What Is This Pigmented Lesion?
Case Report
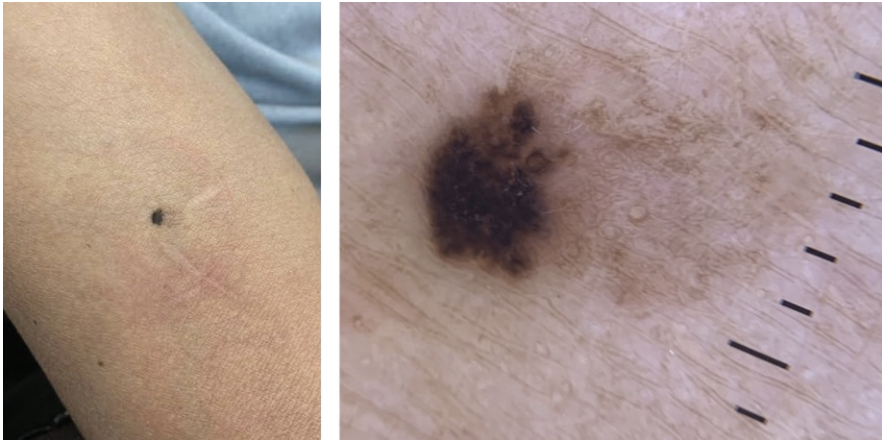
A 63-year-old man with Fitzpatrick skin type III presented to clinic with an asymptomatic 6-mm x 6-mm, brown-black, asymmetric macule and surrounding light brown patch on the left anterior upper arm (Figure 1a). The lesion had been slowly growing over the past 6 years. Dermoscopic findings were notable for amorphous brown pigmentation with brown dots at the periphery and some dotted vessels (Figure 1b). Punch biopsy was done for diagnosis.
What’s Your Diagnosis?™
Check your answer below!
Diagnosis
Pigmented Bowen’s Disease
Bowen’s disease, a type of squamous cell carcinoma in situ (SCCIS), is a rare intraepithelial carcinoma most commonly seen in men ages 60 to 70 years. The characteristic presentation includes an erythematous, well-demarcated, asymptomatic plaque, although atypical presentations are present, such as verrucous, hyperkeratotic, atrophic, and pigmented morphologies. The lesion is typically slow growing and can be present for multiple years before being seen in the clinical setting.
While Bowen’s disease is commonly associated with exposure to sun, arsenic, and human papillomavirus (HPV), it is important to note that risk factors among patients with darker skin differ. Chronic scarring and inflammatory conditions, such as hidradenitis suppurativa and lupus erythematosus, are commonly associated with SCC, with as many as 20% to 40% of SCC cases in patients with darker skin reported to be linked to chronic scarring and inflammatory processes.1,2 Patients with darker skin tones are also more likely to have SCC in non-sun exposed regions than individuals with lighter skin.1,3,4
Pigmented Bowen’s disease comprises only 1.7% of Bowen’s cases.3 Despite the higher prevalence of pigmented SCCIS among patients with dark skin types,3 there is a lack of diversity in images and a paucity of research on the dermoscopic findings of SCC in patients with darker skin tones.
