

Right Subclavian Artery Aneurysm: A First for the Bahamas
Abstract
Subclavian artery aneurysms (SAA) are very uncommon and occur in <1% of the population. The first case ever identified in the Bahamas is presented because the etiology is unclear at this time. The aneurysm was repaired by a single supraclavicular incision by aneurysmorrhaphy. The patient had an uneventful postoperative course. Most SAA are caused by atherosclerosis and despite a histological finding of myxoid degeneration, doubt still surrounds this particular aneurysm because of the patient’s age and lack of risk factors.
VASCULAR DISEASE MANAGEMENT 2011;8(8):E138–E140
Key words: subclavian artery aneurysm
___________________________________________
Introduction
This case represents the first documented Bahamian experience with a right SAA. A literature review on the management of this rare vascular entity follows.
Case Report
 A 33-year-old female presented for evaluation of a right neck swelling that was present for more than 2 years. This swelling was pulsatile and enlarged whenever she exercised or became overly emotional. She described several syncopal episodes with exertion and right upper limb fatigue with prolonged use. She gave no history of trauma and had no other risk factors for vascular disease.
A 33-year-old female presented for evaluation of a right neck swelling that was present for more than 2 years. This swelling was pulsatile and enlarged whenever she exercised or became overly emotional. She described several syncopal episodes with exertion and right upper limb fatigue with prolonged use. She gave no history of trauma and had no other risk factors for vascular disease.
Significant examination findings revealed a pulsatile neck mass approximately 4 cm x 4 cm in the right supraclavicular area and a normal neuromuscular exam of the right upper extremity.
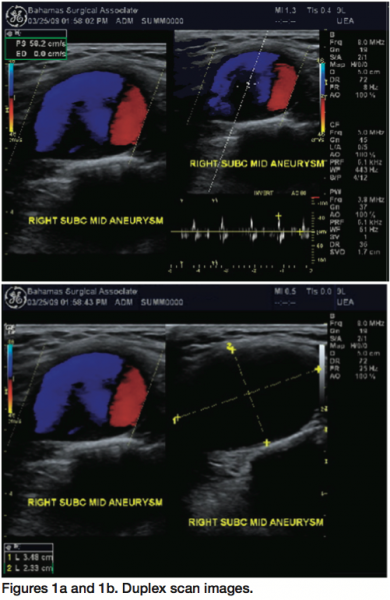
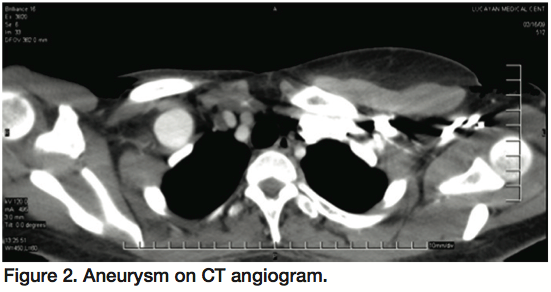
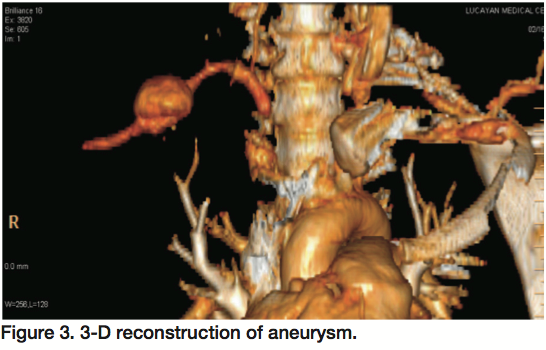
The patient was investigated with a chest x-ray, arterial duplex scan, and a CT angiogram of the right upper extremity and chest. The chest x-ray was normal as was the blood investigation. The duplex scan and CT angiogram with 3D reconstruction confirmed a saccular right SAA distal to the first rib and in the mid segment of the artery. Other vascular beds were negative for aneurysms.
An interventional radiologist suggested an endovascular approach, although he did express some concerns about stent placement and risk of stent fracture. A conventional angiogram was not performed at this time.
