What Is This Yellowish, Erythematous Papule?
Case Report

A 91-year-old African American man with no significant past medical history and no history of skin cancer presented to the dermatology clinic for evaluation of a small, painless papule on his left eyelid of unknown duration. He denied any associated symptoms. On examination, the patient was found to have a round, 3-mm x 3-mm, erythematous papule with a yellowish hue and telangiectasias on the left eyelid, just below his left eyebrow (Figure 1).
What is your diagnosis?
Check your answer below
Diagnosis:
Endocrine Mucin-Producing Sweat Gland Carcinoma
Endocrine mucin-producing sweat gland carcinoma (EMPSGC) is a rare, low-grade, cutaneous adnexal neoplasm with neuroendocrine differentiation.1 It is considered to be a precursor of primary cutaneous mucinous carcinoma, of the neuroendocrine subtype, and is homologous to solid papillary/endocrine ductal carcinoma in situ of the breast, according to the World Health Organization’s 2018 classification.2,3 Since its first description in 1997, less than 200 cases of EMPSGC have been reported in the literature.4
Although it is more frequent in White women between ages 60 and 70 years in the periorbital region, EMPSGC has also been described in men under age 60 years and over age 80 years in extra-eyelid localizations (cheek, temple, and scalp) and in extra-facial localizations (chest and scrotum).3 Clinically, EMPSGC typically presents as a slow-growing, nonspecific, flesh-colored nodule or papule that can resemble a hidradenoma or cyst, with an average lesion size of 9 mm.1,5
Until recently, EMPSGC had not been known to metastasize. Although uncommon, there have been a few case reports cited in the literature of patients developing regional metastases, commonly to the parotid, that developed 9 to 10 years after primary diagnosis and excision with negative margins of the primary eyelid EMPSGC.4 Additionally, there are reports of EMPSGC with locoregional metastasis to the salivary glands, and 1 report of metastasis to lymph nodes, viscera (pancreas), and bone.6,7 There is also evidence of a cutaneous mucinous carcinoma of the right eyelid that metastasized to the lung and was reclassified as an EMPSGC when the excisional biopsy was revisited 8 years later.8 These cases of metastasis were described in both patients with and without an associated mucinous carcinoma diagnosed previously.6-8 Also, a small observational study theorized that a lesion concerning for possible metastasis of EMPSGC may be part of a multicentric primary mucinous carcinoma.9
