



Accelerating Patient Transitions From Hospital to Home in the United Kingdom With Single-Use Negative Pressure Wound Therapy: A Discharge Pathway
© 2025 HMP Global. All Rights Reserved.
Any views and opinions expressed are those of the author(s) and/or participants and do not necessarily reflect the views, policy, or position of Wounds or HMP Global, their employees, and affiliates.
Abstract
Background. Initially limited to inpatient use, negative pressure wound therapy (NPWT) is now frequently used in community settings. However, complexities in wound management step-down strategies in the United Kingdom, including regional variations in referral processes, lack of consensus on funding criteria, and limited availability of NPWT units, have led to extended hospital length of stay (LOS) for patients ready for discharge but still needing NPWT. Single-use NPWT (sNPWT) can serve as a bridge between hospital and community NPWT. Objective. To assess the feasibility, effectiveness, and potential cost savings of the implementation of a discharge pathway utilizing sNPWT. Methods. This case series included 5 patients with open lower limb wounds treated at a National Health Service facility using an sNPWT discharge pathway. Wounds were assessed before and after sNPWT use. Differences in average inpatient LOS and costs were calculated and compared with those for patients who remained hospitalized until community NPWT was available. Results. The sNPWT discharge pathway was well tolerated by patients and resulted in good clinical outcomes. Patients discharged on sNPWT had an average reduction in LOS of 20.2 days, resulting in a projected £12 350 savings in hospital costs per patient. Conclusion. Preliminary findings indicate use of an sNPWT discharge pathway is feasible and may result in reduced LOS and associated costs while improving patient care. Additional studies are needed to understand the effect on wound management, patient outcomes, and overall care costs.
The incidence of wounds and related treatment costs has been increasing in the United Kingdom and across the globe over the last decade.1-3 A study using 2017-2018 data estimated that the National Health Service (NHS) treats over 3.8 million patients with wounds per year at a cost of over £8.3 billion annually.3 These numbers likely are increasing given the aging population, the growing prevalence of chronic diseases that impede wound healing, and increasing numbers of infected wounds that require hospitalization.4 The increased need for inpatient wound care is problematic given that 19 out of 20 NHS hospital beds are currently occupied and growing waiting lists exist for elective surgeries.5,6
Fortunately, there have been continual advances in wound care management.1 Negative pressure wound therapy (NPWT) emerged in the mid-1990s as a means to improve management of chronic and acute wounds.7,8 NPWT can facilitate healing through continuous drainage, wound bed stabilization, the ability to draw wound edges together, and stimulation of tissue growth.9-11 The therapy is commonly used to help prepare larger at-risk wounds for delayed closure in most surgical specialties.8 Many studies have demonstrated improved patient outcomes with NPWT use, including increased rates of wound healing and reductions in time to wound closure, dressing changes, operating room visits, risk of amputation, and length of stay (LOS).1,12-15 NPWT options have broadened over the years and include NPWT with instillation and dwell time (NPWTi-d), which provides additional wound cleansing through the periodic instillation of topical wound solutions directly over the wound bed followed by removal with negative pressure, and closed incision negative pressure therapy to manage the incisions of patients at risk for developing surgical complications.7,16
Initially limited to inpatient use, NPWT is being used more frequently in community settings.1,17 Research has shown that treatment with NPWT outside the hospital is safe and cost-effective.1,17,18 Additionally, use of NPWT in community settings may allow patients to be discharged from the hospital sooner, return to the comfort of their own home, and resume some of their normal everyday activities.1,17 By discharging patients on NPWT, hospitals also can free up beds for patients who need inpatient care, thus increasing patient throughput and reducing wait times.19 However, there is a need for a clear pathway for use of NPWT from hospital discharge to community care.17
In the United Kingdom, challenges and complexities in the process of organizing out-of-hospital advanced wound management therapies such as NPWT delay the transition of patients from inpatient to the community and hinder the initiation and adoption of community NPWT. There are significant barriers to obtaining community NPWT. The referral process varies across each region within the United Kingdom, no consensus on funding criteria exists, and often there are not enough NPWT units available at the acute hospital to give to patients at discharge.
