Conservative Management of a Bullous Hematoma in the Case of von Willebrand Disease and Hemophilia A
© 2025 HMP Global. All Rights Reserved.
Any views and opinions expressed are those of the author(s) and/or participants and do not necessarily reflect the views, policy, or position of Wounds or HMP Global, their employees, and affiliates.
Questions
- How are trauma patients with von Willebrand disease, hemophilia, and anticoagulation unique, and why may this pose a challenge in hematoma management?
- What risk factors or criteria can be used to determine the severity of hematomas?
- What does conservative management of hematomas include?
- What surgical interventions are used to treat hematomas?
Case Description
A 67-year-old man with a history of von Willebrand disease (vWD), characterized by low ristocetin cofactor to von Willebrand factor antigen ratio and hemophilia A, presented to the emergency department 3 days after a motor vehicle accident. According to the injury report, the patient's left arm was in a crossed position when his knees hit the dashboard, resulting in swelling of the soft tissues and the formation of a hematoma. A physical examination and radiographic images revealed that the patient had a left ulnar fracture, comminuted 5th metatarsal fractures on the left side, and a large hematoma on the left pretibial region measuring 15 x 6 cm with a central bulla (Figure 1). Despite the injuries, the patient had a full range of motion in all joints with gross sensation intact and could move his lower extremities without discomfort. Radiographic imaging was unremarkable for fractures or significant soft tissue damage (Figure 2).
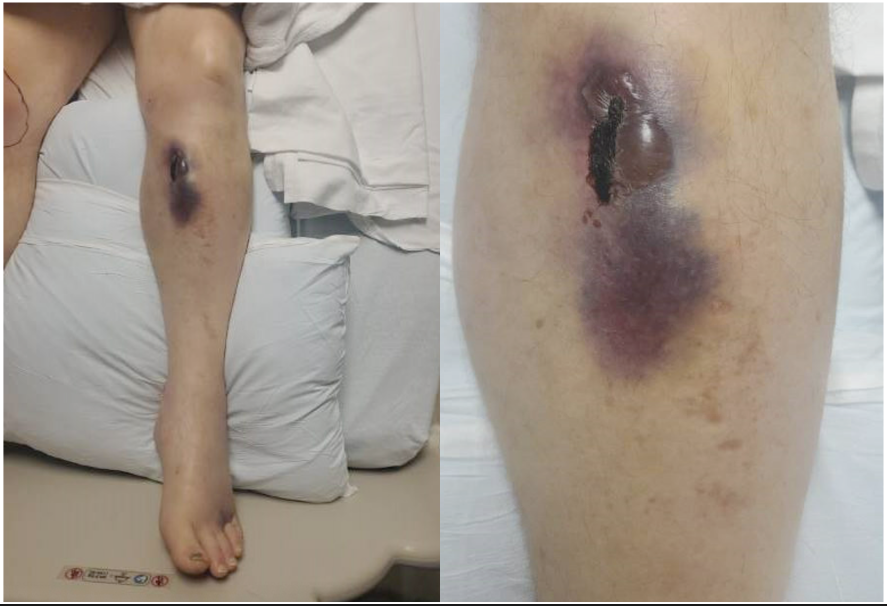
Figure 1. Moderate-sized hematoma measuring 15 × 6 cm. Raised discolored borders with bruising that is firm to palpation. A central bulla is present with some formation of eschar.

Figure 2. Proximal pretibial soft tissue swelling without acute bony injury.
Given the patient's history of von Willebrand disease, the plastic surgery team discussed the risks of draining the hematoma, the difficulty of controlling bleeding, and expanding skin necrosis. They recommended close observation and monitoring for demarcation, with follow-up in the clinic in a week. The hematoma was resolved well during the follow-up visit, with a small central area of skin necrosis (Figure 3). The wound appeared to be on pace for resolution and the patient was advised to return in a month. However, the patient was lost to follow-up, so the final outcome remains unknown.

Figure 3. Image of the pretibial region of the left lower extremity. A necrotic central eschar is present with a mild fluctuance without ecchymosis or edema.
Q1. How are trauma patients with von Willebrand disease, hemophilia, and anticoagulation unique, and why may this pose a challenge in hematoma management?
