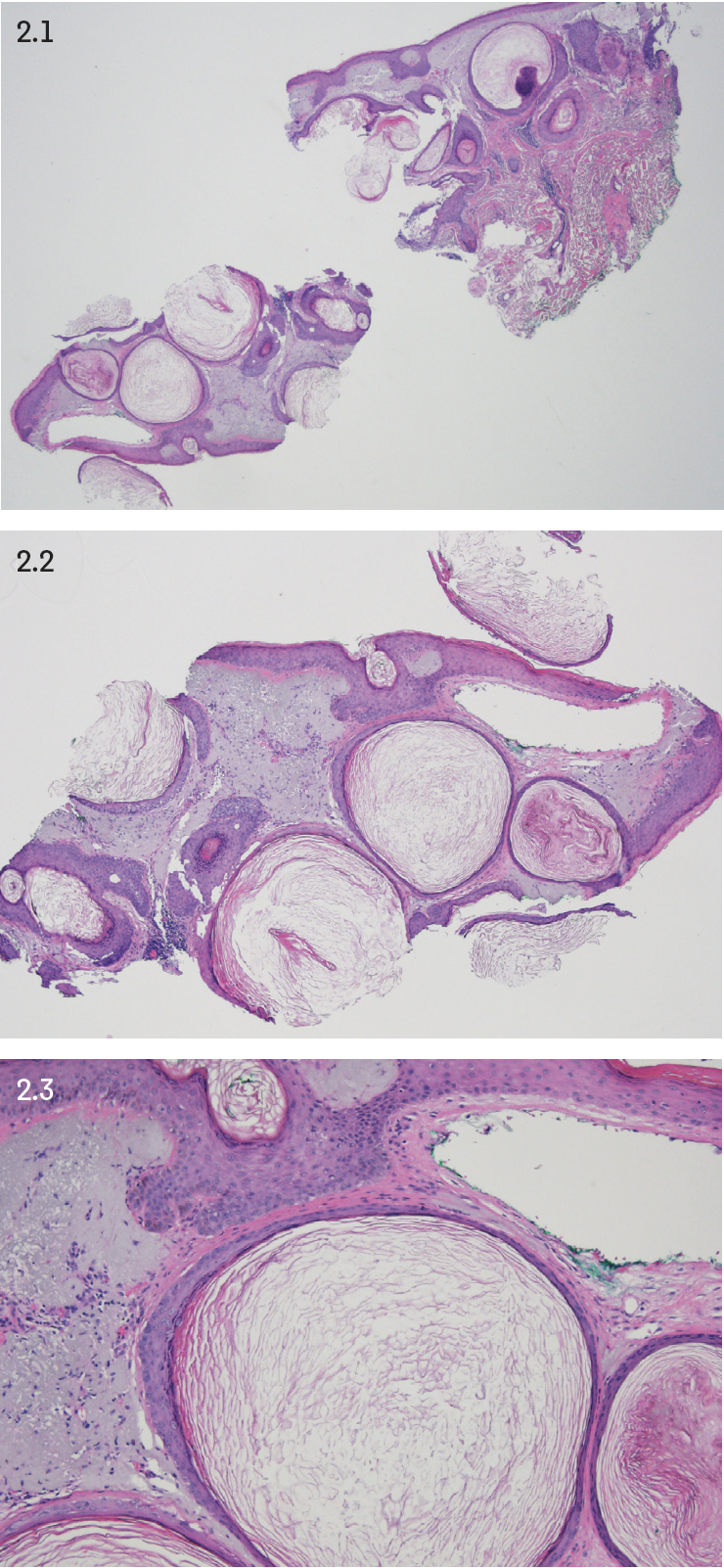
On histopathologic exam, portions of dermal cystic squamous epithelium with intact granular layer were seen, with at least one containing a hair shaft (Figure 2). With clinicopathologic correlation and photo review, a diagnosis of MEP was determined.
