Granulicatella adiacens Producing an Interesting Etiology of Delayed Breast Cellulitis
© 2025 HMP Global. All Rights Reserved.
Any views and opinions expressed are those of the author(s) and/or participants and do not necessarily reflect the views, policy, or position of ePlasty or HMP Global, their employees, and affiliates.
Questions
- What is delayed breast cellulitis, what are its common symptoms and findings, and how can we differentiate it?
- Describe the pathogenesis of delayed breast cellulitis, the risk factors, and the most common causes.
- Describe the uniqueness of the Granulicatella adiacens breast implant infection and why this may pose a challenge in treating cellulitis status post-mastectomy.
- What kind of treatment is needed for delayed breast cellulitis, and how does Granulicatella adiacens alter management?
Case Description
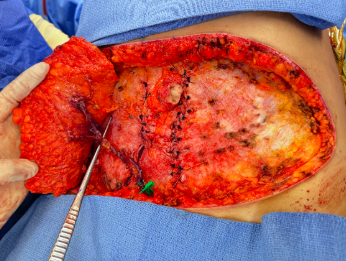
A 44-year-old woman with right skin-sparing mastectomy and axillary lymph node dissection with immediate reconstruction with tissue expander implant placement presented with 2 weeks of increasing erythema along the medial and lateral portions of the incision and a burning sensation (Figure 1). Upon inspection of the surgical site, an area of dehiscence of the lateral portion of the incision was noted with no drainage. The patient had a C-reactive protein (CRP) of 23, no leukocytosis, and an unremarkable ultrasound. The patient was admitted and started on intravenous cefepime and vancomycin.
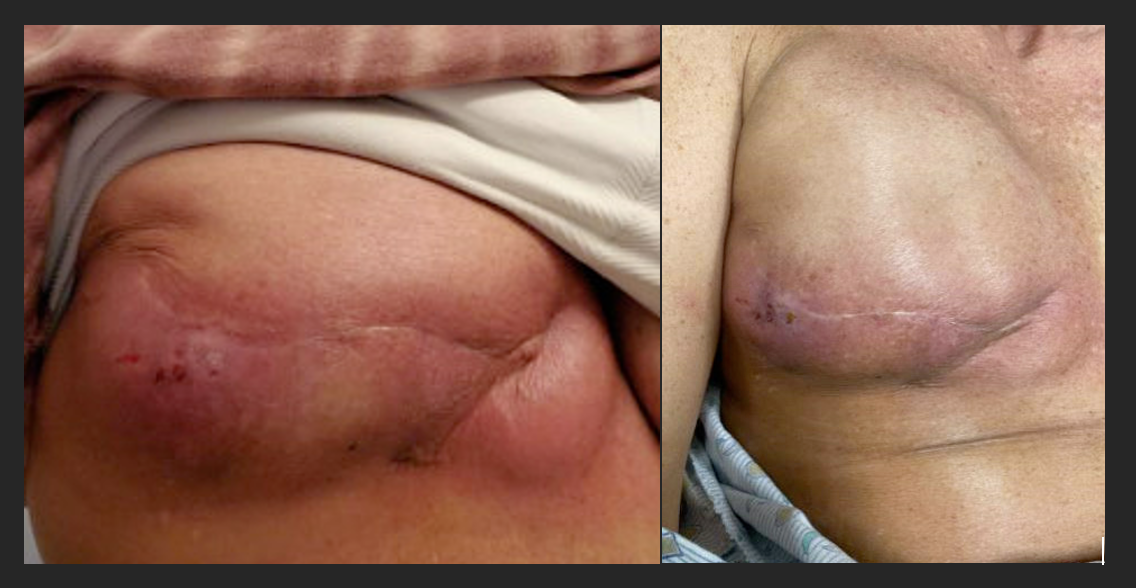
Figure 1. Depicts the clinical appearance of cellulitis, characterized by slight redness along the incision line on the right breast, with tenderness upon palpation. The breast feels uniformly firm. The skin displays warmth and pink coloration and demonstrates normal capillary refill. Furthermore, the incision site shows satisfactory healing progress.
