


Eczema in the United States: Insights from a National Study on Prevalence and Co-Occurrence
© 2025 HMP Global. All Rights Reserved.
Any views and opinions expressed are those of the author(s) and/or participants and do not necessarily reflect the views, policy, or position of The Dermatologist or HMP Global, their employees, and affiliates.

https://nationaleczema.org/visual-guide/
© 2002-2025 National Eczema Association, All rights reserved.
Eczema refers to a group of inflammatory skin conditions with distinct clinical characteristics that affect over 10% of Americans. While atopic dermatitis (AD) is the most commonly recognized form, eczema also includes allergic and irritant contact dermatitis (ACD and ICD), seborrheic dermatitis (SD), dyshidrotic eczema, chronic hand eczema, nummular eczema, neurodermatitis, and stasis dermatitis. Each type has specific clinical features, although symptoms frequently overlap, and many individuals may be diagnosed with multiple types throughout their lives.
A cross-sectional analysis of the National Institutes of Health All of Us (AoU) database provides a detailed real-world snapshot of how different types of eczema coexist in adult patients.1 The findings highlight both the prevalence of co-occurring eczema diagnoses and the necessity to adapt treatment strategies to address this complexity.
A Closer Look at the Cohort
Researchers examined electronic health record (EHR) data from 266,612 participants in the AoU database. Among these, 25,672 adults (9.6%) had at least one eczema diagnosis. Compared with those without eczema, affected individuals were significantly more likely to be women (62.9% vs 60.6%), older (mean age 61.3 vs 57.9 years), White (63.0% vs 53.7%), and non-Hispanic (81.9% vs 77.0%). This large, diverse dataset enabled investigators to track not just the prevalence of individual eczema subtypes but also how often different diagnoses co-occurred in the same patient. Nearly 1 in 5 adults with eczema (18.2%) had more than one eczema subtype documented.
Seborrheic Dermatitis and Atopic Dermatitis Lead the Way
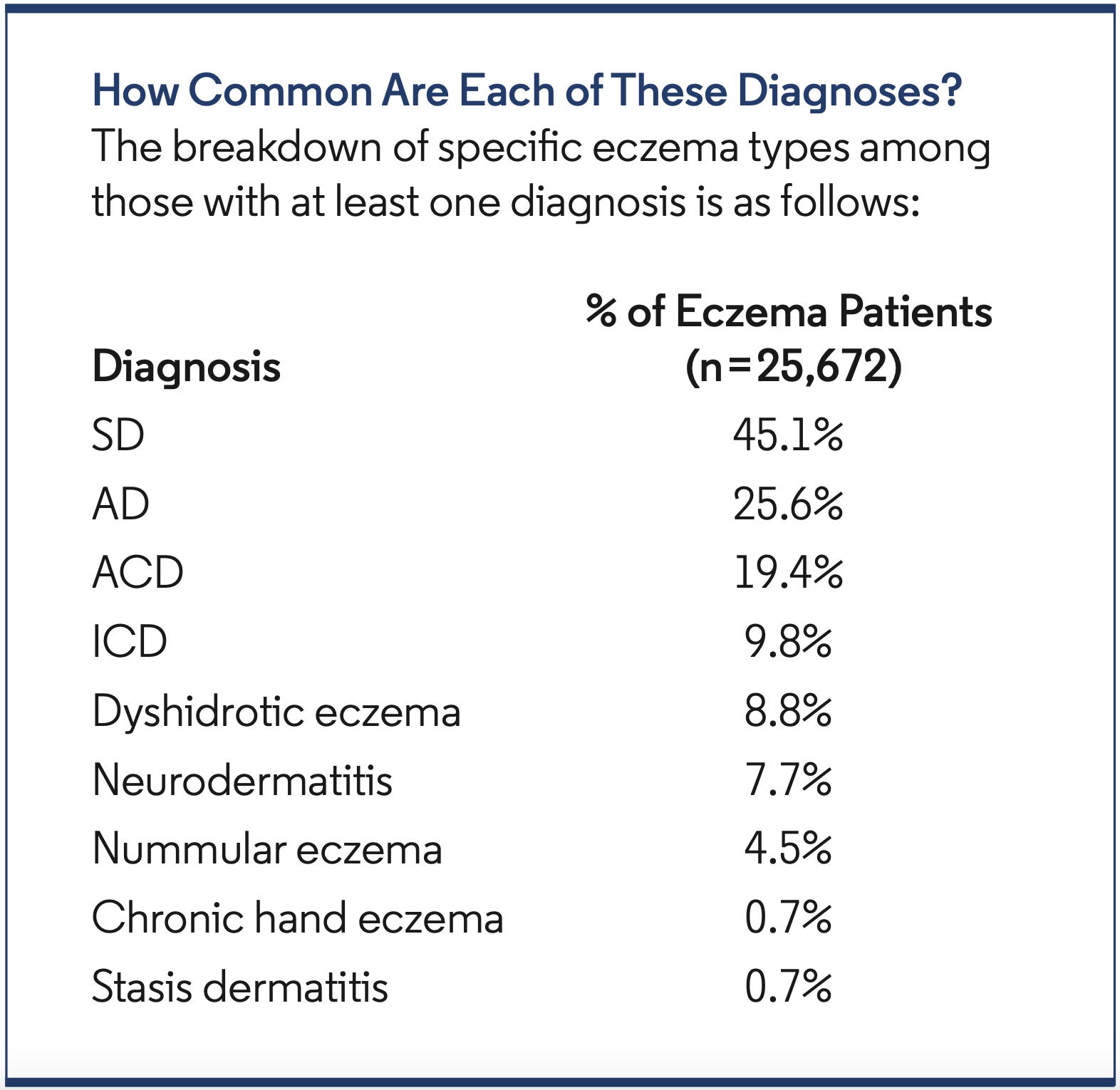
Among all eczema types, SD was the most common diagnosis in the AoU cohort, affecting 4.3% of participants (11,574 of 266,612). AD followed at 2.5% (6571 patients), with ACD at 1.9% and dyshidrotic eczema at 0.8%. ICD was seen in 0.9% of the total population. Among individuals with eczema, SD accounted for nearly half of all cases (45.1%), highlighting its broad prevalence. Despite often being treated as a separate entity in dermatology, SD was included in this study due to its clinical and pathophysiologic overlap with eczematous conditions.
