


Advancing Itch Management With Emerging Therapies and Neuromodulation
© 2025 HMP Global. All Rights Reserved.
Any views and opinions expressed are those of the author(s) and/or participants and do not necessarily reflect the views, policy, or position of The Dermatologist or HMP Global, their employees, and affiliates.

In this in-depth interview, Dr Brian S. Kim shares key clinical insights on the evolving neuroimmunology of itch and the growing role of targeted therapies, highlighting how agents, such as Janus kinase (JAK) inhibitors, dupilumab, and kappa opioid receptor agonists, are redefining treatment strategies for both inflammatory and neuropathic itch.
THE NEUROIMMUNOLOGY OF ITCH
The Dermatologist: How has our understanding of the neural pathways involved in itch evolved in recent years, and how does this knowledge impact clinical decision-making?
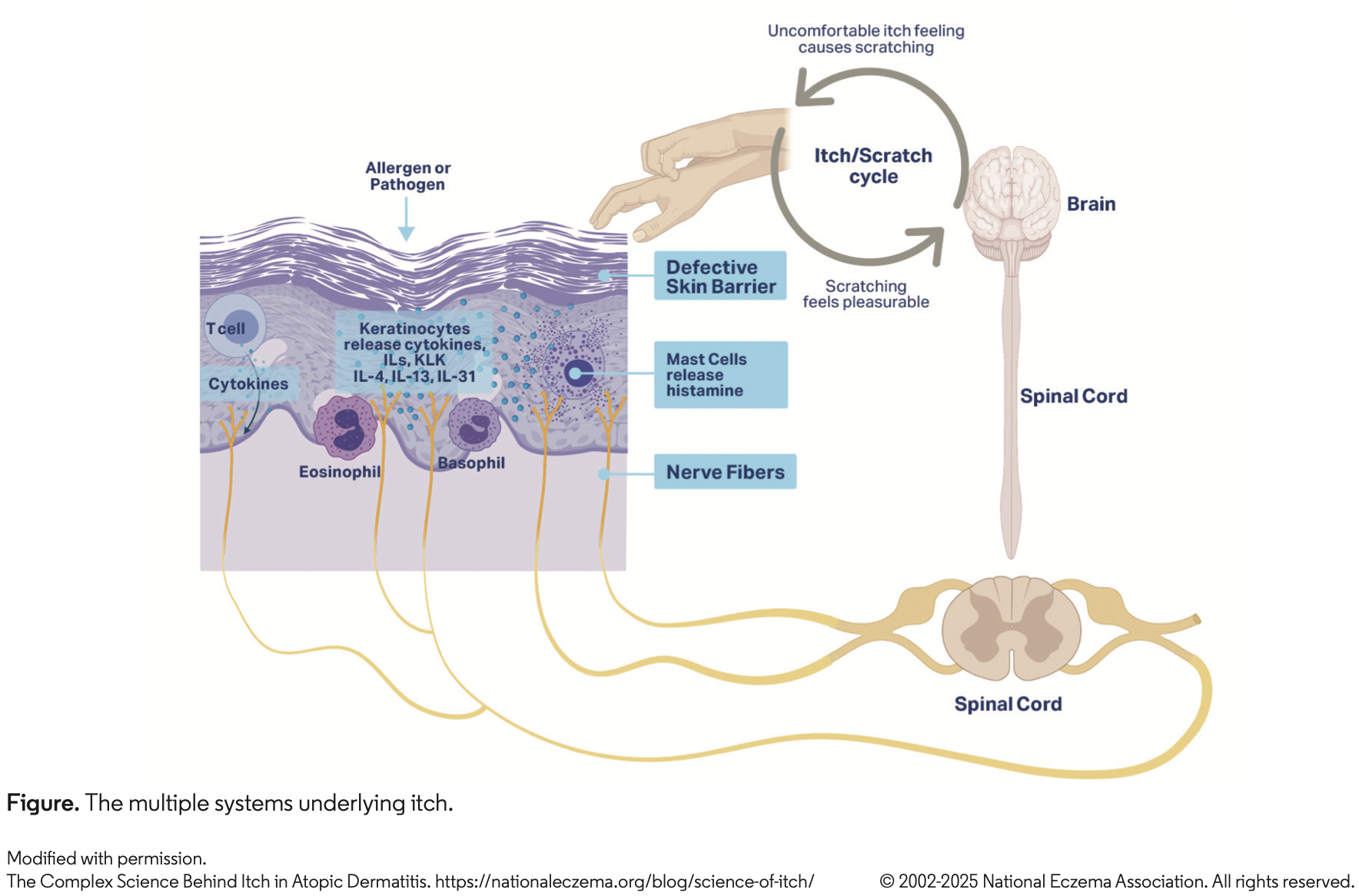
Dr Kim: In the last 10 years, we have come to clearly understand how inflammatory factors, called cytokines, can function to trigger itch by acting directly on the nerves (Figure). These include cytokines like IL-4, IL-13, and IL-31. Prior to this, all we could target was histamine, which does not cause the vast majority of itch in patients. We now have multiple drugs that target these pathways, including dupilumab, lebrikizumab, nemolizumab, and tralokinumab. In addition, we can block pathways that these cytokines bottleneck into such as JAK1 via drugs like abrocitinib, ruxolitinib, and upadacitinib. And many more are coming.