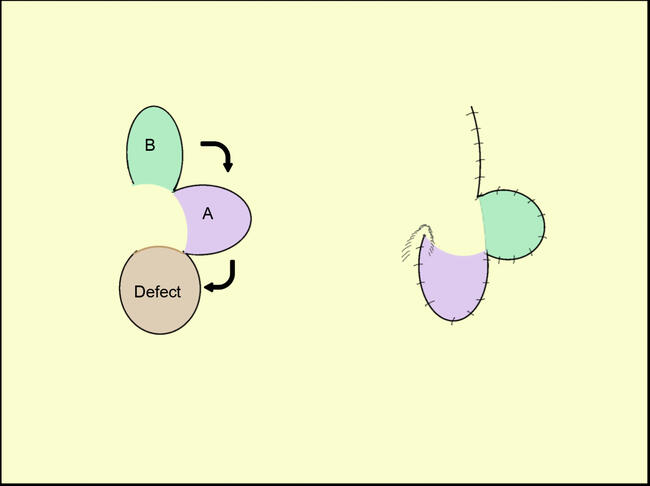
Over the next 2 days, the patient's CRP began downtrending, but erythema and pain persisted. The patient was taken to the operating room for tissue expander removal, washout, and drain placement. Specimens taken during the operation showed necrotic tissue with acute-on-chronic inflammation, fibrous tissue with foreign body giant cell reaction, and Staphylococcal species. Cultures obtained from the drain later identified a rare bacterium, Granulicatella (G.) adiacens, using the MALDI-TOF (Matrix-Assisted Laser Desorption/Ionization Time-of-Flight) mass spectrometer for bacterial identification, with sensitivity testing performed using the VITEK system (bioMérieux). Sensitivity testing confirmed that the initial antibiotic regimen was not optimally matched to G. adiacens, necessitating the adjustment to ciprofloxacin and cephalexin.
On postoperative day 1, the patient's pain improved; on day 2, the patient was deemed stable for discharge with ciprofloxacin and cephalexin. The drain remained and was removed the following week. However, the burning pain returned, and the incision remained erythematous with serous drainage (Figure 2). The patient was managed with daily wet-to-dry dressing changes, and the wound was allowed to heal by secondary intention. At her 4-week follow-up, the patient demonstrated normal wound healing, and the infection had completely resolved.

Figure 2. Images captured 3 weeks post-tissue expander removal and washout. Sutures remain intact, with minimal clear drainage observed at the lateral aspect of the incision. Upon physical examination, the skin exhibited whitening, alongside redness and swelling surrounding the incision site.
Q1. What is delayed breast cellulitis, what are its common symptoms and findings, and how can we differentiate it?
Delayed breast cellulitis (DBC) can occur after breast-conserving procedures such as breast reconstruction and is characterized by diffuse erythema, edema, tenderness, and warmth in the breast.1 Despite its significance, DBC remains underreported, with an incidence of 3% to 5%.1,2 Clinically distinguishing DBC from postoperative infections, recurrent carcinoma, and radiotherapy-induced changes poses challenges because of nonspecific symptoms. DBC is thought to occur after 3 months of breast-conserving surgery and more than 3 weeks following completion of radiotherapy.1-3 Prior studies indicate a median onset of 10 months post-surgery, with symptoms typically resolving within 7 months.1
Diagnosing DBC can be challenging because of the absence of systemic symptoms, unremarkable laboratory tests, and vague patient complaints relating to malaise, mild erythema, and subjective fevers.1,2,4 Objectively, clinical findings may include a low-grade fever, leukocytosis, mildly elevated CRP, and negative blood cultures.1 Thus, a comprehensive breast examination is vital to assess the extent of erythema, swelling, and axillary lymph node involvement.