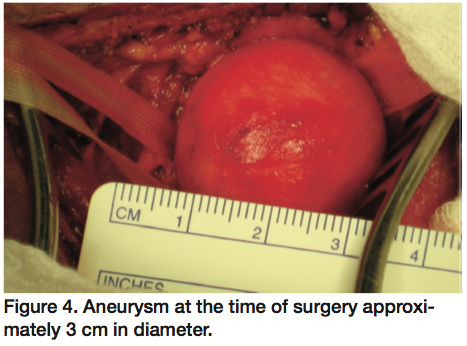
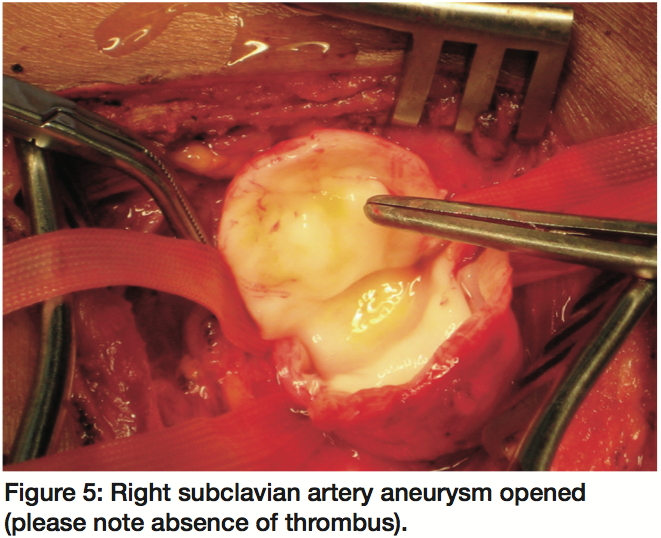
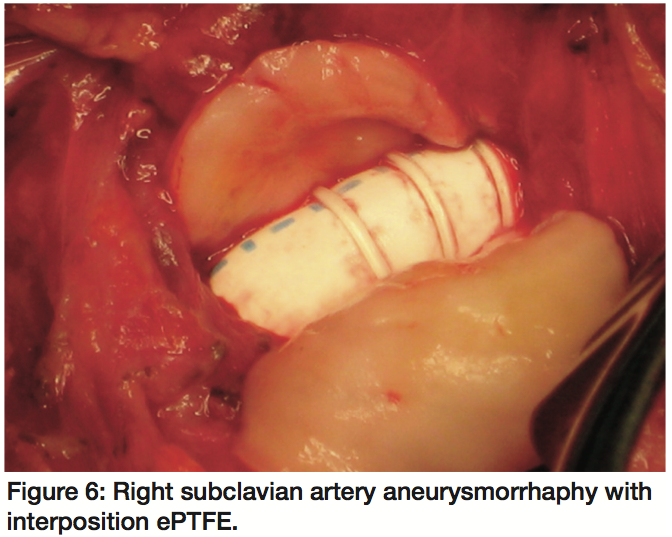
 The patient opted for open surgical repair. A single incision was made in a curvilinear fashion along Langer’s lines of the neck. The right subclavian artery proximal and distal to the aneurysm was dissected and isolated. After systemic heparinization, the vessel was clamped proximally and distally. The aneurysm sac was opened. An aneurysmorrhaphy was completed with externally supported ePTFE 8 mm interposition graft (W.L. Gore & Associates, Flagstaff, Arizona). Of note, there was no evidence of atherosclerosis in the aneurysm at surgery. The sac was closed over the graft.
The patient opted for open surgical repair. A single incision was made in a curvilinear fashion along Langer’s lines of the neck. The right subclavian artery proximal and distal to the aneurysm was dissected and isolated. After systemic heparinization, the vessel was clamped proximally and distally. The aneurysm sac was opened. An aneurysmorrhaphy was completed with externally supported ePTFE 8 mm interposition graft (W.L. Gore & Associates, Flagstaff, Arizona). Of note, there was no evidence of atherosclerosis in the aneurysm at surgery. The sac was closed over the graft.
 The patient had an uneventful postoperative course and remained asymptomatic on follow-up. Follow-up duplex scans revealed a patent graft with no evidence of stenosis. Pathological review of the aneurysm sac showed myxoid degeneration.
The patient had an uneventful postoperative course and remained asymptomatic on follow-up. Follow-up duplex scans revealed a patent graft with no evidence of stenosis. Pathological review of the aneurysm sac showed myxoid degeneration.