Individuals with vWD have deficiencies in von Willebrand factor, a protein crucial for normal blood clotting.1,2 This deficiency can lead to prolonged bleeding even from minor injuries, predisposing them to hematomas. Mucosal bleeding is a common manifestation that can potentially result in acute and life-threatening emergencies if not promptly addressed. Superficial bleeds in vWD may not always necessitate aggressive intervention. Hematomas exacerbate complications due to their tendency to grow and compress adjacent structures.3 Physicians need more education on different types of vWD patients, particularly in replacement therapy and formulation of a bleeding plan, because each phenotype requires a specialized approach.4,5
Similarly, patients with hemophilia experience impaired clot formation, resulting in prolonged and excessive bleeding.1,6 Hematomas in these patients can occur spontaneously or following trauma, posing a heightened risk of prolonged bleeding rendering them highly susceptible to complications.6 These hematomas can affect deep tissues such as muscles and joint spaces. Managing hematomas in hemophiliac patients often requires prompt clotting factor replacement therapy administration to facilitate clot formation and minimize bleeding.
Furthermore, trauma patients on anticoagulation therapy, such as warfarin or direct oral anticoagulants, have altered clotting factors and increased susceptibility to bleeding complications.3 Hematomas in these individuals can be particularly challenging to manage due to the need to balance the risk of bleeding with the risk of thrombosis. Reversal agents or antidotes may need to be administered to counteract the effects of anticoagulation and facilitate hematoma resolution.3,7-9
Achieving optimal patient outcomes and mitigating complications such as impaired mobility, compromised sensation, and blood supply requires a multidisciplinary approach.1,6,9 This approach often involves collaboration among hematologists and surgeons. Additionally, close monitoring is essential to prevent the escalation of pressure within hematomas, which can lead to complications like compartment syndrome and further vascular and neurological compromise.3,7,8
Q2. What risk factors or criteria can be used to determine the severity of hematomas?
The most appropriate management strategy for hematomas is for health care providers to evaluate the nature of the injury, the patient's age, and the use of anticoagulants.3,7 An increase in these risk factors may indicate a greater likelihood of deep tissue damage and potential internal degloving injuries. During the clinical examination of the injury site, health care professionals carefully assess for specific indicators such as edema, erythema, and evidence of open wounds.3 The use of ultrasound helps evaluate the development of fluid collections. The decision on whether to pursue conservative or surgical management is based on the presence of open wounds, active bleeding, the condition of the skin, and the extent of edema.3,7,8 The judgment of severity is mainly subjective, and attention to the patient's whole clinical picture is essential.
Q3. What does conservative management of hematomas include?
The conservative management of hematomas involves a careful, noninvasive approach to facilitate proper healing of the affected soft tissues. The initial step in conservative management is the combination of hydrogels and atraumatic debridement. This process focuses on creating an optimal wound bed for the healing of soft tissues.3 Gentle debridement is typically performed using monofilament-based pads to reduce the risk of infection.3,10 Hydrogels soften and prevent eschar formation and blood clots within the hematoma. It's important to note that debridement can be challenging for patients due to the potential discomfort caused by exposing sensitive nerve endings.10 This method avoids the need for skin grafting. However, conservative management does carry a risk of infection due to the moist environment created by hydrogels, which may promote bacterial growth if not carefully monitored. Additionally, the slow resolution of hematomas through conservative management can increase the risk of tissue necrosis if the hematoma persists for an extended period, leading to pressure on the surrounding tissues.
Research and studies have shown positive outcomes with conservative management. For example, a study involving 35 cases of pre-tibial hematoma managed conservatively demonstrated successful healing in all patients, with none developing necrosis or requiring blood transfusions.8 Interestingly, a significant portion of these patients did not need to return to the emergency room, even though some of them were at higher risk of bleeding due to anticoagulant medication usage.8 Conservative management helps decrease the risk of overlying skin necrosis, which can lead to total skin loss. This approach aims to promote effective soft tissue healing without invasive surgical procedures.
Q4. What surgical interventions are used to treat hematomas?
Surgical management involves performing a fasciotomy of the affected area to alleviate tension and prevent potential skin necrosis caused by closed hematomas.3,8 A suction device is used to evacuate the accumulated hematoma.3,7 During this process, intermittent irrigation with saline is utilized to cleanse the hematoma contents and maintain a clear view of the surgical site.11 Following this, hemostasis is achieved with electrocautery. Depending on the specific case, the surgeon may leave the laceration open to facilitate drainage, or close it instead.11 The decision to proceed with this surgical procedure is contingent upon the absence of additional risks, such as excessive bleeding and hematoma reformation. Hematoma reformation can exert significant tension on the surrounding skin, potentially leading to skin necrosis and serving as a source of infection.3,7,8 Further wound care may be required, extending the patient's hospitalization and rehabilitation. It is strongly advised to perform surgical intervention early if deemed appropriate.