Key features differentiate acute breast cellulitis and DBC (Figure 3). Acute infections typically arise within 3 months of breast implantation, presenting with severe pain, fever, and pronounced redness of the breast, especially associated with breast implants.4-6 DBC is characterized by infections occurring beyond 3 months post-implantation. These are far less common and often arise from bacterial seeding due to bacteremia or invasive procedures.1,2 As a result, symptoms of DBC may be less severe, making diagnosis more challenging. Radiographic imaging, such as ultrasound, can help identify fluid collections, abscesses, or malignancies associated with both conditions.1
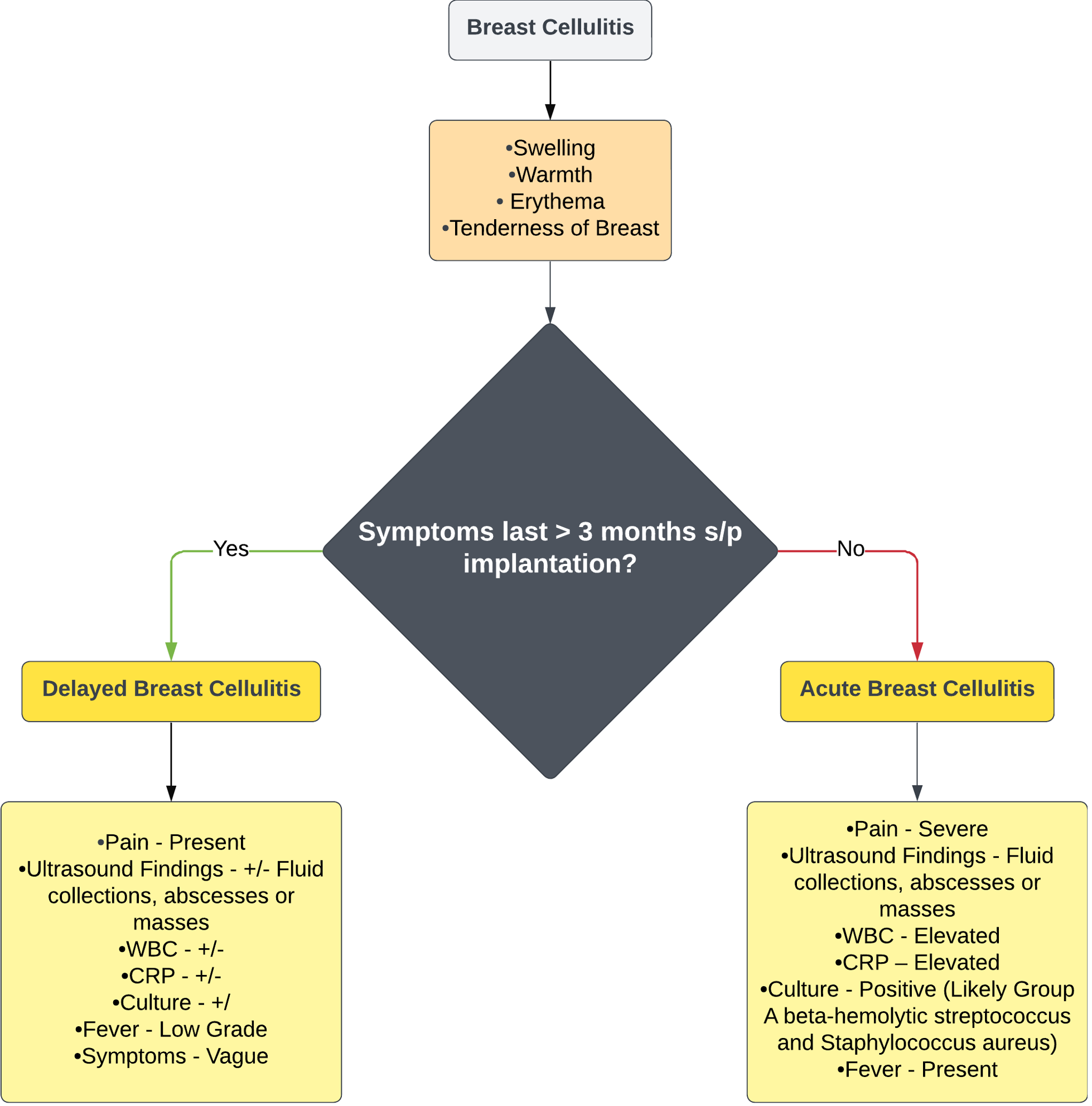
Figure 3. This algorithm aims to aid clinicians in distinguishing between acute and delayed breast cellulitis by considering the duration of symptoms, associated laboratory values, and clinical examination findings. CRP = C-reactive protein; WBC = white blood cell count.