However, it is generally characterized by indolent growth and has a favorable prognosis.1,2 Recurrence rates vary based on its association with underlying mucinous carcinoma.4 In a review by Au et al. of 190 cases of EMPSGC, 35.7% were associated with mucinous carcinoma.5 Overall recurrence rate was found to be 8.4% and for EMPSGC with associated cutaneous mucinous carcinoma, 12.3%.4,5
Histopathology
Histologic examination of EMPSGC typically reveals basaloid nodules that are composed of medium-sized, bland, round to oval cells with central nuclei and moderately abundant eosinophilic cytoplasm. As the name implies, there is both intracellular and extracellular mucin production, resulting in a mucinous basophilic stroma and a variably bluish hue to some cells. Microcysts and pools of mucin can be seen. Occasional glandular structures may also be observed. Definitive diagnosis requires immunohistochemical staining.1 Evidence has shown that EMPSGC expresses cytokeratin AE1/AE3, CAM 5.2, CK7, and EMA, but also GCDFP-15 and E-cadherin with high concordance, together with at least 1 neuroendocrine differentiation marker, such as synaptophysin, chromogranin A, neuron-specific enolase, and/or CD56. This entity also expresses estrogen receptors and progesterone receptors in most cases.3
Differential Diagnosis
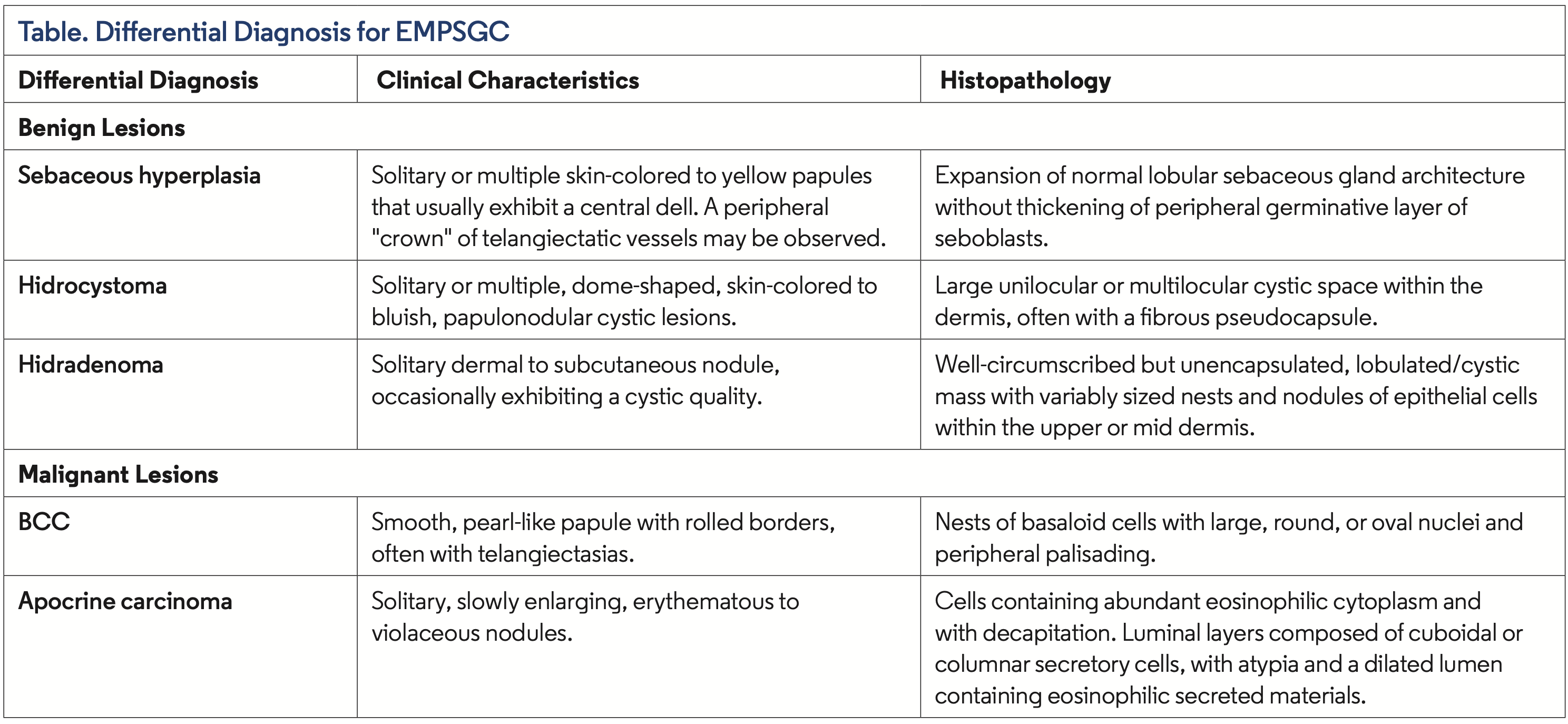
Due to the nonspecific clinical presentation, the differential diagnosis for EMPSGC is broad. Both benign and malignant neoplasms should be considered, such as hidradenoma, hidrocystoma, cystadenoma, mucinous carcinoma, apocrine carcinomas, and basal cell carcinoma (BCC) (Table). It may also be misdiagnosed as an inflammatory lesion, such as chalazion, or as a benign finding like sebaceous hyperplasia, resulting in delayed intervention.5 Given that EMPSGC most often occurs in individuals with lighter skin tones, this may present a diagnostic challenge for those caring for patients of color; changes in pigmentation and features like telangiectasia may be more difficult to visualize in patients with Fitzpatrick skin phototypes IV–VI.