Summary
The management of hematoma in patients with a prediction of bleeding requires a comprehensive discussion regarding the potential hazards associated with hematoma drainage. The determination of the appropriate course for hematoma management should revolve around the challenges of achieving hemostasis and mitigating the expansion of skin necrosis. In such scenarios, a vigilant approach encompassing close observation and gentle debridement of the superficial skin, coupled with hydrogels, can establish a secure and productive treatment strategy tailored to vWD and hemophilic patients. However, when managing hematomas in the presence of open fractures or exposed hardware, wound management may need to be more aggressive to prevent infection and ensure proper healing of the underlying structures. Subsequent clinic appointments should strongly emphasize monitoring wound healing progress and instituting measures for infection prevention, thus ensuring favorable and successful outcomes (Figures 5 and 6).
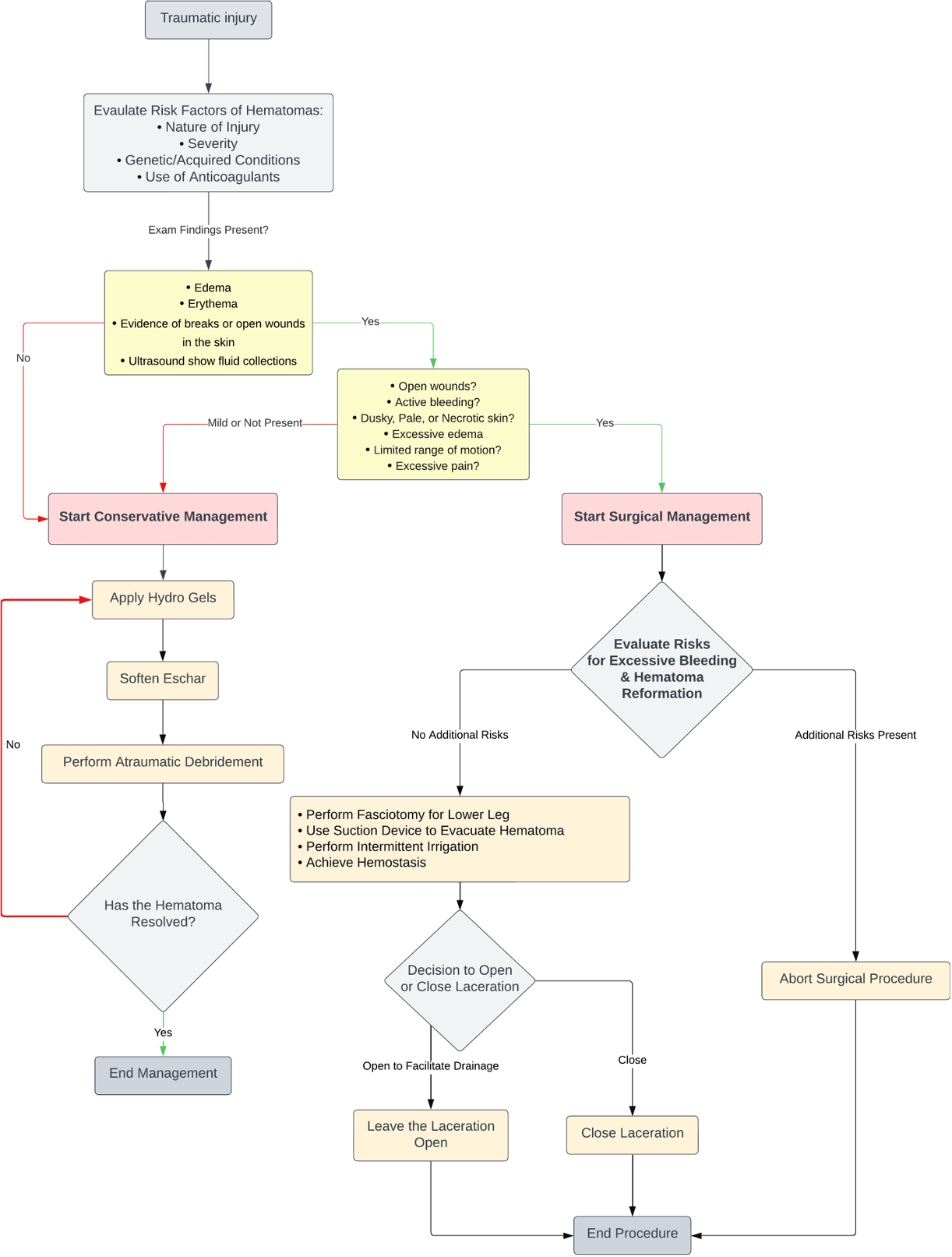
Figure 4. Algorithm for assessing, evaluating, and clinical decision-making for lower extremity hematomas.

