Surgical Management of Biopolymer Induced Granulomatous Hypercalcemia and Renal Insufficiency: A Case Report and Literature Review
© 2025 HMP Global. All Rights Reserved.
Any views and opinions expressed are those of the author(s) and/or participants and do not necessarily reflect the views, policy, or position of Wounds or HMP Global, their employees, and affiliates.
Abstract
Volumetric enhancement is a key component of body contouring, with injections of natural or synthetic biopolymers being one of the most common methods used. Biopolymers, however, are associated with both acute and chronic complications including the risk of granulomatosis and hypercalcemia. Unrecognized and untreated, biopolymer-induced granulomatous hypercalcemia can lead to renal failure, metastatic calcifications, and death. Medical management is the primary treatment for biopolymer-induced granulomatous hypercalcemia, with corticosteroids and other drugs targeting calcium metabolism and immunomodulation. In cases refractory to medical management, surgical excision of biopolymer granulomatous tissue can normalize serum calcium and improve renal function. This case report of 2 patients and literature review of 4 patients investigates the rare surgical management of patients with biopolymer-induced granulomatous hypercalcemia, the morbidity of such a procedure, and adjunctive techniques that may be utilized to facilitate biopolymer removal and reduce complications.
Introduction
Volumetric enhancement is a key component of body contouring. Injections of natural or synthetic biopolymers have been one of the most common methods of volumetric enhancement both historically and today. Biopolymer filling agents include both legal soft-tissue fillers like polymethylmethacrylate spheres (Bellafill, Suneva Medical), calcium hydroxyapatite spheres (Radiesse, Merz Aesthetics), poly-L-lactic acid (Sculptra, Galderma), collagen, and hyaluronic acid, as well as products not approved by the US Food and Drug