Clinical Presentation and Histology
A valuable tool during physical examinations for diagnosing pigmented Bowen’s disease, dermoscopy can be useful for distinguishing it from common differential diagnoses in patients with darker skin types.5 Cameron et al. reported on the dermoscopic features of 52 cases of pigmented Bowen’s disease, noting that one of the most common features is a structureless pattern, with or without dotted patterns.6 They found that 83% of cases had a structureless pattern, and 42% additionally showed dotted patterns.6 Another large case series by Inskip et al. evaluated the dermoscopic findings of 79 pigmented Bowen’s lesions on the head and neck area, which showed that 54.4% of cases only had 1 pattern and 40.5% presented with a structureless pattern.7 Interestingly, Cameron et al. observed vessels in the majority of cases (67%).6 Similarly, Bugatti et al. reviewed 14 cases of pigmented SCC and reported atypical vascular structures in 87%,8 and Inskip et al. reported visible vessels in 49.4% of their cases, as well as scaling in 21.5% of cases.7 All cases reported by Inskip et al. had a brown color in combination with at least 1 additional color (gray, pink/red, white), with only 1 case presenting with a brown color alone. In 88.6% of the 79 cases, there was an asymmetry in the distribution of colors, often accompanied by areas of hypopigmentation or hyperpigmentation.7
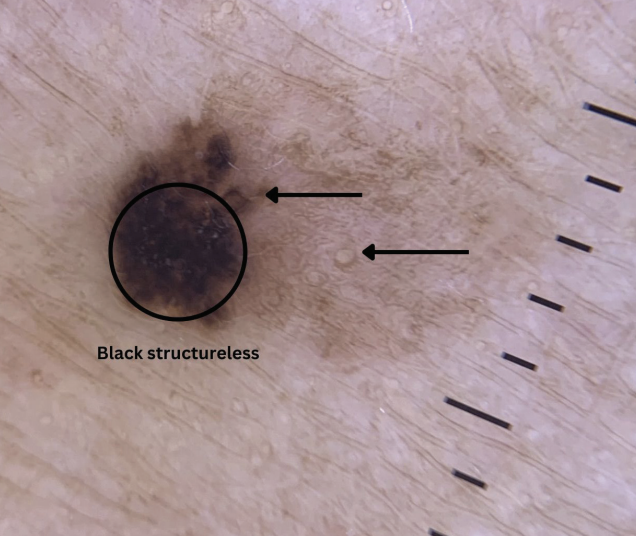
Patients with darker skin types are diagnosed with nonmelanoma skin cancers less frequently than those with lighter skin types but these skin cancers are associated with higher morbidity and mortality in individuals with darker skin tones.1 Given that patients with skin of color often experience worse outcomes, dermatologists should be able to recognize these cases to enhance early detection and improve outcomes. In our case, we observed a brown-black structureless area with a peripheral pigment network with brown circles, which was suggestive of pigmented Bowen’s disease (Figure 2).
Differential Diagnosis
The main differential diagnosis for this patient was atypical nevus. Other differential diagnoses for pigmented lesions include melanoma, seborrheic keratosis, melanocytic nevus, and pigmented basal cell carcinoma.5
Treatment
Treatment of Bowen’s disease may include topical chemotherapy agents, photodynamic therapy, electrodesiccation and curettage, or surgical excision.
Our Patient
Although Bowen’s disease can be associated with sun exposure, arsenic, and HPV, our patient did not report any of these exposures. Dermoscopic findings showed an amorphous brownish pigmentation, with brown dots at the periphery and some dotted vessels noted. No scaling or ulceration were present. In our case, punch biopsy confirmed the diagnosis as pigmented Bowen’s disease, which also ruled out alternative diagnoses concerning for melanoma. Following diagnosis, the neoplasm was excised.
Conclusion
Pigmented Bowen’s disease should be considered on the differential diagnosis in patients with pigmented lesions.
References
1. Gloster HM Jr, Neal K. Skin cancer in skin of color. J Am Acad Dermatol. 2006;55(5):741-60; quiz 761-764. doi:10.1016/j.jaad.2005.08.063
2. Agbai ON, Buster K, Sanchez M, et al. Skin cancer and photoprotection in people of color: a review and recommendations for physicians and the public. J Am Acad Dermatol. 2014;70(4):748-762. doi:10.1016/j.jaad.2013.11.038
3. Ragi G, Turner MS, Klein LE, Stoll HL Jr. Pigmented Bowen’s disease and review of 420 Bowen’s disease lesions. J Dermatol Surg Oncol. 1988;14(7):765-769. doi:10.1111/j.1524-4725.1988.tb01161.x
4. Halder RM, Bang KM. Skin cancer in blacks in the United States. Dermatol Clin. 1988;6(3):397-405.
5. Woo T, Naert K, Chia JC. Pigmented squamous cell carcinoma in situ with amyloid deposition mimicking melanoma. JAAD Case Rep. 2022;27:137-139. doi:10.1016/j.jdcr.2022.07.028
6. Cameron A, Rosendahl C, Tschandl P, Riedl E, Kittler H. Dermatoscopy of pigmented Bowen’s disease. J Am Acad Dermatol. 2010;62(4):597-604. doi:10.1016/j.jaad.2009.06.008
7. Inskip M, Cameron A, Akay BN, et al. Dermatoscopic features of pigmented intraepidermal carcinoma on the head and neck. J Dtsch Dermatol Ges. 2020;18(9):969-976. doi:10.1111/ddg.14220
8. Bugatti L, Filosa G, De Angelis R. Dermoscopic observation of Bowen’s disease. J Eur Acad Dermatol Venereol. 2004;18(5):572-574. doi:10.1111/j.1468- 3083.2004.01008.x