Incompatible consumable components across the different NPWT manufacturers further compounds this issue. In certain regions of London, England, it takes an average of 18 days—nearly 3 weeks—to complete enrollment in community NPWT and secure an NPWT device; thereafter, responsibility is handed over to the community team and the patient is discharged. As a result, patients on NPWT who are otherwise ready for discharge must remain in the hospital for an extended period on hospital NPWT, while waiting for funding, approval, delivery of units and consumables, and availability of suitably skilled staff in the community nursing teams. There are many consequences to a prolonged inpatient stay, including delayed mobility and return to baseline functionality, negative effects on mental health, and potential loss of employment and housing.20 Additionally, the unnecessary prolonged LOS for patients on NPWT results in reduced bed capacity for elective procedures and other more acute patients.19
Single-use NPWT (sNPWT) can serve as a bridge between hospital NPWT and community NPWT, allowing for patients to be discharged home as soon as wound management is achievable in an outpatient setting. An sNPWT discharge pathway was created to transition patients receiving wound care with inpatient NPWT to community NPWT. The feasibility, effectiveness, and effect on hospital costs of this strategy were assessed through a small case series of 5 patients.
Methods
This case series examined 5 representative patients with open lower limb wounds who were managed with the sNPWT discharge pathway from June through November 2023 by a surgeon (M.J.P.) at the Royal Free Hospital, a vascular hub in London, England. The objective was to investigate the feasibility of the pathway and its effect on inpatient LOS, length of NPWT, wound healing, and costs of care. Written consent was obtained from the patients for the use of the included case studies and photographs.
Inpatient treatment
Inpatient treatment was guided by an existing wound management emergency transfer pathway. Surgical management was indicated for patients presenting with wet gangrene, purulent discharge from a deep source, fluctuant collections or abscess, tissue crepitus, and/or radiographic evidence of soft tissue gas. Immediate treatment included empirical antibiotic therapy and sepsis source control surgery with abscess drainage, drain insertion, debridement, and/or amputation based on the surgeon’s clinical assessment. Revascularization was performed, if indicated, using an endovascular, open, or hybrid approach. Endovascular approaches included aortoiliac, superficial femoral artery, popliteal, and below-knee interventions. Open approaches included endarterectomy and bypass.
NPWT (3M ActiV.A.C. Therapy Unit with 3M V.A.C. Granufoam Dressing; Solventum Corporation) was applied to the patients on the vascular ward to manage exudate, reduce edema, improve granulation tissue formation and local tissue perfusion, and reduce the need for surgical debridement. NPWTi-d (3M Veraflo Therapy; Solventum Corporation) was indicated for and applied to wounds that were infected, had heavy biofilm, required further debridement due to thick slough or fibrinous exudates, and/or were poorly granulating. NPWTi-d was also indicated for large cavities that required extensive granulation or for granulation over structures such as tendons and bones. Normal saline was used for the instillation with a 10-minute dwell time, followed by 2-hour cycles of negative pressure at −125 mm Hg. Dressing changes occurred every 72 hours. Patients who received NPWTi-d were stepped down to NPWT once thick slough and fibrinous exudates were removed and other wound end points such as granulation tissue volumes had been met. Patients continued to receive NPWT in the hospital with dressing changes every 72 hours. Patients without indications for NPWT, or with contraindications as per the instructions for use (including malignancy; untreated osteomyelitis; unexplored fistulae; presence of necrotic eschar; or exposed vessels, vascular grafts, organs, or nerves), did not receive NPWT and were ineligible for the sNPWT discharge pathway.
Discharge pathway with sNPWT
The discharge pathway for accelerating transitions for patients on NPWT from hospital to home is depicted in Figure 1. Once the patient meets hospital discharge criteria other than the need for continued NPWT, the patient is informed about the possibility of discharge with sNPWT. If consent is obtained, a nurse completes the community NPWT referral and a ward nurse replaces the patient’s NPWT device with sNPWT.