Q2. Describe the pathogenesis of DBC, the risk factors, and the most common causes.
The literature reports that DBC represents an aseptic inflammatory process resulting from bacterial involvement.1,2,4 The current understanding is that fibrosis-induced obstruction in the subcutaneous and subdermal layers impedes lymphatic drainage. This obstruction results in fluid accumulation, bacterial proliferation, biofilm formation, and subsequent infection.1 Once established, this infection exacerbates lymphedema, causing heightened capillary permeability and compromised lymphatic drainage, perpetuating a cycle of recurrent scarring and infection (Figure 4).
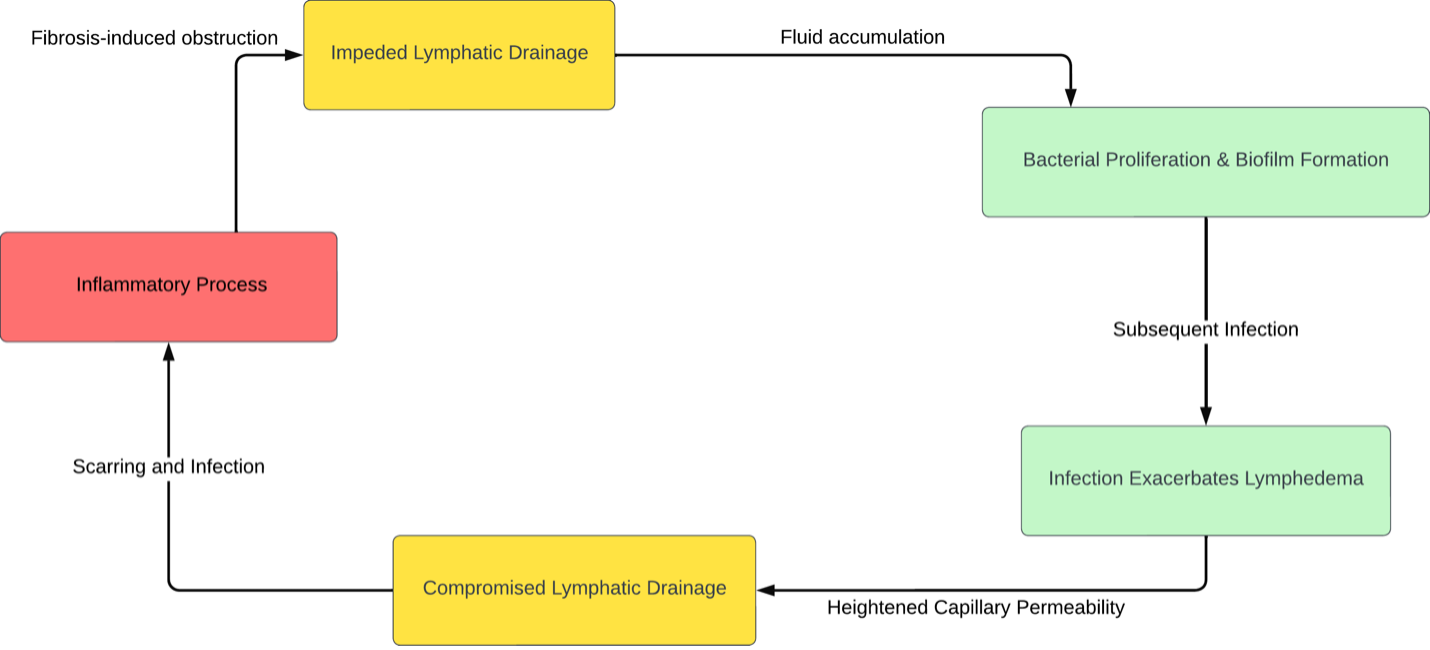
Figure 4. The proposed mechanism underlying delayed breast cellulitis based on current literature.