Diagnostic Overlap Is Common
The analysis revealed patterns of diagnostic overlap. Among the 4669 patients with more than one eczema diagnosis:
- 25.9% (1212 individuals) had both AD and SD
- 15.3% (716 individuals) had ACD and SD
- 13.8% (647 individuals) had both AD and ACD
Chronological analysis of diagnosis coding revealed that among patients with AD and SD or AD and ACD, the AD diagnosis was typically recorded first in just under half of cases (48.9% and 53.8%, respectively). In contrast, SD tended to precede ACD in 60.2% of co-diagnosed cases. Among all individuals with multiple eczema diagnoses, SD was the most common initial diagnosis (33.1%).
Co-Occurrence Rates Across Eczema Types
Cross-tabulation of diagnoses revealed co-occurrence patterns. For instance, 18.4% of adults with AD also had SD, and 9.8% had ACD. Among those with SD, 10.5% also had AD, and 6.2% had ACD. Additionally, individuals with ACD often had co-diagnoses of ICD (15.2%) and SD (14.4%). These results highlight the frequent co-occurrence of contact dermatitis and SD with AD and other eczema types, emphasizing the need to consider coexisting conditions in diagnosis and treatment.
Implications for Clinical Practice
Eczema research and clinical trials, particularly those focused on AD, often exclude patients with coexisting skin conditions. Yet in real-world settings, many patients experience multiple eczema subtypes. These patients may respond differently to treatments than those with isolated AD or another singular form.
This study highlights the need for broader inclusion criteria in clinical trials and the development of treatment guidelines that account for co-occurring diagnoses. It also raises questions about whether standard monotherapies for AD, such as topical corticosteroids or biologics like dupilumab, offer equivalent benefit in patients who also have SD, ACD, or other eczematous conditions.
Real-World Prevalence Higher Than Previously Estimated
Earlier studies using more limited definitions of eczema found prevalence rates of 5.4% to 5.6% in the AoU dataset. However, this updated analysis, involving 62,799 additional participants and the inclusion of SD and other variants, found an overall prevalence of 9.6%. That is nearly 1 in 10 US adults with at least one documented eczema diagnosis. Interestingly, the prevalence of SD in this study (4.3%) aligns closely with global estimates (4.4%), lending credibility to the findings.
Challenges in Diagnosis and Coding
A key limitation of this study is the potential for misclassification due to overlapping features among eczema types. This is especially relevant for chronic hand eczema, for which no unique international classification of diseases ICD-10 code currently exists. In some cases, patients may receive multiple codes not because they have distinct conditions but to facilitate billing or meet insurance requirements.
Furthermore, the study did not validate diagnoses by reviewing full clinical records. As such, coding errors or inconsistencies cannot be ruled out, and future studies are needed to confirm the accuracy of electronic health record-based diagnostic labels.
Looking Ahead: The Need for Integrated Care
One of the most significant takeaways from this study is that nearly 1 in 5 adults with eczema has more than one subtype—a finding with major implications for treatment, research, and patient care. Patients with coexisting eczema conditions may require personalized care plans that go beyond standard protocols.
These real-world data reinforce the importance of moving toward integrated, patient-centered dermatologic care. They also provide a strong rationale for expanding clinical trials to include patients with multiple eczema diagnoses so treatment outcomes can reflect the real-life experiences of the broader patient population.
Conclusion
The co-occurrence of multiple eczema types is far from rare and affects thousands of adults across the United States. This may significantly influence their clinical course and treatment outcomes. As more comprehensive data become available, clinicians, researchers, and policymakers must work together to update diagnostic frameworks, therapeutic guidelines, and trial inclusion criteria to better reflect the multifaceted nature of eczema in the real world.
Reference
- Loiselle AR, Johnson JK, Smith Begolka W. Prevalence and co-occurrence of eczema types in adults in the United States: insights from the All of Us research program. J Invest Dermatol. 2025:S0022-202X(25)00297-0. doi:10.1016/j.jid.2025.02.136