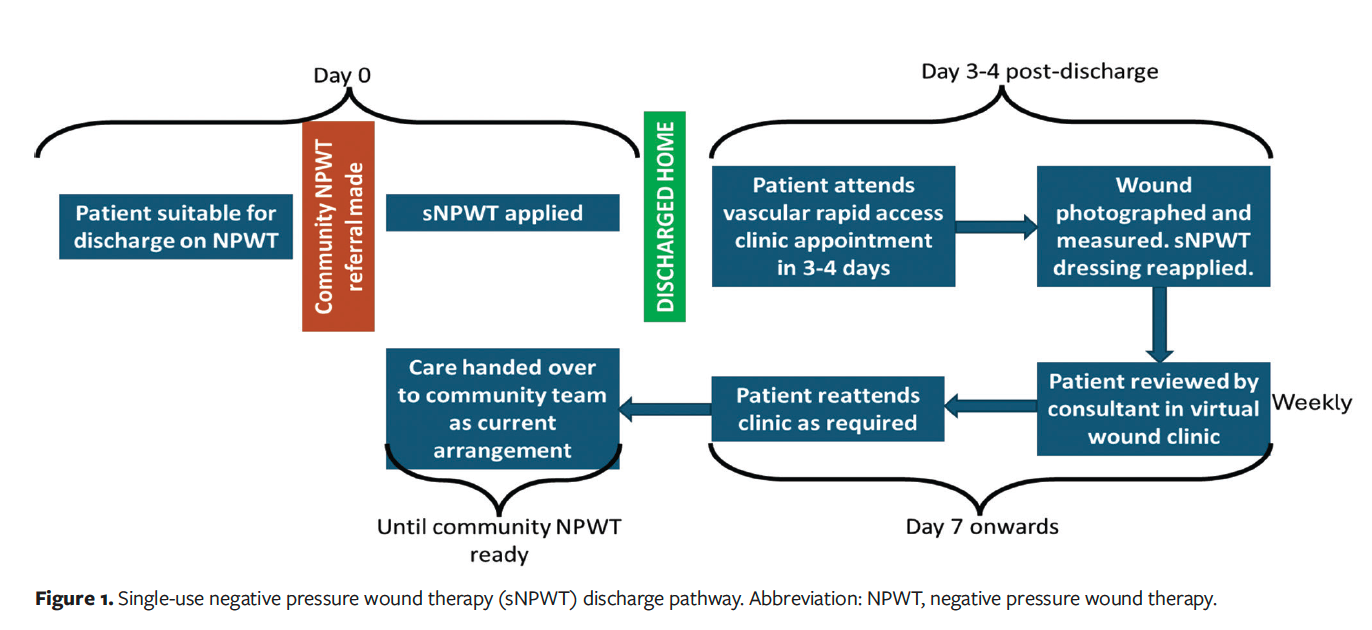
A key component of the discharge pathway is the sNPWT device. The patients in this case series were treated with the 3M Prevena Plus 125 Therapy Unit (Solventum Corporation). This compact, portable device is now indicated for use in open wounds. When used with compatible dressings, sNPWT is intended to create an environment that promotes wound healing by secondary or tertiary (delayed primary) intention by preparing the wound bed for closure, reducing edema, promoting granulation tissue formation and perfusion, and removing exudate and infectious material.
Once the sNPWT device has been placed, the patient is scheduled for a vascular rapid access clinic appointment in 3 to 4 days, given an information leaflet on the sNPWT device and emergency contact number, and discharged home. At the vascular rapid access clinic appointment, the wound is photographed and measured and the NPWT dressing is changed. The patient reattends the clinic as required until they can be discharged to community wound care services and NPWT delivery or they no longer require NPWT.
Cost analysis
The effect of the sNPWT discharge pathway on inpatient utilization and costs was assessed by comparing average LOS for patients who were treated with the pathway to average LOS for patients who were treated at the same facility in the months prior to pathway implementation and who remained hospitalized until community NPWT was available. Potential cost savings were calculated by multiplying the difference in LOS between groups by the average cost of one night of an inpatient stay.
Results
The following case studies describe the transition of patients from inpatient NPWT at the Royal Free Hospital in London to community NPWT using sNPWT.
Patient 1
A 57-year-old male with a history of type 1 diabetes mellitus, retinopathy, and neuropathy presented acutely with a 1-week history of a deteriorating right hallux infection (Figure 2A). He was clinically unwell, pyrexial, and tachycardic. The patient was immediately started on intravenous antibiotics guided by local protocols and underwent a same-day hallux amputation (Figure 2B). NPWT was applied on postoperative day 2 (Figure 2C). After 72 hours of NPWT, antibiotics were changed to oral equivalents for an intended duration of 6 weeks, and the patient was discharged home ambulatory with sNPWT. After 14 days, sNPWT was discontinued (Figure 2D). A community NPWT unit was delivered the following day, 15 days after hospital discharge. The wound completely healed after 3 months (Figure 2E).