Radiotherapy plays a role in DBC by triggering desquamation and promoting bacterial colonization, metaplastic change of the duct epithelium, and the development of obstructive epithelioid structures within mammary ducts.1 Additionally, it initiates periductal inflammation and encourages bacterial overgrowth. Other contributing risk factors include axillary dissection involving more than 5 lymph nodes, connective tissue disorders, obesity, larger breast size, and tumor localization in the upper outer quadrant or the breast tail.1,2,4
When infections occur, the primary agents responsible for delayed breast cellulitis typically include skin flora, such as Group A beta-hemolytic Streptococcus and Staphylococcus aureus.1 The prevalence of this condition tends to be greater in instances of venous or lymphatic compromise.
Q3. Describe the uniqueness of G. adiacens breast implant infection and why this may pose a challenge in treating cellulitis status post-mastectomy.
Identifying G. adiacens,7,8 a nutritionally variant Streptococcus species, poses a formidable challenge because of its fastidious growth requirements. This bacterium predominantly inhabits the oral, urogenital, and gastrointestinal tracts and is implicated in diverse infections, spanning bacteremia, endocarditis, and orbital and nasolacrimal duct infections.7-10 It has been associated with some implant-related infections. It frequently evades detection within polymicrobial infections, leading to suboptimal treatment outcomes.7,10,11
Infections attributed to G. adiacens present a therapeutic dilemma, particularly in cases involving cardiac electronic implantable devices and prosthetic joint infections.9,10 Successful management typically necessitates rigorous irrigation, debridement, and an 8-week course of antimicrobial therapy.9 Notably, instances have arisen where G. adiacens was identified only post-treatment of prior prosthetic infections caused by Staphylococci, necessitating prolonged antibiotic courses and even prosthesis exchange or removal.9 Hence, primary staphylococcal infections refractory to initial antibiotic therapy warrant scrutiny for G. adiacens, especially if the condition exacerbates. Effective identification and treatment of G. adiacens are pivotal in averting complications and ensuring favorable treatment outcomes in individuals with implants.
While G. adiacens primarily features in infections across various body sites, literature about its role in breast infections remains scarce. Breast infections typically attributed to Staphylococcus aureus or Streptococcus species have limited documentation of G. adiacens involvement. However, considering its propensity to provoke infections in diverse anatomical regions and its inclination to be masked by polymicrobial infections, the potential involvement of G. adiacens in certain breast infections, particularly in immunocompromised cohorts or those with underlying medical conditions, warrants exploration. Detailed investigations and case reports elucidating the role of G. adiacens as a causative agent in breast infections would offer invaluable insights into its clinical significance in this context.
Q4. What kind of treatment is needed for DBC, and how does G. adiacens alter management?
The treatment approach for DBC varies depending on the severity of the infection, the duration of symptoms, and whether surface tissue or implant capsule is involved (Figure 5).1-4 Ultrasound can be used to identify fluid collections. Monitoring inflammatory markers such as white blood cell count, CRP, and sedimentation rate can give more insight into the clinical picture.