Administration including liquid silicone, mineral oil, vegetable oil, paraffin, and others. Another source of biopolymer exposure, silicone implants, can have gel bleed or rupture, with studies showing an incidence of silent rupture in up to 10.6% of silicone breast implants.1 Of particular concern is the scourge of illicit biopolymer injections with often unknown agents by unlicensed sham providers in the United States, with Florida in 2013 representing the majority of cases (10), followed by Texas (4) and California (3).2
Biopolymers are associated with both acute and chronic complications. Acute biopolymer exposure can lead to cellulitis; abscesses; atypical infections; local, regional, or systemic migration; and fatal silicone oil embolism.3-5 Chronic sequelae of biopolymer exposure include skin changes, fibrosis, foreign body granulomas, regional and remote migration, and autoimmune phenomena. Unrecognized and untreated, biopolymer granulomatosis can lead to biopolymer-induced granulomatous hypercalcemia, end-stage renal failure, metastatic calcifications, and death.6 Biopolymer granulomas are rare, with an incidence of 0.02% to 1% of exposed patients, and are associated with the total cumulative volume used (body burden), the injection method, the location injected, and the presence of any adulterants.7 Specifically, volumes over 10 mm, repeated injections, injection of large depots rather than microdroplets, injecting in the trunk or buttocks, particle surface smoothness, particle surface charge, hydrophilicity, and the presence of adulterants such as heavy metals and pesticides have all been associated with an increased complication rate and poor outcomes.8-10
Biopolymer granulomatosis is an M1-mediated macrophage response to foreign bodies correlating with host immunoreactivity and antigenic bioburden, and may occur early or decades after exposure.8 Following biopolymer injection, host protein adsorption occurs on the biopolymer particles, activating host