Figure 5. Granulation tissue is present on the left lower extremity wound, with surrounding induration and tautness. Eschar and necrotic debris have been drained and removed.

Figure 6. The left lower extremity wound is granulated, with surrounding tissue taut, indurated, and erythematous, which has decreased since the previous exam.
Acknowledgments
Authors: Lundrim Marku, BS, MSc1; Hakam Rajjoub, BS1; Mihail Climov, MD2; Halil Safak Uygur, MD2
Affiliations: 1West Virginia University School of Medicine, Morgantown, West Virginia; 2West Virginia University Department of Surgery, Division of Plastic, Reconstructive, and Hand Surgery, Morgantown, West Virginia
Correspondence: Lundrim Marku, BS, MSc; lsmarku@mix.wvu.edu
Disclosures: The authors have nothing to disclose. No funding was received for this article. None of the authors has a financial interest in any of the products, devices, or drugs mentioned in this manuscript.
References
1. Ng C, Motto DG, Di Paola J. Diagnostic approach to von Willebrand disease. Blood. Mar 26 2015;125(13):2029-2037. doi:10.1182/blood-2014-08-528398
2. Du P, Bergamasco A, Moride Y, Truong Berthoz F, Ozen G, Tzivelekis S. Von Willebrand disease epidemiology, burden of illness and management: a systematic review. J Blood Med. 2023;14:189-208. doi:10.2147/JBM.S389241
3. Salmeron-Gonzalez E, Garcia-Vilarino E, Perez-Garcia A. Therapeutic management of traumatic tension hematoma with potential skin necrosis: a retrospective review of 180 patients. Eur J Trauma Emerg Surg. Apr 2022;48(2):1363-1367. doi:10.1007/s00068-021-01687-z
4. Hazendonk H, Heijdra JM, de Jager NCB, et al. Analysis of current perioperative management with Haemate(®) P/Humate P(®) in von Willebrand disease: identifying the need for personalized treatment. Haemophilia. May 2018;24(3):460-470. doi:10.1111/hae.13451
5. Livesey K, Yealy DM, Li J, Moore CG, Ragni MV. Von Willebrand disease in the emergency department. Haemophilia. Mar 2016;22(2):263-267. doi:10.1111/hae.12841
6. Reinke C, Spodeck A, Schildhauer TA, Swol J. Haemophilia A in a major trauma patient. BMJ Case Rep. Dec 16 2015;2015: bcr2015211694. doi:10.1136/bcr-2015-211694
7. Sakamoto A, Okamoto T, Matsuda S. Chronic expanding hematoma in the extremities: a clinical problem of adhesion to the surrounding tissues. Biomed Res Int. 2017;2017:4634350. doi:10.1155/2017/4634350
8. Seppala T, Grunthal V, Koljonen V. Pretibial hematomas - a real-world single-center study. JPRAS Open. Jun 2022;32:79-87. doi:10.1016/j.jpra.2022.01.001
9. Singleton T, Kruse-Jarres R, Leissinger C. Emergency department care for patients with hemophilia and von Willebrand disease. J Emerg Med. Aug 2010;39(2):158-165. doi:10.1016/j.jemermed.2007.12.024
10. Emergency Care for Patients with von Willebrand Disease. Canadian Hemophilia Society. Published 2019. Accessed March 11, 2025. https://www.hemophilia.ca/wp-content/uploads/2019/10/Emergency-Care-for-Patients-with-von-Willebrand-Disease-2019.pdf
11. Ubbink D, Brölmann FE, Go P, Vermeulen H. Evidence-Based Care of Acute Wounds: A Perspective. Adv Wound Care (New Rochelle). 2015;4(5):286-294. doi:10.1089/wound.2014.0592