But now we are also starting to understand that itch itself may not just be a sensation but a prelude to inflammation, too, in the other direction. This is a big concept, so to be concrete I will give an example. We have a drug like dupilumab that is approved for prurigo nodularis (PN). The problem with PN is that it starts off with itch, which then leads to inflammation. It is not so much inflammation that leads to itch, rather it is itch that leads to inflammation, which is a little bit different than atopic dermatitis (AD). Based on a lot of the science, we believe that essentially what happens in PN is that the nerve is itchy, or “hot,” which can cause inflammation directly through the release of neuropeptides. We think that this is a new understanding of itch: It is not just a symptom, but in and of itself itch can be a potential driver of inflammation and disease.
The Dermatologist: Given the significant burden of chronic itch conditions, what are some key considerations dermatologists should keep in mind when selecting a treatment approach?
Dr Kim: You want to know what kind of itch the patient has. Do they have an inflammatory itch? If they do, you want an agent that has some anti-inflammatory property and maybe some additional anti-itch property. If it is more of a neuropathic itch, you really need an agent that is going to have a neuromodulatory property, whether it is something like gabapentin or butorphanol. Then there are conditions I view as a mix, where you have an element of neuropathy, but you also have an element of fibrotic inflammation that continues to propagate the itch. In this case, you want to treat the itch and the inflammation, and you also want to untie the knot of fibrosis to get rid of these hard nodules that are going to be hotspots for inflammation and persistent scratching. Every patient is going to come in with a slightly different kind of relative composition of inflammation and itch, and how these contribute to the condition. The other thing we now know is that the different agents are all going to impact inflammation and itch in slightly different ways, whether it is dupilumab, nemolizumab, the JAK inhibitors like topical ruxolitinib, lebrikizumab, or tralokinumab.
If you have an appreciation for these things, then you can tailor and personalize the treatment. For example, if a patient has tons of inflammation and lots of rash and itch, in my view, something like dupilumab might be more appropriate. If a patient with AD has not had a lot of rashes but has a ton of itch, nemolizumab might be more appropriate because it is much more of an itch-predominant drug. These are some of the ways in which you can tailor treatments because it is not going to be a one-size-fits-all approach.
THE CURRENT TREATMENT LANDSCAPE
The Dermatologist: The approval of targeted therapies for itch conditions represents a significant advancement in dermatology. What lessons have we learned from the development of dupilumab and JAK inhibitors that could inform future itch treatments?
Dr Kim: We have learned a lot. For instance, with the JAK inhibitors, and even early learnings from dupilumab, we know you can target itch very effectively. The JAK inhibitors taught us that we can target itch very rapidly. It used to take weeks before we could improve itch, and we now know improvement can happen within a matter of minutes to hours to a day. I am sure we are hearing that even with drugs like nemolizumab. Our fundamental clinical expectation and understanding of what we can do for our patients has shifted dramatically with these drugs. Now, the new standard for any drug coming out for a condition in which itch is a central symptom is going to be how quickly, potently, and effectively can you alleviate the itch?
The Dermatologist: How do emerging therapies targeting IL-31 compare to existing treatments in terms of efficacy and safety?