Patient 2
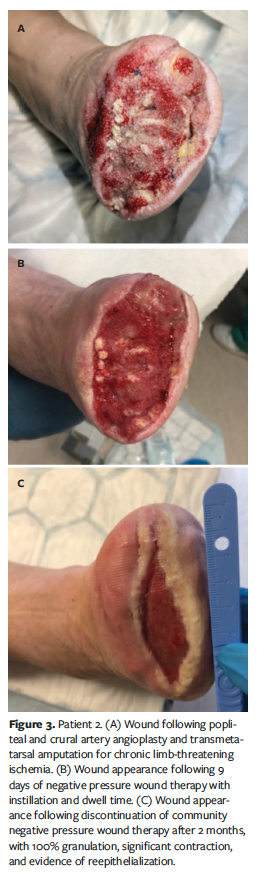
A frail 88-year-old male was transferred to the vascular hub from his local hospital with chronic limb-threatening ischemia presenting as painful gangrenous toes. He had a history of peripheral artery disease, severe aortic stenosis awaiting transcatheter aortic valve replacement, and ischemic heart disease with a 4-vessel coronary artery bypass graft 20 years prior. He underwent a popliteal and crural artery angioplasty and transmetatarsal amputation under regional anesthesia (Figure 3A). The patient received NPWTi-d using a reticulated open cell foam (ROCF) dressing with through holes for a total of 9 days (Figure 3B). To encourage mobility, he was transitioned to NPWT. After 5 weeks of medical optimization and inpatient physiotherapy, the patient was discharged home on sNPWT. A community NPWT unit was delivered 28 days post-discharge. NPWT was discontinued after 2 months by the community team with the wound having achieved 100% granulation, significant contraction, and evidence of reepithelialization (Figure 3C).
Patient 3
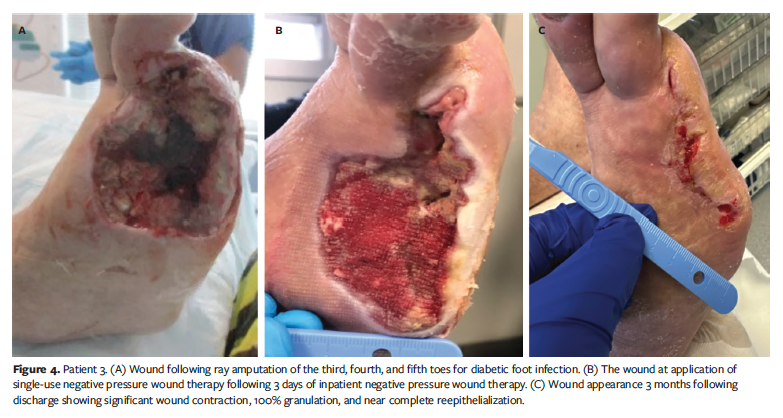
A 79-year-old female with type 2 diabetes mellitus, hypertension, ischemic heart disease, and peripheral artery disease underwent a fourth toe amputation for a diabetic foot infection. The patient presented again 5 weeks later with wet gangrene involving the third and fifth toes as well as the fourth toe amputation site. Imaging revealed osteomyelitis of the metatarsal heads of the third, fourth, and fifth toes. The patient was started on empirical antibiotics, and she underwent ray amputation of the third, fourth, and fifth toes (Figure 4A). She underwent a crural vessel angioplasty and received inpatient NPWT for 3 days. Because the patient was the main caregiver for her disabled husband, she wished to be discharged. The patient went home the same day on sNPWT (Figure 4B). A community NPWT was delivered on postoperative day 16. The appearance of the wound at 3 months showed significant wound contraction, 100% granulation, and near-complete reepithelialization (Figure 4C).
Patient 4
A 72-year-old male with type 2 diabetes mellitus, hypertension, and atrial fibrillation presented with a left diabetic foot infection. He had a collection on the plantar surface at the base of the fourth and fifth toes with spreading cellulitis over the dorsum. The patient was started on empirical intravenous antibiotics and underwent an emergency amputation of the fourth and fifth toes with a dorsal foot debridement as a sepsis source control procedure (Figure 5A). Four days after amputation there were no further signs of local infection, and NPWT was offered to the patient. He declined to stay in the hospital; therefore, sNPWT was applied and the patient went home immediately on oral antibiotics. The wound appearance at 14 days following initiation of sNPWT is shown in Figure 5B. The patient was transitioned to a community NPWT, and at 5 months after surgery, the wound had healed (Figure 5C).