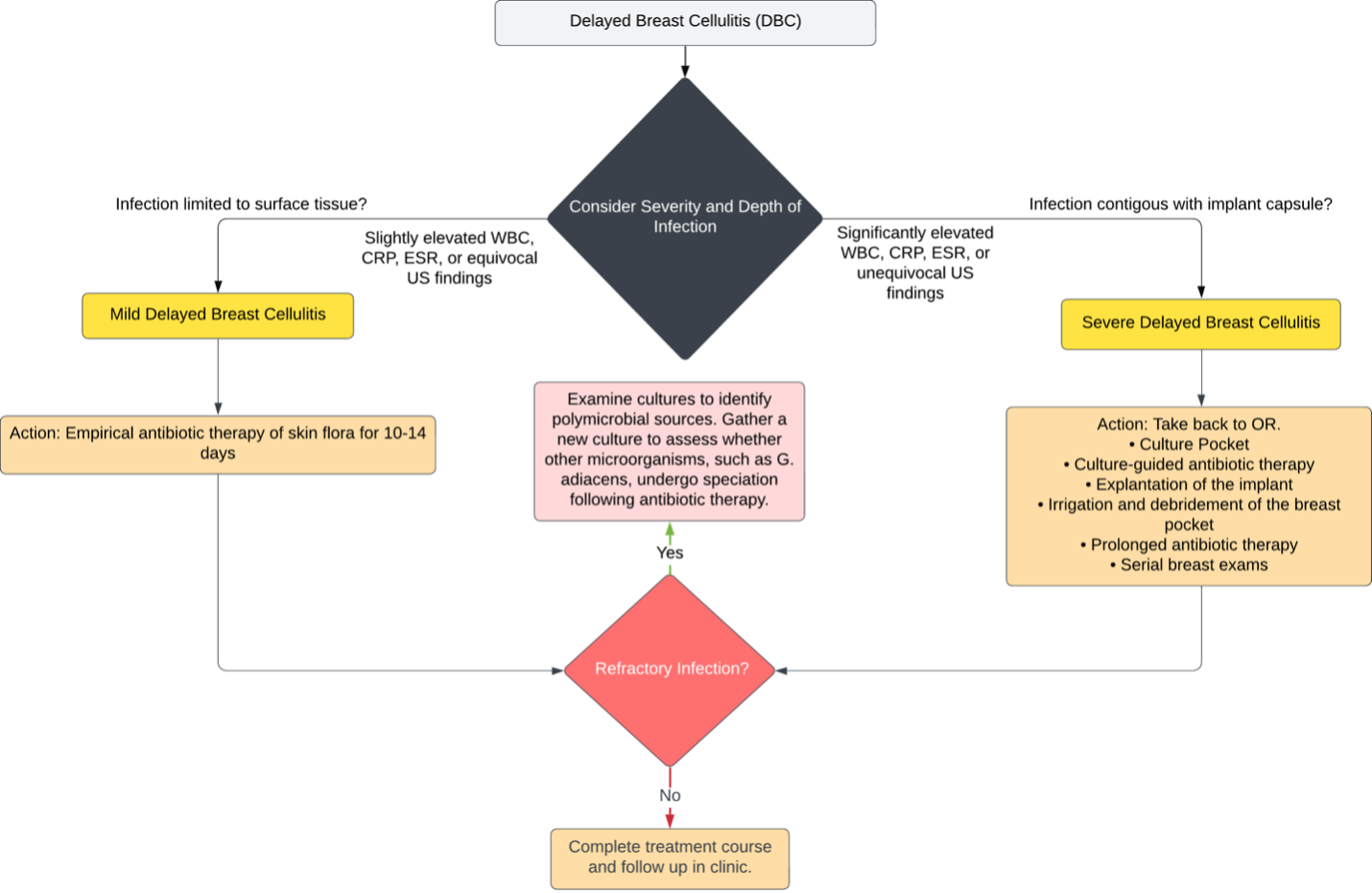
Figure 5. This algorithm delineates the treatment strategy for delayed breast cellulitis (DBC), taking into consideration factors such as white blood cell count (WBC), C-reactive protein (CRP), erythrocyte sedimentation rate (ESR), ultrasound (US) findings, depth of tissue involvement, and response to therapy.
For infections limited to surface tissue, empirical antibiotic therapy for 10 to 14 days is typically prescribed.1,3,4 Antibiotic choice is guided by local skin flora. However, if treatment is refractory, the threshold for returning the patient to the operating room to obtain an appropriate culture should be low. Performing invasive procedures like aspiration or biopsy should be avoided initially to prevent increased infection risk and implant damage.
A more aggressive approach may be necessary in severe cases involving the implant capsule. Prompt medical attention is crucial upon observing signs of delayed breast cellulitis, including redness, warmth, swelling around the implant, or deep pain.1-4 Treatment involves culturing the pocket, explantation of the implant, irrigation and debridement of the breast pocket, prolonged culture-guided antibiotic therapy, and serial breast exams. In refractory infections, polymicrobial causes, such as the speciation of G. adiacens, should be considered.