Dr Kim: There is no question that both of those pathways, whether it is dupilumab for IL-4 and IL-13 or nemolizumab for IL-31, can do things that traditional medicines just simply were not able to do. The added value of these kinds of agents derives from the fact that they clearly have anti-itch properties and probably anti-neuroinflammatory properties as well. This is different from just a traditional anti-inflammatory drug. Whether it is a topical or oral steroid, those do not get directly at neuroactive processes. They do not go after itch or neuroinflammation, they just go after inflammation. It might sound like semantics, but it is not. What we are understanding is that the breakthroughs in these therapies are greater efficacy, faster efficacy, and higher safety. This means there are real breakthroughs, with a new understanding of biology and new ways to harness that biology. I think we will be able to appreciate this more as newer agents arrive. For example, there are drugs coming in the near future that will combine these modalities.
The Dermatologist: How do kappa opioid receptor agonists like difelikefalin fit into the current treatment landscape, and what patient populations are most likely to benefit from them?
Dr Kim: We think that kappa opioid receptor agonism is a pathway for itch alleviation. These drugs have the capacity to suppress itch by stimulating very broad mechanisms. Namely, from our own studies, we have found they seem to be able to activate nerves in the skin that are probably the nerves which respond to scratching. They can mimic the feeling of scratching in an effective way to alleviate itch. But the nice thing about this is, not only could it potentially work in certain forms of inflammatory itch, but also neuropathic itch where it is not really an inflammatory stimulus causing the itch but just that the nerves are firing and too sensitive. In those situations, if you treat with anti-inflammatory agents, you are not going to be successful because the nerves themselves are particularly prone to just firing on their own.
FUTURE DEVELOPMENTS
The Dermatologist: Your presentation last Dermatology Week touched on itch disorders such as notalgia paresthetica and uremic pruritus. Beyond AD and PN, which conditions do you believe will benefit most from ongoing therapeutic developments?
Dr Kim: For uremic pruritus in dialysis, we already have difelikefalin approved. We now have a proof of concept that it can be treated, and I think there is more to come. I remain very optimistic about it, although there is not a lead candidate right now in clinical trials that I am aware of. The other area that is huge right now is chronic pruritus of unknown origin (CPUO), and we have dupilumab in phase 3 clinical trials. CPUO has drawn a lot of interest from other companies as well. I think this is because the condition is just much better understood now.
What we have learned is that sometimes when you do a phase 3 clinical trial in a condition like PN, which is not well understood, suddenly the disease becomes much better understood. You have a lot of trial sites and investigators, who are also practicing dermatologists, now aware of the condition. They start talking about it and they see more of it in clinic because it is being advertised that we are now doing trials in this condition. We saw it with PN, and I think we are seeing this with CPUO. Why is everyone interested all of a sudden? I think because we have a phase 3 clinical trial that has been going on now for a bit of time.
The Dermatologist: Looking ahead, what do you see as the most pressing research questions in the field of itch, and how can dermatologists contribute to advancing this area of medicine in clinical practice?
Dr Kim: The reality is that most itch conditions start when someone did not itch before and then suddenly they do, and it just will not go away. So, in my mind, the biggest question in itch is: Where is the memory of itch embedded into the nervous system? Is it in the peripheral nervous system? The spinal cord? The brain? And if we discover that, how can we induce amnesia to the itch with a new therapy?
An example of a neuromodulatory drug is a medication called suzetrigine, which is a NaV1.8 blocker that is now approved for acute pain. This is a great proof of concept where a channel that is only expressed in the nervous system can be exploited to block pain. These are the kinds of modalities we want to see in itch, where we are selectively blocking the nervous system, and nothing else, and being able to shut down itch. To me, doing that with itch is the holy grail. We have not done it yet, but this is the future of what science needs to bring to dermatology. I think there is hope that in the next 5 years, we will have newer agents which are by design for itch and truly tailored in that way.
Disclosure: Dr Kim is co-founder of Alys Pharmaceuticals and Neurommune Therapeutics; he has served as a consultant for ABRAX Japan, AbbVie, Amgen, Attovia Therapeutics, Cara Therapeutics, Clexio Biosciences, Eli Lilly and Company, Escient Pharmaceuticals, Evommune, Galderma, Gilead, LEO Pharma, Micreos, Novartis, Pfizer, Recens Medical, Regeneron, Sanofi, Septerna, Teva Pharmaceuticals, and Triveni Bio; he has stock in ABRAX Japan, Alys Pharamaceuticals, Attovia Therapeutics, Locus Biosciences, Neurommune Therapeutics, Recens Medical, and Triveni Bio; and he holds a patent for the use of JAK1 inhibitors for chronic pruritus.