Patient 5
An 80-year-old male with type 2 diabetes mellitus and peripheral artery disease was admitted with an extensive right dorsal foot collection and fifth toe wet gangrene. He underwent an emergency fifth toe amputation and drainage of the dorsal abscess (Figure 6A). Following a crural vessel angioplasty and at day 7 post-drainage, NPWTi-d using an ROCF dressing with through holes was initiated and used for 3 weeks (Figure 6B). After medical optimization, the patient was discharged home on sNPWT. At 14 days post-discharge, the wound was 90% covered with healthy granulation tissue and evidence of wound contracture was observed (Figure 6C). The patient was transferred to community NPWT, and the wound was healed 6 months after surgery (Figure 6D).

Cost analysis
The sNPWT discharge pathway has been used on a total of 68 patients as of this writing. The average LOS for patients has decreased by approximately 20.2 days following implementation of the discharge pathway compared with patients who did not receive sNPWT. The cost of 1 night of an inpatient stay is approximately £612; thus, use of the sNPWT pathway could save approximately £12 350 per patient through a reduction in bed days alone.
Discussion
Complexities in wound management step-down strategies in the United Kingdom have resulted in delayed transitions from inpatient to community NPWT use. One facility has used an sNPWT discharge pathway to bridge the gap between inpatient and community NPWT. The 5 case studies in the current series demonstrate the feasibility and potential cost savings of an sNPWT discharge pathway for patients with open wounds. Patients were successfully treated at home with an sNPWT device until community NPWT was available instead of remaining hospitalized when they were otherwise clinically ready for discharge. The patients’ wounds improved following use of NPWT and sNPWT, with 3 patients experiencing complete wound healing within 2 to 6 months. No adverse outcomes or problems with sNPWT were reported. Patients treated with the sNPWT discharge pathway had an average reduction in LOS of 20.2 days, resulting in an estimated hospital cost savings of approximately £12 350 per patient.
These preliminary findings align with those from a recent study by Rossato et al19 examining the clinical outcomes and potential cost savings of a hospital-at-home (H@H) NPWT service for 2 NHS hospitals allowing patients to be discharged with NPWT (RENASYS; Smith and Nephew) or sNPWT (PICO; Smith and Nephew) provided in the home until the wound reepithelialized. Most of the 31 treated wounds were amputation sites, diabetic foot ulcers, or abscesses in the lower extremities. After a mean hospital stay of 13.7 days, patients were discharged to H@H care, with most patients (93.5%) receiving NPWT for an average of 29.2 days. Statistically significant reductions in wound area and volume from baseline were observed at weekly follow-up visits. Thirty of the 31 patients were discharged from the H@H service without further need for NPWT treatment. The estimated cost savings per day of providing NPWT at home vs in the hospital was £180, resulting in an average cost savings of £5256 per patient.19
A distinguishing feature of the proposed discharge pathway presented in this report is the use of sNPWT for all cases to facilitate the transition between hospital and community care. The sNPWT device used in the study conducted by Rossato et al lacks a canister and was designed to manage low-to-moderate exudate volume and shallower wound dimensions.19 Thus, NPWT was deemed more suitable for most patients based on wound dimensions and exudate volume. Although Rossato et al19 claimed all of the wounds would have been suitable to step across to sNPWT, most of the patients were not transitioned from NPWT to sNPWT per clinical judgment. The sNPWT device used in the current case series has a replaceable canister that holds 150 mL, allowing for the management of exudating wounds without the dressings becoming saturated, thus reducing the need for frequent changes. It provides continuous negative pressure of −125 mm Hg in contrast to the −80 mm Hg of pressure delivered by the device used in the Rossato et al19 study. Orlov and Gefen21 found that canister-based sNPWT delivered relatively greater continuous negative pressure by transporting excess fluid to the canister and was more likely to achieve better clinical outcomes than a canister-less system. In addition, the dressings and component connections used with the sNPWT unit with canister are compatible across the continuum of care, allowing for an easy transition between NPWT and sNPWT devices. The use of sNPWT for all patients transitioning between inpatient and community wound care also addresses the shortage of NPWT devices available upon discharge within the NHS.
