Buccal Sulcus Approach to Septal Perforation Repair
© 2025 HMP Global. All Rights Reserved.
Any views and opinions expressed are those of the author(s) and/or participants and do not necessarily reflect the views, policy, or position of ePlasty or HMP Global, their employees, and affiliates.
Abstract
The treatment of septal perforations is a challenging endeavor. The recurrence rate ranges from 30% to 70%. Operative correction often requires wide dissection, local flaps, and septal spacers. The pediatric population poses an even greater challenge given the limited size for visualization and less tissue available to transfer. The most common and successful methods involve endoscopic and open rhinoplasty techniques. The authors present a midfacial degloving approach via a transoral, gingivobuccal approach that does not require an endonasal component or external incisions.
Introduction
The treatment of septal perforations is a challenging endeavor. High relapse rates exist, with the incidence of perforation recurrence ranging from 30% to 70%.1 Operative correction often requires wide dissection, recruitment of surrounding tissues, and placement of a septal spacer in order to avoid opposing suture lines. The pediatric population poses an even greater challenge given the limited visualization, access, and the amount of adjacent tissue available to transfer.2 The most common and successful techniques reported involve endoscopic-assisted tissue transfer and an open rhinoplasty technique.2,3
Here, we describe a modification of the sublabial, midfacial degloving approach that is similar to a previously reported approach by Karlan et al.4 Unlike the former description that utilized bilateral intercartilaginous and complete transfixion incisions to augment a gingivobuccal sulcus incision, our approach does not require the addition of an endonasal component.
Case Presentations
A.B. is a 7-year-old male who presented with a septal perforation after battery lodgment in his nostril. The patient had recurrent epistaxis, nasal drainage, irritation, and whistling with speaking. He had previously undergone approximately 20 procedures at different institutions including debridements, stent placements, and multiple surgical attempts at closure. The physical exam revealed a persistent 15-mm perforation approximately 1-cm posterior to the caudal septum (Figure 1). After utilizing the mucoperichondrial and mucoperiosteal flaps from the maxillary buccal suclcus incision, the patient had 49 months of follow-up with no recurrence.

Figure 1. Intraoperative nasal speculum exam demonstrating chronic anterior nasal septal perforation.
J.D. is a 23-year-old female who presented with a septal perforation after she collided with a large dog, which caused a septal hematoma that went unrecognized. The patient had recurrent congestion, epistaxis, dryness, and drainage. The physical exam revealed a 15-mm perforation approximately 1-cm posterior to the caudal septum
Surgical technique
Following endotracheal intubation and appropriate sterile preparation of the nose and face, an upper gingivobuccal sulcus incision was carried down to the maxillary periosteum (Figure 2). A subperiosteal dissection was then performed to the level of the piriform rim and anterior nasal spine, elevating the lateral vestibular mucosa and nasal floor in continuity as a wide-based mucoperiosteal flap. Dissection was carried out at this depth, medially raising the mucoperichondrium off the caudal septum and the mucoperiosteum off the vomer up to level of the septal perforation. An incision was then made around the circumference of the perforation, followed by separation of the mucoperichondrium bilaterally covering the cartilaginous septum (Figure 3). By en bloc elevation, the mucoperichondrium from the lateral vestibule/piriform and nasal floor were advanced medially, effectively closing the perforation in a straight, tension-free bilateral closure from posterior to anterior (Figure 4). An interposition graft of human acellular dermal matrix (AlloDerm, LifeCell Corp) was then inset, and the caudal septum was affixed to the maxillary spine to prevent displacement. Lastly, the gingivobuccal sulcus incision was closed, and silicone nasal splints were placed using transeptal suture fixation.