Summary
Cases of G. adiacens infection are exceedingly rare with breast implants. Only a few cases have reported microbial cultures of G. adiacens after tissue expander placement. Treating such infections presents challenges as isolating the organism takes time, and they are often mistaken for polymicrobial infections. Studies involving other prosthetics suggest that managing G. adiacens may necessitate debridement, irrigation, and a prolonged course of antimicrobials. Identifying G. adiacens as a secondary infection after group A beta-hemolytic Streptococcus or Staphylococcus aureus infection is crucial, and polymicrobial infections should not be dismissed. Effective management of these infections can prevent further complications associated with breast cellulitis.
Acknowledgments
Authors: Rebecca Norcini, MD1; Lundrim Marku, MD2; Hakam Rajjoub, BS2; Kerri Woodberry, MD1
Affiliations: 1West Virginia University Department of Surgery, Division of Plastic, Reconstructive, and Hand Surgery, Morgantown, West Virginia; 2West Virginia University School of Medicine, Morgantown, West Virginia
Correspondence: Rebecca Norcini, MD, West Virginia University Department of Surgery, Division of Plastic, Reconstructive, and Hand Surgery, 64 Medical Center Drive, Morgantown, WV 26506, USA. E-mail: Rebecca.norcini@gmail.com
Ethics: Consent was obtained from the patient for de-identified presentation of personal medical information. The authors are thankful for her willingness to let the medical community learn from her case.
Disclosures: The authors disclose no financial or other conflicts of interest.
References
1. Exarchos G, Metaxa L, Constantinidou A, Kontos M. Delayed breast cellulitis following surgery for breast cancer: a literature review. Breast Care (Basel). 2019;14(1):48-52. doi:10.1159/000494691
2. Indelicato DJ, Grobmyer SR, Newlin H, et al. Delayed breast cellulitis: an evolving complication of breast conservation. Int J Radiat Oncol Biol Phys. 2006;66(5):1339-1346. doi:10.1016/j.ijrobp.2006.07.1388
3. Miller SR, Mondry T, Reed JS, Findley A, Johnstone PA. Delayed cellulitis associated with conservative therapy for breast cancer. J Surg Oncol. 1998;67(4):242-245. doi:10.1002/(sici)1096-9098(199804)67:4<242::aid-jso6>3.0.co;2-8
4. Zippel D, Siegelmann-Danieli N, Ayalon S, Kaufman B, Pfeffer R, Zvi Papa M. Delayed breast cellulitis following breast conserving operation. Eur J Surg Oncol. 2003;29(4):327-330. doi:10.1053/ejso.2002.1377
5. Froman J, Landercasper J, Ellis R, De Maiffe B, Theede L. Red breast as a presenting complaint at a breast center: an institutional review. Surgery. 2011;149(6):813-819. doi:10.1016/j.surg.2010.12.013
6. Viola GM, Selber JC, Crosby M, et al. Salvaging the infected breast tissue expander: a standardized multidisciplinary approach. Plast Reconstr Surg Glob Open. 2016;4(6):e732. doi:10.1097/GOX.0000000000000676
7. del Pozo JL, Garcia-Quetglas E, Hernaez S, et al. Granulicatella adiacens breast implant-associated infection. Diagn Microbiol Infect Dis. 2008;61(1):58-60. doi:10.1016/j.diagmicrobio.2007.12.009
8. Gupta S, Garg M, Misra S, Singhal S. Granulicatella adiacens abscess: two rare cases and review. J Lab Physicians. 2018;10(1):121-123. doi:10.4103/JLP.JLP_58_17
9. Quénard F, Seng P, Lagier JC, Fenollar F, Stein A. Prosthetic joint infection caused by Granulicatella adiacens: a case series and review of literature. BMC Musculoskelet Disord. 2017;18(1):276. doi:10.1186/s12891-017-1630-1
10. Sendi P, Wustmann K, Büchi AE, et al. Cardiac implantable electronic device-related infection due to Granulicatella adiacens. Open Forum Infect Dis. 2019;6(4):ofz130. doi:10.1093/ofid/ofz130
11. Quénard F, Seng P, Lagier JC, Fenollar F, Stein A. Prosthetic joint infection caused by Granulicatella adiacens: a case series and review of literature. BMC Musculoskelet Disord. 2017;18(1):276. doi:10.1186/s12891-017-1630-1