The sNPWT discharge pathway aligns with the NHS goals of accelerating discharge from hospitals and providing more care in community settings, including wound care with NPWT.5,17 The NHS Long Term Plan states that when patients no longer need to be in a hospital bed, they should receive good health and social care support that allows them to return home.22 Despite NHS’s desire to provide NPWT in community settings, there are many barriers, and widespread implementation has not occurred.17 The sNPWT discharge strategy provides an actionable framework for transitioning patients from inpatient to community NPWT without the need for sweeping organizational change.
Most importantly, the sNPWT discharge pathway provides patient-centered care and allows patients to continue treatment in the comfort of their own homes. In a qualitative study, Monsen et al23 reported several benefits of transitioning from the inpatient setting to home on NPWT. Patients expressed relief at being home in their normal environment and preferred sleeping in their own bed, not being disturbed by others, and having the ability to resume everyday life. Two patients in the current case series requested to be discharged as soon as possible. One patient was the primary caregiver for her disabled husband and needed to return home to manage his care. In addition, accelerating discharge from the hospital can help patients avoid depression and limit exposure to hospital-acquired illnesses and infections.24 Patients have reported that a key component to having a positive experience with NPWT was the feeling of being well prepared at discharge.23 In the current case series, as part of the sNPWT
discharge pathway, patients received education and an informative leaflet as well as continued support and care from the vascular access clinic and the virtual wound clinic.
Although this sNPWT discharge pathway addresses specific barriers to continuation of NPWT at home in the United Kingdom, challenges regarding reimbursement, device procurement, and access to adequate outpatient or in-home wound care are common in other regions and may result in delays in discharge and prolonged hospital LOS for patients. In a survey, clinicians and procurement/equipment managers from Australia, France, Germany, Italy, the United States, and the United Kingdom indicated that it was difficult and time-consuming to manage patient discharge on NPWT, that there were disagreements over billing, and that the fleet of NPWT devices were frequently lost, not properly stored, or went unused.25 A lack of patient monitoring systems and nurses specialized in NPWT application have also been cited as barriers to discharge on NPWT.25,26 Transitioning a patient from inpatient to outpatient NPWT may be more or less cumbersome in certain countries due to differences in health care infrastructure and payment systems. Discharge planning is pivotal in moving wound management beyond acute care settings, navigating reimbursement, and ensuring that patients have appropriately timed discharge with access to NPWT as they move across the care continuum, but processes often vary by facility.25
In the United States, NPWT devices are covered as durable medical equipment by Medicare and some private insurance policies, along with home health services that can assist with NPWT and wound care. NPWT devices may be available on-site for patient discharge at some facilities, but equipment-related delays are common and may contribute to unnecessary increases in LOS.27 Device manufacturers may offer programs to facilitate placing of orders and insurance authorization as well as device consignment that allow for on-site home care equipment to be provided to the patient at or before discharge without interrupting therapy and preventing unnecessary dressing changes.27 Outpatient NPWT is organized and financed differently across Europe, and despite evidence of its effectiveness and a general shifting of inpatient care to outpatient settings, adoption has been limited.17,28 In many regions, the hospital remains responsible for providing and financing the treatment after care is moved to the outpatient setting, and patients are manually monitored through hospital visits for dressing changes.28 This model may streamline the transition of NPWT to the home by reducing care handoffs and simplifying billing.
Discharging patients on sNPWT may expedite and improve the transition from inpatient to outpatient care, particularly when NPWT devices are difficult to obtain. However, selection of NPWT and sNPWT devices and timing of transitions should be dependent on a myriad of factors, including therapeutic goals, wound characteristics, patient satisfaction and quality of life, care settings, economic implications, and evidence.26 Differences among countries, regions, and facilities in the organization of care and the availability of community wound care resources may prevent the establishment of a common approach to providing NPWT outside the hospital, but additional research regarding when to use NPWT and sNPWT that considers differences in operational and financial factors is needed to promote effective use of these therapies.25 The establishment of hospital-level discharge policies and care pathways is key to ensuring successful care transitions and providing the best care for patients receiving NPWT, and the sNPWT discharge pathway provides an example of optimizing NPWT care with available resources.