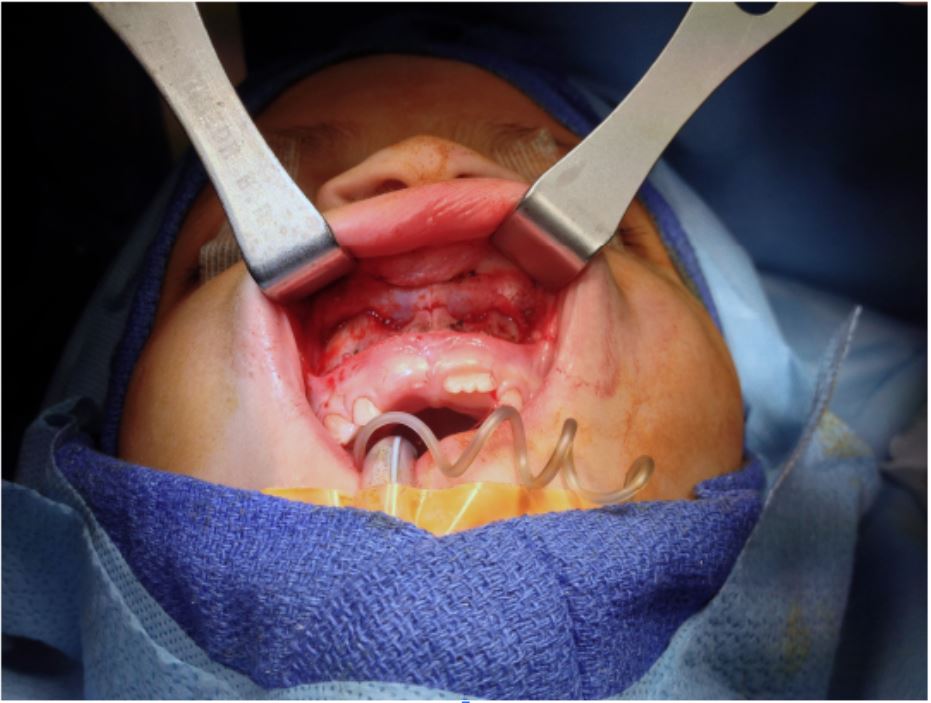
Figure 2. Upper buccal sulcus incision allows exposure to the anterior nasal septal perforation and local tissue advancement and closure.
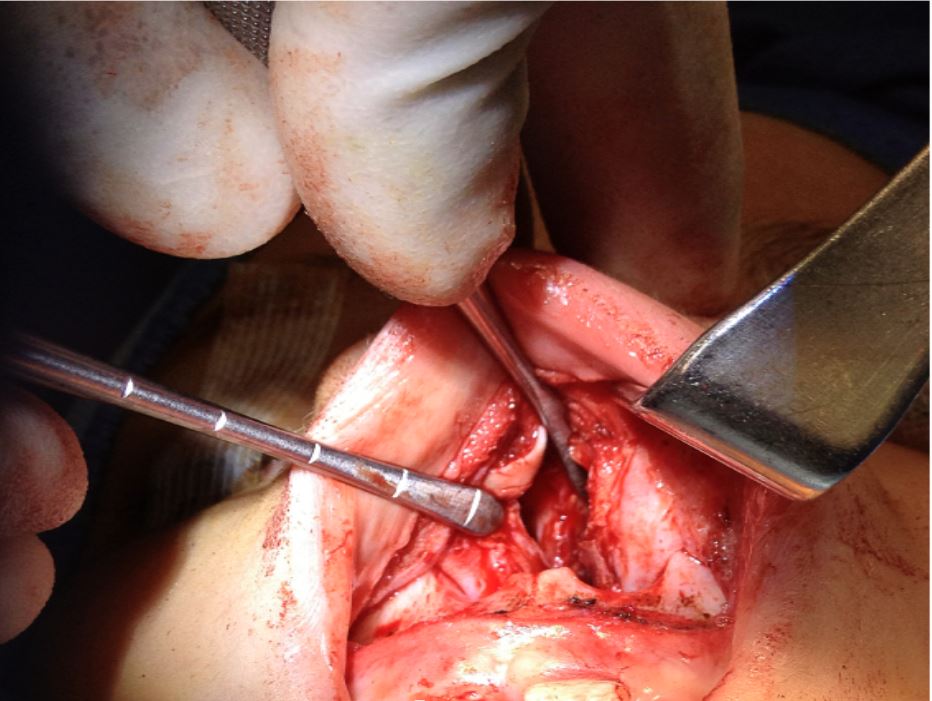
Figure 3. Bilateral mucoperichondrial dissection exposing cartilaginous perforation.