Management of Localized and Metastatic EMPSGC
Regardless of metastatic potential, EMPSGC at primary sites can be locally aggressive and recur, so treatment via complete excision with wide margins or Mohs micrographic surgery (MMS) is recommended.1 Studies show lower rates of recurrence with MMS (6.25%) when compared to surgical excision (13.5%).5 MMS appears to be an appropriate treatment for EMPSGC due to its predilection for cosmetically sensitive areas and because there is a risk of associated and co-existent invasive mucinous carcinoma.10 Due to similar morphological and immunohistochemical features (positivity for neuroendocrine and estrogen receptor/progesterone receptor markers) with some forms of breast cancer, some advocate ruling out breast metastasis for all patients with a clinical and radiographic workup, even in the case of in situ EMPSGC lesions.11 Surgical resection of metastatic lesions is recommended along with close clinical follow up, but chemotherapy and radiation may also be considered.7,8,12
Our Patient
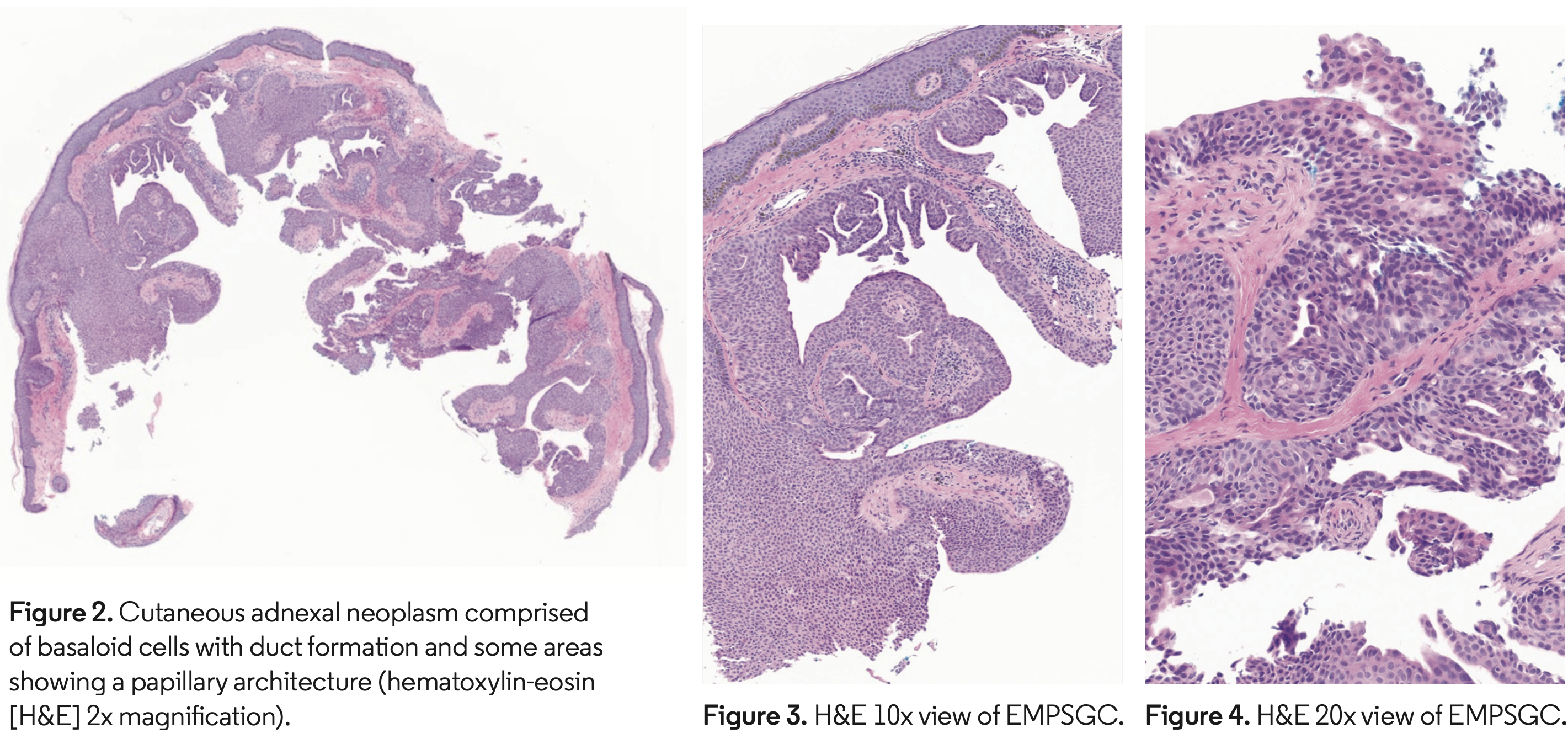
Our patient’s skin examination was most concerning for BCC, but sebaceous hyperplasia was also high on the differential diagnosis. A shave biopsy of the lesion was performed, and pathology showed skin with a cutaneous adnexal neoplasm comprised of basaloid cells with duct formation and some areas showing a papillary architecture, confirming the diagnosis of EMPSGC (Figures 2–4). Immunohistochemical staining was not performed. The patient was treated with MMS, and negative margins were achieved in 1 stage. The defect was closed with an intermediate layered repair and the patient tolerated the procedure well without complications. The patient was advised to return in 6 months for a regular skin examination.