Discussion
True SAA are rare.1 They represent a significant risk for rupture, embolization, or thrombosis, and therefore should be considered for surgical treatment.2 These aneurysms are rarely seen in the clinical setting and represent <1% of all peripheral artery aneurysms. In a 1995 review, Dougherty et al found 64 patients with 70 SAA reported in the literature since 1926.3 Dent et al reviewed the location of atherosclerotic aneurysms in 1,488 patients, with isolated subclavian lesions occurring in only 2 patients (0.13%).1
The most common etiology of true SAA is atherosclerosis, accounting for 60% of the reported cause, followed by infectious aneurysms (syphilis, 15%;4 tuberculosis, 10%;5 bacterial, few). Marfan syndrome6 and cystic medial necrosis7 represented 10% of the cases.8-10 True aneurysm of the distal part of the subclavian artery is mostly poststenotic, belonging to the thoracic outlet syndrome (TOS), but it is very rare. In literature, the incidence is approximately 1.1% in patients with TOS.11 The other cause is trauma, Turner’s Syndrome,10 Behçet’s disease,12 aortitis syndrome13 and congenital arterial disease.14
 Most patients with SAA are asymptomatic. When symptomatic they may be related to distal embolization and thrombosis. Typically, painful punctate lesions affect the fingers and palm.15 Patients can also present with pressure symptoms from an enlarging pulsatile mass or rarely with dysphagia, respiratory distress, or hemoptysis.16
Most patients with SAA are asymptomatic. When symptomatic they may be related to distal embolization and thrombosis. Typically, painful punctate lesions affect the fingers and palm.15 Patients can also present with pressure symptoms from an enlarging pulsatile mass or rarely with dysphagia, respiratory distress, or hemoptysis.16
Diagnosis of SAA can be easily accomplished with clinical history and physical examination. The advances in duplex scan have enabled clinicians to use noninvasive methods to isolate and identify these aneurysms. CT scanning is also useful, but routine CT scan does not provide sufficient detail for complete diagnosis. Reconstruction techniques using 3-D imaging can be used to demonstrate the entire cervical vasculature allowing visualization of all arteries connecting to the aneurysm.17 Conventional angiography is the gold standard and has always been mandatory for planning surgical management. This may not completely or always demonstrate the distal subclavian artery in some cases because of contrast medium dilution.17 MRI/MRA is also useful and transesophageal echocardiogram has also been utilized.18 A conventional angiogram was not done in this case.
 Open surgery is the classic method of therapy for SAA. The surgical approach to the extrathoracic SAA is often feasible through the combined supra- and infraclavicular incisions. In our case, a single supraclavicular approach was successfully used. Right-sided intrathoracic SAA is approached through a median sternotomy, whereas left-sided aneurysms can be approached through a high left posterolateral thoracotomy.
Open surgery is the classic method of therapy for SAA. The surgical approach to the extrathoracic SAA is often feasible through the combined supra- and infraclavicular incisions. In our case, a single supraclavicular approach was successfully used. Right-sided intrathoracic SAA is approached through a median sternotomy, whereas left-sided aneurysms can be approached through a high left posterolateral thoracotomy.
In TOS, removal of a cervical rib or resection of the first rib should be performed prior to the procedure for an aneurysm. The axillary approach is suitable for distal aneurysm. Other neurological structures are preserved along with the thoracic duct. Several authors have successfully described treatment using endovascular techniques.19,20,21 Others have reported using a combined open and endovascular approach.22 Reports on stent graft treatment of SAA have dealt mostly with pseudoaneurysms in the setting of iatrogenic or penetrating traumatic injuries. The advantages of this procedure include a minimally invasive approach, shortened hospitalization, and cost effectiveness. While this treatment modality is technically feasible, widespread utilization is not employed because of the rarity of the problem and the scarcity of information regarding long-term outcomes of stent grafts in this area.
 In the early reports, operations for SAA were limited to simple ligation without revascularization.23 Repair of these aneurysms has been attempted by several other techniques, which include partial excision of the sac and repair by aneurysmorrhaphy or a patch repair with prosthetic material. Resection of the aneurysm and revascularization is currently the common procedure. Arterial reconstruction options include anatomic reconstruction with interposition graft, primary end-to-end anastomosis, and extra-anatomic reconstruction such as carotid-subclavian transposition or bypass grafting.
In the early reports, operations for SAA were limited to simple ligation without revascularization.23 Repair of these aneurysms has been attempted by several other techniques, which include partial excision of the sac and repair by aneurysmorrhaphy or a patch repair with prosthetic material. Resection of the aneurysm and revascularization is currently the common procedure. Arterial reconstruction options include anatomic reconstruction with interposition graft, primary end-to-end anastomosis, and extra-anatomic reconstruction such as carotid-subclavian transposition or bypass grafting.
Conclusion
A right SAA was successfully repaired using an open technique with a single supraclavicular incision. The ease of recognition, appropriate investigations, and proper surgical technique ensure a good clinical outcome. Although the endovascular approach is becoming more feasible, long-term outcome data are limited and so this must be used with caution and experience.
References
- Dent TL, Lindenauer SM, Ernst CB, Fry WJ. Multiple arteriosclerotic arterial aneurysms. Arch Surg 1972;105(2):338–344.
- Pairolero PC, Walls JT, Payne WS, Hollier LH, Fairbairn JF 2nd. Subclavian-axillary artery aneurysms. Surgery 1981;90(4):757–763.
- Dougherty MJ, Calligaro KD, Savarese RP, DeLaurentis DA. Atherosclerotic aneurysm of the intrathoracic subclavian artery: A case report and review of the literature. J Vasc Surg 1995;21(3):521–529.