Limitations
This is a small case series of 5 patients and has inherent limitations. All patients were treated by 1 vascular surgeon at 1 NHS facility, and the findings may not be generalizable to other settings. There was not a prospective comparison group because the sNPWT discharge pathway has been adopted as standard of care at the facility. The cost analysis was based on a retrospective comparison with patients who received care prior to implementation of the pathway, and it examined cost savings only in terms of reduction in bed days.
Conclusion
This case series provides early evidence that an sNPWT discharge pathway provides a clear and feasible step-down strategy compatible with a range of NPWT devices and advanced wound dressings for bridging the gap between hospital and community wound care. The pathway aligns with the NHS’s desire to reduce unnecessary hospital bed days and could result in cost savings. Most importantly, the sNPWT discharge pathway can optimize wound recovery for patients, allowing them to be discharged home in a timely manner. Larger studies across a variety of wound types are needed to validate these findings and investigate the cost-effectiveness of this strategy.
Author and Public Information
Authors: Mark J. Portou, PhD, FRCS1; Ashley W. Collinsworth, ScD, MPH2; and Siobhan Lookess, BSc, PGDip2
Affiliations: 1Royal Free London NHS Foundation Trust, London, UK; 2Solventum, Maplewood, MN, USA
Acknowledgments: The authors thank Julie M. Robertson, PhD (Solventum), for assistance with manuscript editing.
Disclosure: M.J.P. is a consultant for Solventum. A.W.C. and S.L. are employees of Solventum.
Ethical Statement: Written consent was obtained from the patients for the use of the included case studies and photographs.
Correspondence: Ashley Collinsworth, ScD, MPH; 12930 W Interstate 10, San Antonio, TX; acollinsworth@solventum.com
Manuscript Accepted: June 11, 2025
References
1. Dowsett C, Davis L, Henderson V, Searle R. The economic benefits of negative pressure wound therapy in community-based wound care in the NHS. Int Wound J. 2012;9(5):544-552. doi:10.1111/j.1742-481X.2011.00913.x
2. Guest JF, Fuller GW, Vowden P. Diabetic foot ulcer management in clinical practice in the UK: costs and outcomes. Int Wound J. 2018;15(1):43-52. doi:10.1111/iwj.12816
3. Guest JF, Fuller GW, Vowden P. Cohort study evaluating the burden of wounds to the UK's National Health Service in 2017/2018: update from 2012/2013. BMJ Open. 2020;10(12):e045253. doi:10.1136/bmjopen-2020-045253
4. Sen CK. Human wound and its burden: updated 2022 compendium of estimates. Adv Wound Care (New Rochelle). 2023;12(12):657-670. doi:10.1089/wound.2023.0150
5. National Health Service. Delivery Plan for Recovering Urgent and Emergency Care Services - January 2023. 2023. https://www.england.nhs.uk/long-read/delivery-plan-for-recovering-urgent-and-emergency-care-services-january-2023/
6. Warner M, Zaranko B. The Past and Future of NHS Waiting Lists in England. 2024. Accessed October 29, 2024. https://ifs.org.uk/publications/past-and-future-nhs-waiting-lists-england
7. Collinsworth AW, Griffin LP. The effect of timing of instillation therapy on outcomes and costs for patients receiving negative pressure wound therapy. Wounds. 2022;34(11):269-275. doi:10.25270/wnds/22013
8. Gupta S, Gabriel A, Lantis J, Téot L. Clinical recommendations and practical guide for negative pressure wound therapy with instillation. Int Wound J. 2016;13(2):159-174. doi:10.1111/iwj.12452
9. Anchalia M, Upadhyay S, Dahiya M. Negative pressure wound therapy with instillation and dwell time and standard negative pressure wound therapy in complex wounds: are they complementary or competitive? Wounds. 2020;32(12):E84-E91.