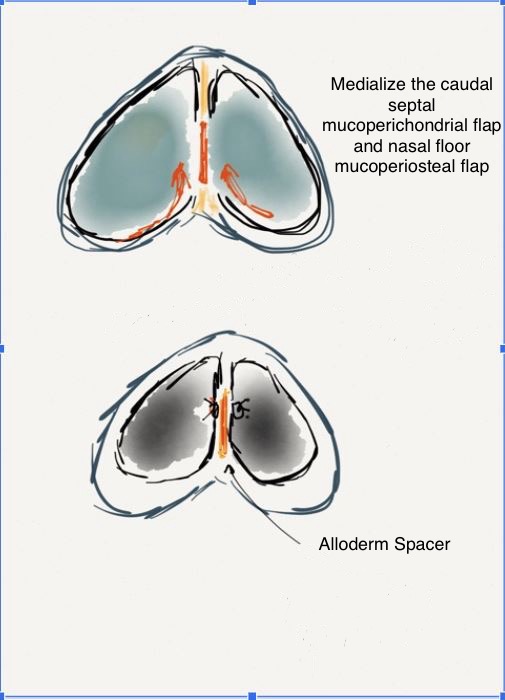
Figure 4. Illustration depicting medial advancement of the nasal mucosa to achieve perforation closure over an interposition graft of acellular dermal matrix.
Discussion
The prevalence of nasal septal perforations has been reported to be as high as 0.9%,1 of which roughly 62% are symptomatic,5 although the incidence in the pediatric population is not well documented. Iatrogenic causes include septal surgery (the most common etiology and up to 25% following submucous resection6), nasal cauterization and/or packing for epistaxis, nasogastric tube placement, prolonged nasal intubation, or cryosurgery. Traumatic nasal bone/septal fractures, untreated septal hematomas, the presence of nasal foreign bodies or rhinoliths, and nose picking have resulted in nasal septal perforations. Substance abuse (eg, cocaine, methamphetamine), infection (eg, syphilis, tuberculosis, varicella zoster), and neoplastic (eg, T-cell lymphoma, carcinomas, cryoglobunemias) and inflammatory (eg, Wegener’s granulomatosis, systemic lupus erythematosus, midline lethal granuloma, Crohn’s disease, polyarteritis nodosa, pyoderma granulosum, dermatomyositis, rheumatoid arthritis) pathologies have all been associated with perforations of the nasal septum. Again, not all nasal septal perforations are symptomatic, as asymptomatic lesions tend to be located posteriorly, with well-healed edges rarely requiring treatment. However, the more anterior the perforation, the more likely it is that the patient will seek evaluation and treatment. Symptoms associated with septal perforation include crusting, bleeding, whistling (smaller perforations resulting in laminar airflow disruption), nasal obstruction due to crusting or turbulence, pain, rhinorrhea, malodorous discharge, and concomitant paranasal sinusitis in individuals seeking therapy.7
There are nonsurgical methods of closure that utilize either an acrylic, silastic, or silicone obturator. Their use, however, has been associated with unfavorable long-term patient tolerance. Approximately 50% of patients with an obturator report compliance and/or satisfaction.8 Therefore, this is not considered first-line therapy, and it is restricted for those who are inappropriate surgical candidates or those who continue to use cocaine.9
There exists no single operative technique to address a septal perforation that is universal and uniformly reliable,9 and surgical failure rates have ranged from 30% to 70% in the literature.1 Successful repairs tend to use vascularized tissue, an interpositional connective tissue scaffold, and tension-free mucosal closure.2,3,9,10 Surgical approaches for access to the perforation have included endonasal, endonasal with alatomy, endoscopic, and external transcolumellar incisions.9 The closed or endoscopic approaches have limited visibility and can be difficult to perform depending on the location and the size of the defect. The more difficult and larger defects often require external “open” incisions.
Casson et al11 originally described the midface degloving technique for exposure of maxillary operations. Sachs et al12 have reported their success with reliable and durable closure of septal perforations through a graduated surgical approach based on the size and location of the defect. Anterior perforations of less than 5 mm were closed using bipedicle opposing septal mucosal flaps through an intranasal approach. For perforations 5 to 20 mm in size, and smaller perforations more posteriorly located, the authors used an extended external rhinoplasty with subsequent elevation and rotation of posterior-based, unipedicled, intranasal mucosal flaps and an acellular dermal matrix interposition graft, thereby achieving successful closure in 92.9% of cases. Finally, perforations greater than 20 mm were addressed in a staged mucosal expansion and flap medialization over an acellular dermal matrix interposition graft via a midface degloving approach, as previously described.10 Eighty-two percent of patients had complete perforation closure at 1-year postoperative. Karlan et al4 modified Sachs’ technique by utilizing the midface degloving technique and less intranasal dissection for his bipedicle flap formation. Both of these techniques leave an area of denuded bone at the level of the piriform aperture where the flap is raised.