neutrophils. Neutrophils release opsonins and soluble factors including chemokines, recruiting immune cells to the area. Macrophages attempt to phagocytize the particles and combine to form multinucleated giant cells under the influence of IL-4 and IL-13. Finally, the multinucleate giant cells signal with lymphocytes and fibroblasts, walling off the foreign body with a fibrotic capsule (Figure 1).10 Staging is determined by physical examination and imaging and is graded according to the presence of skin changes, pain, and depth of tissue plane affected (Figure 2).11 Computed tomography features include silicone cysts, granulomas, nodules with fatty infiltration, and calcifications with surrounding reactive changes. Magnetic resonance imaging features include soft tissue nodules hypointense on T1 and T2 sequences but hyperintense on silicone-sensitive sequences.12
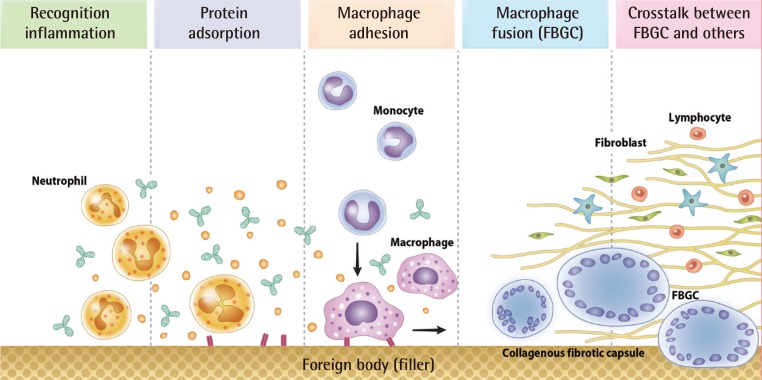
Figure 1. Phases of foreign body granuloma formation. Reprinted under Creative Commons – Noncommercial License from Lee JM, fig. 1, p. 233.10
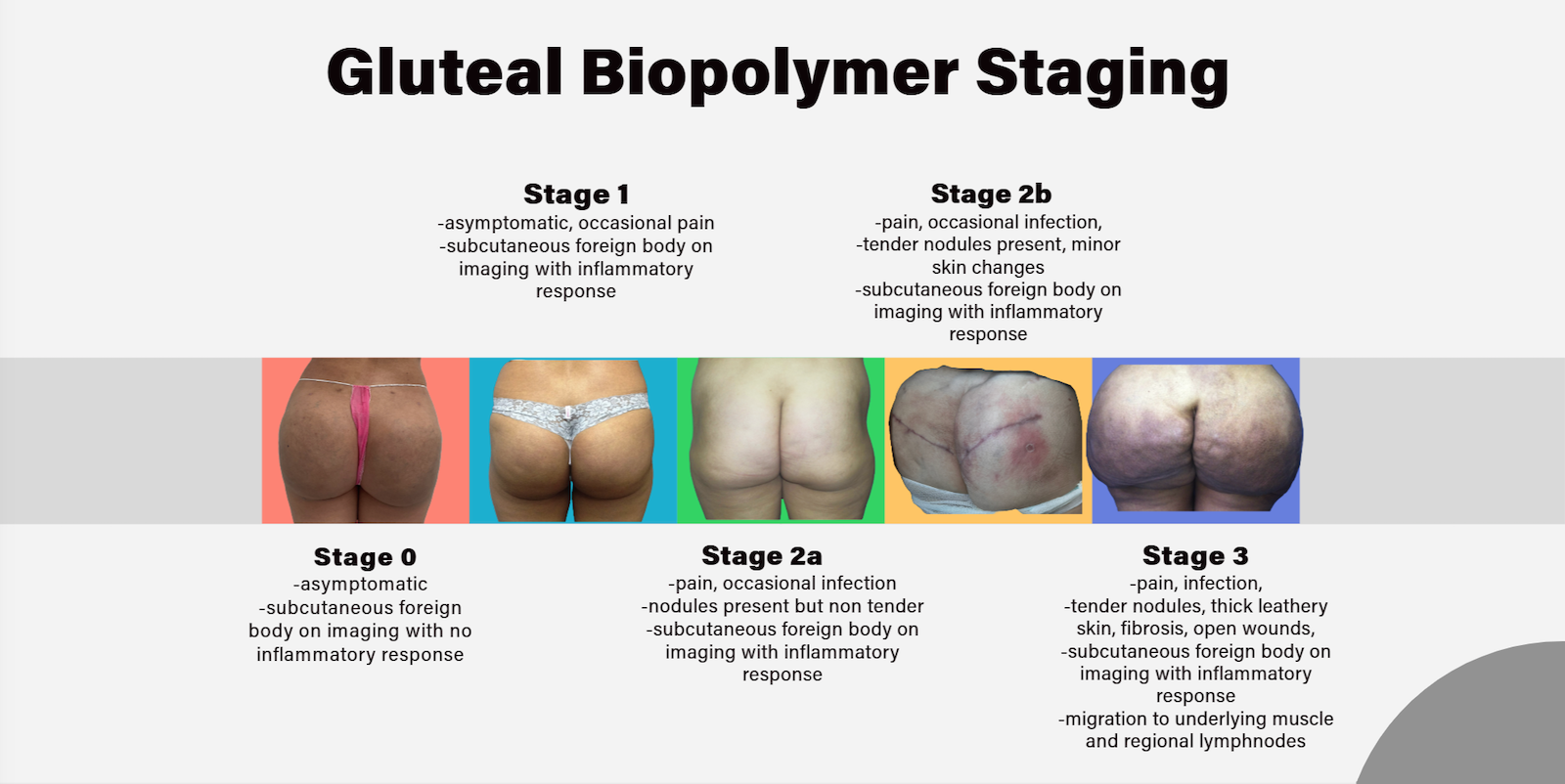
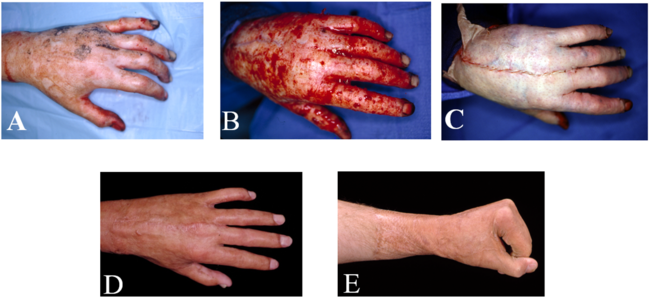
Figure 2. Gluteal biopolymer staging.
Case Presentation
The authors present 2 cases of biopolymer-induced granulomatous hypercalcemia treated with surgical management. The primary end points were preoperative and postoperative markers of biopolymer-induced granulomatous; hypercalcemia; and renal function including absolute serum calcium, creatinine, and 1,25-hydroxycholecalciferol. Additional end points included age; gender; type of biopolymer exposure and length of time since exposure; number of operative interventions; and complications such as wound dehiscence, seroma, surgical site infection, and progression to dialysis-dependent renal failure.
A systematic literature review was performed for articles related to biopolymer-induced granulomatous hypercalcemia and surgical management, with data related to outcome and complications extracted.