- Daniel RA Jr. Syphilitic aneurysm of the subclavian artery. Ann Surg 1951;134(2):251–258.
- Hara M, Bransford RM. Aneurysm of the subclavian artery associated with contiguous pulmonary tuberculosis. J Thorac Cardiovasc Surg 1963;46:256–264.
- Coselli JS, Crawford ES. Surgical treatment of aneurysms of the intrathoracic segment of the subclavian artery. Chest 1987;91(5):704–708.
- Fee HJ, Gewirtz HS, O’Connell TX, Grollman JH. Bilateral subclavian artery aneurysm associated with idiopathic cystic medial necrosis. Ann Thorac Surg 1978;26:387–390.
- Bahnson HT. Definitive treatment of saccular aneurysms of the aorta with excision of sac and aortic suture. Surg Gynecol Obstet 1953;96:383–402.
- Applebaum RE, Caniano DA, Sun CC, Azizkhan RA, Queral LA. Synchronous left subclavian and axillary artery aneurysms associated with melorheostosis. Surgery 1986;99(2):249–253.
- Akasaka T, Mitsuishi T, Nakajima H, Suzuki R, Shimizu S. Aneurysm of the left subclavian artery associated with Turner’s syndrome. Successful surgical treatment. J Cardiovasc Surg (Torino) 1989;30(6):945–947.
- Utíkal P, Bachleda P, Köcher M, et al. Aneurysm of the subclavian artery. Acta Univ Palacki Olomuc Fac Med 1999;142:107–109.
- Okita Y, Ando M, Minatoya K, Kitamura S, Matsuo H. Multiple pseudoaneurysms of the aortic arch, right subclavian artery, and abdominal aorta in a patient with Behçet’s disease. J Vasc Surg 1998;28(4):723–726.
- Nishimori H, Hirose K, Fukutomi T, et al. A subclavian artery aneurysm associated with aortitis syndrome. Jpn J Thorac Cardiovasc Surg 1999;47(12):621–624.
- Stahl RD, Lawrence PF, Bhirangi K. Left subclavian artery aneurysm: Two cases of rare congenital etiology. J Vasc Surg 1999;29(4):715–718.
- Nehler MR, Taylor LM Jr, Moneta GL, Porter JM. Upper extremity ischemia from subclavian artery aneurysm caused by bony abnormalities of the thoracic outlet. Arch Surg 1997;132(5):527–532.
- Wu MH, Lai WW, Lin MY, Chou NS. Massive hemoptysis caused by a ruptured subclavian artery aneurysm. Chest 1993;104(2):612–613.
- Hirose SM, Hadama T, Iwata E, et al. Atherosclerotic aneurysm of the intrathoracic segment of the subclavian artery: A case report. Ann Thorac Cardiovasc Surg 2000;6(4):281–284.
- Shah A, Katz ES, Stern A, Tunick PA, Kronzon I. Isolated subclavian artery aneurysm: Evaluation by transesophageal echocardiography. Echocardiography 2004;21(1);73–76.
- Iannelli G, Di Tommaso L, Monaco M, Piscione F. Endovascular treatment of right-sided subclavian artery aneurysm in a congenitally malformed aortic arch. J Thorac Cardiovasc Surg 2005;129(3):682–684.
- Kedora J, Grimsley B, Pearl G. Endovascular treatment of an aberrant right subclavian artery aneurysm with use of the Zenith iliac plug. Proc (Bayl Univ Med Cent) 2009 Apr;22(2):144–145.
- May J, White G, Waugh R, Yu W, Harris J. Transluminal placement of a prosthetic graft-stent device for treatment of subclavian aneurysm. J Vasc Surg 1993;18:1056–1059.
- Van Leemput A, Maleux G, Heye S, Nevelsteen A. Combined open and endovascular repair of a true right subclavian artery aneurysm without proximal neck. Interact CardioVasc Thorac Surg 2007;6(3):406–408.
- Thomas TV. Intrathoracic aneurysms of the innominate and subclavian arteries. J Thorac Cardiovasc Surg 1972;63(3):461–471.
___________________________________________
From the Princess Margaret Hospital, The University of the West Indies, Doctors Hospital, Nassau, Bahamas.
The author reports no financial relationships or conflicts of interest regarding the content herein.
Manuscript submitted November 25, 2010, provisional acceptance given December 17, 2010, final version accepted January 18, 2011.
Address for correspondence: Princess Margaret Hospital, The University of the West Indies, Doctors Hospital, Surgery, P.O. Box GT 2373, #5 Albury Lane, Nassau, Bahamas. Email: deltonfarquharson@yahoo.com