10. Diehm YF, Loew J, Will PA, et al. Negative pressure wound therapy with instillation and dwell time (NPWTi-d) with V. A.C. VeraFlo in traumatic, surgical, and chronic wounds-a helpful tool for decontamination and to prepare successful reconstruction. Int Wound J. 2020;17(6):1740-1749. doi:10.1111/iwj.13462
11. Kim PJ, Silverman R, Attinger CE, Griffin L. Comparison of negative pressure wound therapy with and without instillation of saline in the management of infected wounds. Cureus. 2020;12(7):e9047. doi:10.7759/cureus.9047
12. Apelqvist J, Armstrong DG, Lavery LA, Boulton AJ. Resource utilization and economic costs of care based on a randomized trial of vacuum-assisted closure therapy in the treatment of diabetic foot wounds. Am J Surg. 2008;195(6):782-788. doi:10.1016/j.amjsurg.2007.06.023
13. Driver VR, Blume PA. Evaluation of wound care and health-care use costs in patients with diabetic foot ulcers treated with negative pressure wound therapy versus advanced moist wound therapy. J Am Podiatr Med Assoc. 2014;104(2):147-153. doi:10.7547/0003-0538-104.2.147
14. Kaplan M, Daly D, Stemkowski S. Early intervention of negative pressure wound therapy using vacuum-assisted closure in trauma patients: impact on hospital length of stay and cost. Adv Skin Wound Care. 2009;22(3):128-132. doi:10.1097/01.ASW.0000305451.71811.d5
15. Gabriel A, Kahn K, Karmy-Jones R. Use of negative pressure wound therapy with automated, volumetric instillation for the treatment of extremity and trunk wounds: clinical outcomes and potential cost-effectiveness. Eplasty. 2014;14:e41.
16. Miller-Mikolajczyk C, Beach K, Silverman R, Cooper M. The evolution of commercial negative pressure wound therapy systems over the past three decades. Adv Wound Care (New Rochelle). 2024;13(8):375-390. doi:10.1089/wound.2023.0115
17. Apelqvist J, Fagerdahl A, Teot L, Willy C. Negative pressure wound therapy an update for clinicians and outpatient care givers. J Wound Management. 2024;25(2 Sup1):S1-S56. doi:10.35279/jowm2024.25.02.sup01
18. Santosa KB, Keane AM, Keller M, Olsen MA, Sears ED, Snyder-Warwick AK. Inpatient versus outpatient management of negative pressure wound therapy in pediatric patients. J Surg Res. 2020;254:197-205. doi:10.1016/j.jss.2020.04.025
19. Rossato M, Ryrie M, Robinson M, Searle R, Murdoch J. Use of NPWT as part of a Hospital @ Home wound management service. Journal of Community Nursing. 2021;35(4):50-57.
20. Rojas-García A, Turner S, Pizzo E, Hudson E, Thomas J, Raine R. Impact and experiences of delayed discharge: a mixed-studies systematic review. Health Expect. 2018;21(1):41-56. doi:10.1111/hex.12619
21. Orlov A, Gefen A. The potential of a canister-
based single-use negative-pressure wound therapy system delivering a greater and continuous absolute pressure level to facilitate better surgical wound care. Int Wound J. 2022;19(6):1471-1493. doi:10.1111/iwj.13744
22. National Health Service. The NHS Long Term Plan. 2019. https:/www.longtermplan.nhs.uk/publication/nhs-long-term-plan/
23. Monsen C, Acosta S, Kumlien C. Patients experiences of negative pressure wound therapy at home for the treatment of deep perivascular groin infection after vascular surgery. J Clin Nurs. 2017;26(9-10):1405-1413. doi:10.1111/jocn.13702
24. Tipton K, Leas BF, Mull NK, et al. AHRQ Comparative Effectiveness Technical Briefs. Interventions To Decrease Hospital Length of Stay. Agency for Healthcare Research and Quality (US); 2021.
25. Kirsner RS, Hurd T. Assessing the need for negative pressure wound therapy utilization guidelines: an overview of the challenges with providing optimal care. Wounds. 2020;32(12):328-333.
26. Hurd T, Kirsner RS, Sancho-Insenser JJ, et al. International consensus panel recommendations for the optimization of traditional and single-use negative pressure wound therapy in the treatment of acute and chronic wounds. Wounds. 2021;33(suppl 2):S1-S11.
27. Boti L, Soloway L, Myers D, Pillai D, Zabihi J. Decreased health care expenditure and average length of therapy with facilitated transition discharge program for patients receiving negative pressure wound therapy. Wounds. 2022;34(12):E118-E120. doi:10.25270/wnds/22050
28. Fagerdahl A. Organisation of NPWT in primary care in Europe – a descriptive survey. J Wound Management. 2023;24(2):3-5.