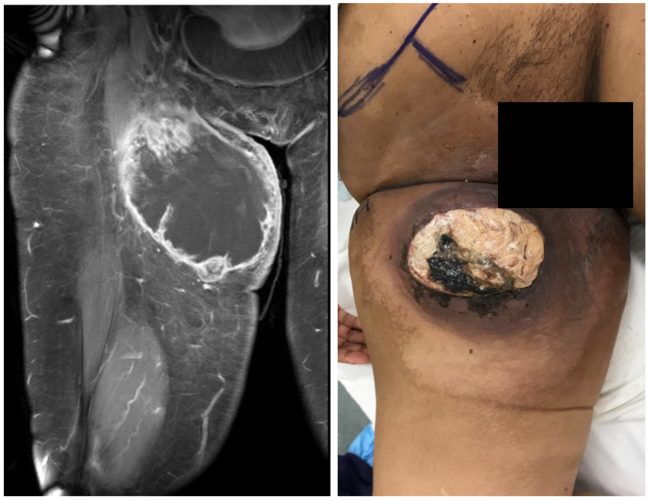
Our first case is a 53-year-old woman with a history of gluteal augmentation with intramuscular silicone implants 10 years previously. She developed nodularity, discomfort, skin changes, fatigue, and renal dysfunction 9 years following augmentation and underwent 1 year of medical management without improvement (Figure 3). Computed tomography revealed the presence of biopolymer granulomatosis within the skin, subcutaneous tissue, gluteal musculature, and the presence of regional pelvic lymphadenopathy, consistent with stage 3 biopolymer granulomatosis. Preoperatively, the patient had a serum calcium of 12.2 (reference: 8.5-10.2 mg/dL) and a serum creatinine of 1.1 (reference in women: 0.59-1.04 mg/dL), consistent with stage 2 chronic kidney disease. Preoperative 1,25-hydroxycholecalciferol was 109 pg/mL (reference in women: 18-78 pg/mL), consistent with granulomatosis. The patient underwent direct excision and serial debridement of the granulomatous tissue, including the superficial portion of the gluteus maximus, 3 times over 6 weeks. Inside the granulomatous area, individual silicone “beads” were found surrounded by a thick capsule and fibrosis (Figures 4 and 5). Structures deep to the superficial gluteus maximus were left intact because of concern for increased morbidity (Figure 6). Negative pressure wound therapy was used to temporize the wound between each debridement. Following the third debridement, reconstruction was performed with local flaps, quilting sutures, and closed suction drains; the drains were removed at 2 weeks. Reconstruction was complicated by a seroma that responded to incision and drainage with packing in the clinic. Pain at the site and hypercalcemia improved but did not fully resolve. The patient returned to the operating room at 18 and 30 months following the initial debridement for re-excision and closure. The final debridement and reconstruction were complicated by a localized dehiscence at 3 weeks postoperative that responded to incision and drainage and packing. Hypercalcemia was found to have fully resolved 3 months following her final procedure with a final serum calcium of 9.1 mg/dL (reference: 8.5-10.2 mg/dL). Renal function improved with a final creatinine of 0.68 mg/dL (reference in women: 0.59-1.04 mg/dL), consistent with a complete normalization of kidney function. Granulomatous activity was decreased, with a final postoperative serum 1,25-hydroxycholecalciferol of 78.5 pg/mL (reference in women: 18-78 pg/mL). The patient was satisfied with the final result (Figure 7).

Figure 3. Preoperative: postero-anterior and lateral views revealing granulomatous skin changes and nodularity.

Figure 4. Intraoperative: silicone granuloma ex vivo. Note the silicone bead surrounded by a fibrous capsule.