Discussion
Pickleball, the most rapidly growing sport in the United States, continues to gain popularity due to its low-impact nature and accessibility.4,5 With its recent gain in popularity, injuries relating to the sport are also on the rise.6,7 Recent studies report sprains/ strains, fractures, Achilles tendon injuries, and low back pain as the most common injuries in pickleball athletes, but do not specifically mention cutaneous injuries.8,9 However, not all injuries are orthopedic, as demonstrated in this case. Generally, dermatologic conditions associated with sports, particularly paddle or racket ball sports, result from high-velocity impacts from equipment (balls, paddles, rackets) or impact from the court surface, leading to abrasions, contusions, and occasionally lacerations.10-13
Given the numerous coalescent lesions and highly visible location, our patient was presented at department-wide grand rounds for input on treatment. Typical treatment of MEP is monitoring vs extraction. However, the extraction of multiple adjacent lesions would be uncomfortable, technically difficult, and carry an elevated risk of scarring. Staged extraction was suggested as a potential procedural treatment, with 3 to 4 preceding months of topical tretinoin 0.1%. Other treatment options offered to the patient were topical tretinoin 0.1% alone, laser, or no treatment. At this point, the patient is applying topical tretinoin and will follow up in a few months to determine further management.
Conclusion
To date, there have not been any reports of MEP resulting from pickleball or other sports. This case highlights the potential for MEP to develop as a delayed consequence of sports-related skin trauma. Furthermore, it emphasizes the need for a better understanding of potential injuries related to the popular, growing sport of pickleball and awareness of dermatologic manifestations of sports-related injuries.
References
1. Beutler BD, Cohen PR. Cryotherapy-induced milia en plaque: case report and literature review. Dermatol Online J. 2014;21(2):13030/qt4dw7k4nk
2. Lee WS, Kim SJ, Ahn SK, Lee SH. Milia arising in herpes zoster scars. J Dermatol. 1996;23(8):556-558. doi:10.1111/j.1346-8138.1996.tb02651.x
3. Losada-Campa A, De La Torre-Fraga C, Cruces-Prado M. Milia en plaque. Br J Dermatol. 1996;134(5):970-972.
4. SFIA’s topline participation report shows strong positive trends across multiple sports and fitness categories. Sports & Fitness Industry Association. February 27, 2024. Accessed March 26, 2025. https://sfia.org/resources/sfias-topline-participation-report-shows-strong-positive-trends-across-multiple-sports-and-fitness-categories-2
5. 2024 USA Pickleball annual facts & highlights. USA Pickleball. January 14, 2025. Accessed March 26, 2025. https://usapickleball.org/about-us/organizational-docs/pickleball-annual-growth-repor
6. Azar, FM. Lamplot JD, Bernholt DL, Spence DD. Pickleball: a standard review of injury prevalence and prevention in a rapidly growing sport. J Am Acad Orthop Surg. 2024;32(22):e1130-e1141. doi:10.5435/JAAOS-D-24-00151
7. Stroesser K, Mulcaster A, Andrews DM. Pickleball participation and the health and well-being of adults—a scoping review. J Phys Act Health. 2024;21(9):847- 860. doi:10.1123/jpah.2024-0092
8. Olsen AA, Li A, Johnson DD, Manson HC. Pickleball primer: an overview of common injuries, treatment, and optimization strategies in pickleball athlete. J Am Acad Orthop Surg. 2024;32(17):763-770. doi:10.5435/JAAOS-D-23-00705
9. Opara OA, Brush PL, Pohl N, et al. Pickleball- and paddleball-related injuries in the lower extremity: description, treatment options, and return to play. Cureus. 2024;16(2):e53954. doi:10.7759/cureus.53954
10. Cohen PR. The ball SITE sign: ball sports-induced targetoid erythema in a racquetball player. Dermatol Pract Concept. 2015;5(3):47-52. doi:10.5826/dpc.0503a11
11. Steele, RB, Taylor, JS, Aneja, S. Skin disorders in athletes: professional and recreational sports. In: John S, Johansen J, Rustemeyer T, Elsner P, Maibach H, eds. Kanerva’s Occupational Dermatology. Springer; 2018.
12. Forrester MB. Pickleball-related injuries treated in emergency departments. J Emerg Med. 2020;58(2):275-279. doi:10.1016/j.jemermed.2019.09.016
13. Nhan DT, Klyce W, Lee RJ. Epidemiological patterns of alternative racquet-sport injuries in the United States, 1997–2016. Orthop J Sports Med. 2018;6(7):2325967118786237. doi:10.1177/2325967118786237