Conclusion
Given the rarity and nonspecific presentation of EMPSGC, biopsy is necessary for diagnosis. EMPSGC should be on the differential diagnosis for any patient with an unassuming, slow-growing, flesh-colored lesion, especially in the periorbital region. EMPSGC can be easily confused with other neoplasms or benign conditions, particularly in individuals with darker skin tones where examination findings may be less conspicuous, potentially leading to treatment delays. Delay to diagnosis is especially important to be aware of in patients of color, as disparities in access to dermatologic care disproportionately affect minority populations.13 Once diagnosed, complete excision is recommended with close clinical follow up due to the risk of recurrence and the potential association of EMPSGC with invasive mucinous carcinoma.
At Baylor College of Medicine in Houston, TX, Angelique Ruml is a medical student, Ibeth Caceres is a medical student, Dr Fernandez is a micrographic surgery and dermatologic oncology fellow in the department of dermatology, Dr Workman is a dermatology resident in the department of dermatology, Dr Huttenbach is an assistant professor in the department pathology and immunology, Dr Shimizu is an associate professor in the department of dermatology, and Dr Ranario is an asssistant professor in the department of dermatology.
Disclosure: The authors report no relevant financial relationships.
References
- Shimizu I, Dufresne R, Robinson-Bostom L. Endocrine mucin-producing sweat gland carcinoma. Cutis. 2014;93(1):47-49.
- Hadi R, Xu H, Barber BR, Shinohara MM, Moshiri AS. A case of endocrine mucin-producing sweat gland carcinoma with distant metastasis. J Cutan Pathol. 2021;48(7):937-942. doi:10.1111/cup.13999
- Cazzato G, Bellitti E, Trilli I, et al. Endocrine mucin-producing sweat gland carcinoma: case presentation with a comprehensive review of the literature. Dermatopathology (Basel). 2023;10(3):266-280. doi:10.3390/dermatopathology10030035
- Sarangi J, Konkimalla A, Kaur K, Sikka K, Sen S, Kakkar A. Endocrine mucin producing sweat gland carcinoma with metastasis to parotid gland: not as indolent as perceived? Head Neck Pathol. 2022;16(1):331-337. doi:10.1007/s12105-021-01353-1
- Au RTM, Bundele MM. Endocrine mucin-producing sweat gland carcinoma and associated primary cutaneous mucinous carcinoma: review of the literature. J Cutan Pathol. 2021;48(9):1156-1165. doi:10.1111/cup.13983
- Chang MH, Wu CH. Cytological findings in a case of endocrine mucin-producing sweat gland carcinoma with metastasis to salivary glands. Cytopathology. 2023; 34(4):381-384. doi:10.1111/cyt.13239
- Shah M, Aman A, Srinivaas K, Gudipati A, Chavali P. Endocrine mucin-producing sweat gland carcinoma of the peno-scrotum with systemic metastases: a rare case report. Indian J Pathol Microbiol. 2021;64(1):180-182. doi:10.4103/IJPM. IJPM_342_19
- Fournier JE, Russell C, Hossain M. Metastatic endocrine mucin-producing sweat gland carcinoma to the lung: a case report. Cureus. 2023;15(11):e49711. doi:10.7759/cureus.49711
- Ravi PY, Walsh NM, Archibald C, Pasternak S. Endocrine mucin-producing sweat gland carcinoma: emerging evidence of multicentric cutaneous origin and occasional concurrence with analogous breast tumors. Am J Dermatopathol. 2022;44(5):321-326. doi:10.1097/DAD.0000000000002132
- Tannous ZS, Avram MM, Zembowicz A, et al. Treatment of synchronous mucinous carcinoma and endocrine mucin-producing sweat gland carcinoma with Mohs’ micrographic surgery. Dermatol Surg. 2005;31(3):364-367. doi:10.1111 /j.1524-4725.2005.31091
- Agni M, Raven ML, Bowen RC, et al. An update on endocrine mucinproducing sweat gland carcinoma: clinicopathologic study of 63 cases and comparative analysis. Am J Surg Pathol. 2020;44(8):1005-1016. doi:10.1097/ PAS.0000000000001462
- Grushchak S, Barlow T, Palla B, Mannor GE, Greenway HT, Kelley BF. Endocrine mucin-producing sweat gland carcinoma and primary cutaneous mucinous carcinoma: a case series. Cutis. 2023;112(3):E6-E10. doi:10.12788/cutis.0856
- Vaidya T, Zubritsky L, Alikhan A, Housholder A. Socioeconomic and geographic barriers to dermatology care in urban and rural US populations. J Am Acad Dermatol. 2018;78(2):406-408. doi:10.1016/j.jaad.2017.07.050