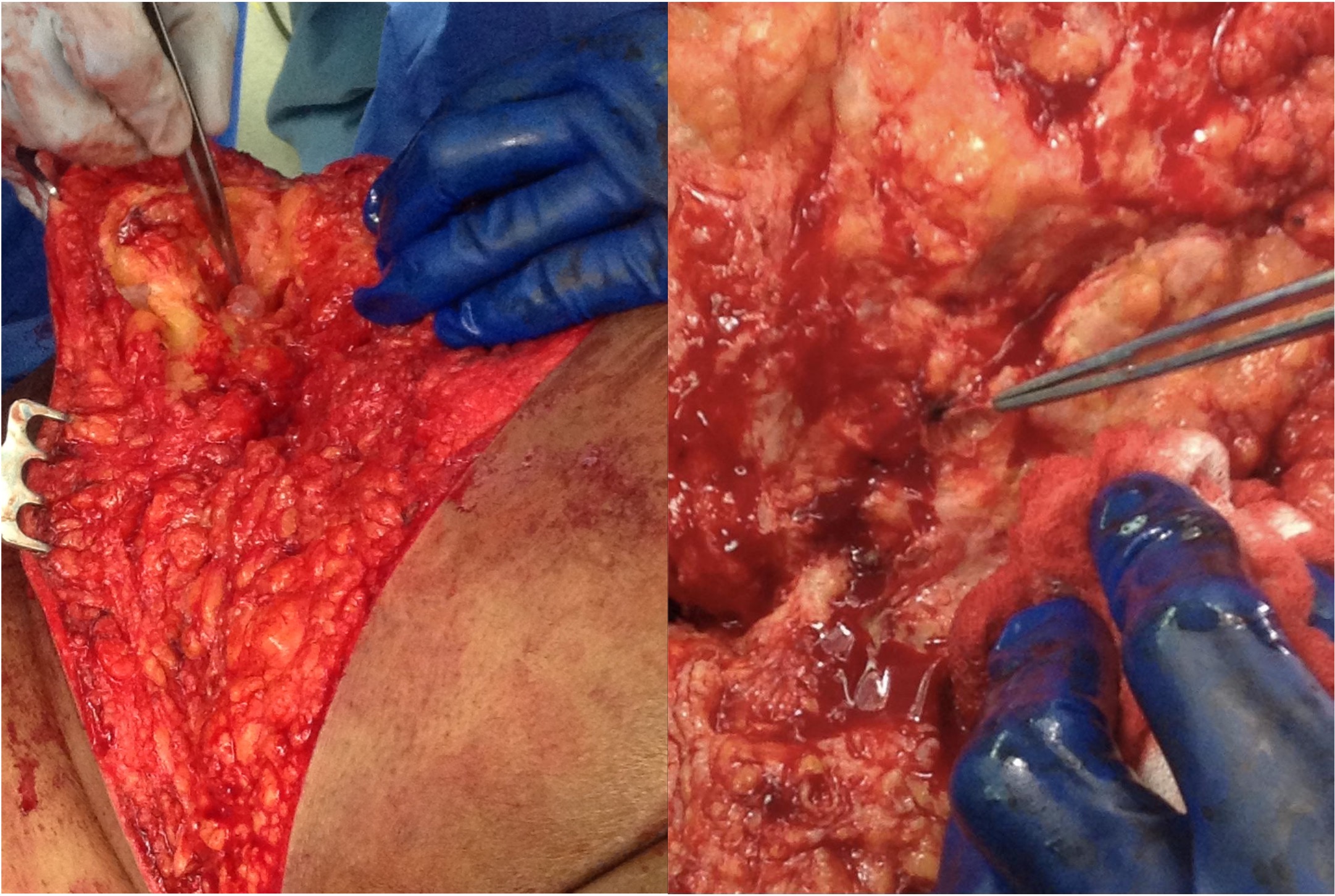
Figure 5. Intraoperative: silicone granuloma in vivo. Note the fibrotic tissue surrounding the silicone bead.
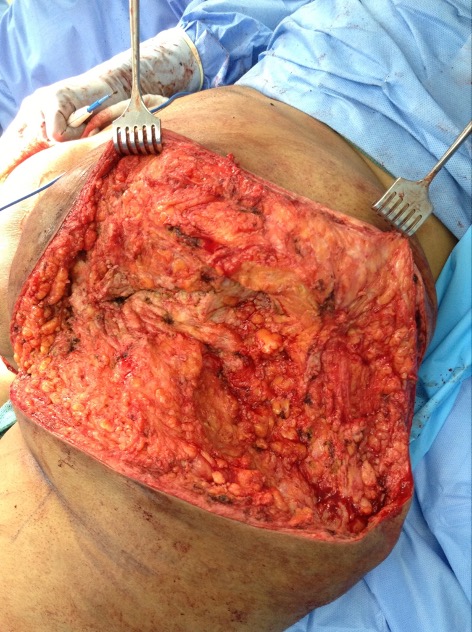
Figure 6. Intraoperative: buttock wound following debridement of granulomatous tissue.