Following the surgical principles presented by Sachs and Karlan, our technique uses vascularized tissue and acellular dermal matrix interposition grafts to achieve closure of these nasal perforations with the added benefit of no visible or external incisions. The gingivobuccal incision is useful to fully elevate the required mucoperiosteum and mucoperichondrium to allow medial mobilization without requiring the creation of a uni/bipedicle flap or areas of denuded bone from an intranasal or external incision. The buccal sulcus incision technique is routinely performed during orthognathic surgery and provides improved access and visibility. With improved access, we are able to elevate wide base flaps that have adequate vascular supply to cover the interposition graft to ensure incorporation and create tension-free closure of the perforation. This technique has shown positive results and should be added to the armamentarium of surgeons faced with this difficult issue.
Conclusions
Nasal septal perforation repair with wide-based mucoperiosteal and mucoperichondrial flaps via an intraoral, maxillary buccal sulcus incision is a safe and effective alternative for the repair of chronic, anterior nasal septal perforations in the pediatric population. This approach preserves facial aesthetics by avoiding external scarring from alatomy or open rhinoplasty incisions and eliminates the risk of facial growth disturbances.
Acknowledgments
Authors: Kenny T. Quang, MD1;
Affiliations: 1Summa Health Systems, Division of Plastic Surgery, Akron, Ohio; 2Akron Children’s Hospital, Division of Pediatric Plastic Surgery, Akron, Ohio
Correspondence: Kenny Quang, MD, 55 Arch Street, Suite 2F, Akron, OH 44304, USA. Email: kenny.quang@gmail.com
Ethics: Consent was obtained from all patients for the use of images for publication.
Disclosures: The authors disclose no relevant financial or nonfinancial interests.
References
- Beckmann N, Ponnappan A, Campana J, Ramakrishnan VR. Posterior septal resection: a simple surgical option for management of nasal septal perforation. JAMA Otolaryngol Head Neck Surg. 2014;140(2):150-154. doi:10.1001/jamaoto.2013.5996
- Chang DT, Irace AL, Kawai K, Rogers-Vizena CR, Nuss R, Adil EA. Nasal septal perforation in children: presentation, etiology, and management. Int J Pediatr Otorhinolaryngol. 2017;92:176-180. doi:10.1016/j.ijporl.2016.12.003
- Jennings JJ, Shaffer AD, Stapleton AL. Pediatric nasal septal perforation. Int J Pediatr Otorhinolaryngol. 2019;118:15-20. doi:10.1016/j.ijporl.2018.12.001
- Karlan MS, Ossoff R, Christu P. Reconstruction for large septal perforations. Arch Otolaryngol. 1982;108(7):433-436. doi:10.1001/archotol.1982.00790550037009
- Ozdek A, Bayır O, Dündar Y, Tatar EC, Saylam G, Korkmaz MH. Closure of nasal septal perforations using bilateral intranasal advancement/rotation flaps. Kulak Burun Bogaz Ihtis Derg. 2014;24(3):123-128. doi:10.5606/kbbihtisas.2014.20092
- Dommerby H, Rasmussen OR, Rosborg J. Long-term results of septoplastic operations. ORL J Otorhinolaryngol Relat Spec. 1985;47(3):151-157. doi:10.1159/000275761
- Romo T III, Sclafani AP, Falk AN, Toffel PH. A graduated approach to the repair of nasal septal perforations. Plast Reconstr Surg. 1999;103(1):66-75. doi:10.1097/00006534-199901000-00012
- Lee KC, Lee NH, Ban JH, Jin SM. Surgical treatment using an allograft dermal matrix for nasal septal perforation. Yonsei Med J. 2008;49(2):244-248. doi:10.3349/ymj.2008.49.2.244
- Kridel RW. Septal perforation repair. Otolaryngol Clin North Am. 1999;32(4):695-724. doi:10.1016/s0030-6665(05)70165-1
- Metzinger SE. Diagnosing and treating nasal septal perforations. Aesthet Surg J. 2005;25(5):524-529. doi:10.1016/j.asj.2005.06.002
- Casson PR, Bonanno PC, Converse JM. The midface degloving procedure. Plast Reconstr Surg. 1974;53(1):102-103. doi:10.1097/00006534-197401000-00026
- Romo T III, Foster CA, Korovin GS, Sachs ME. Repair of nasal septal perforation utilizing the midface degloving technique. Arch Otolaryngol Head Neck Surg. 1988;114(7):739-742. doi:10.1001/archotol.1988.01860190043019