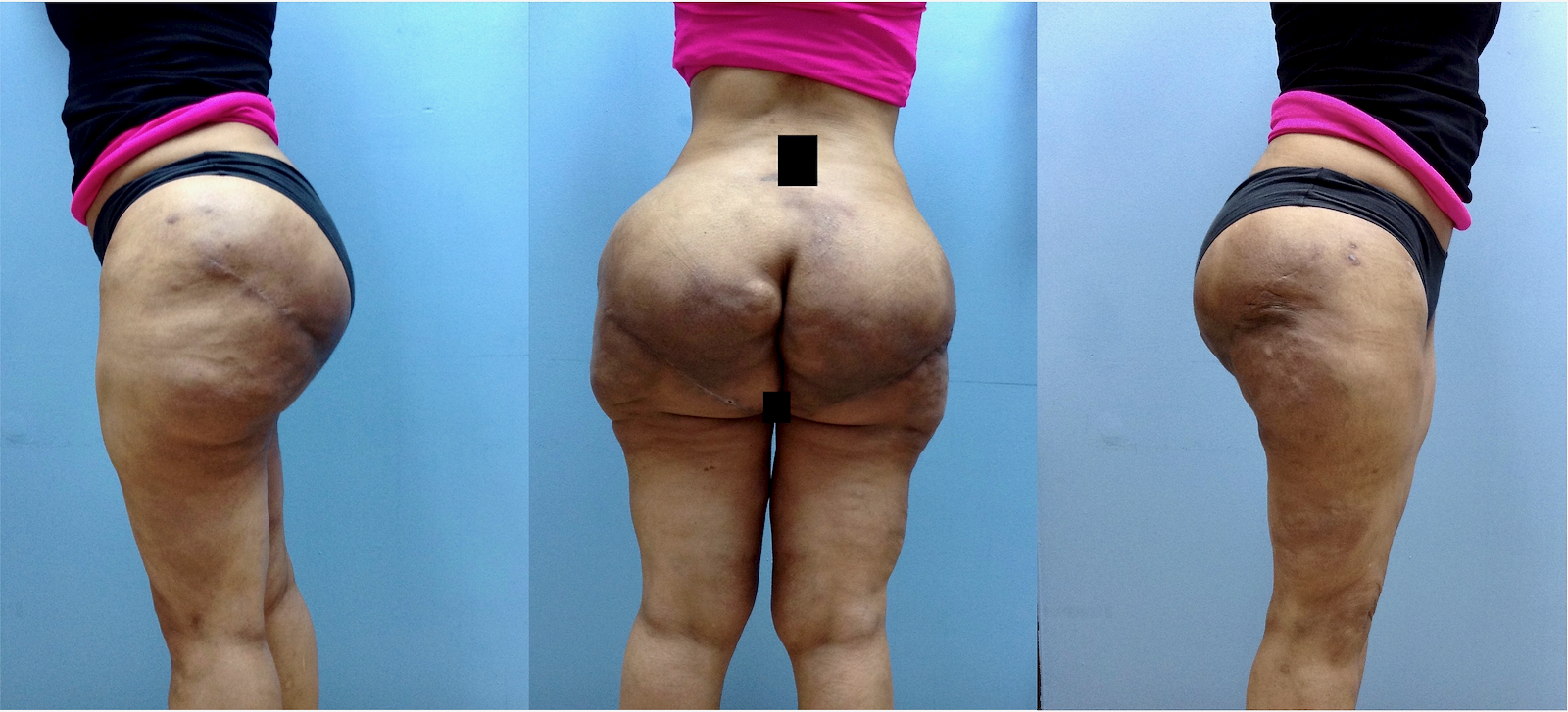
Figure 7. Postoperative: postero-anterior and lateral views of final result. Note improvement of skin changes and nodularity, but with some persistent contour irregularity.
Our second case is a 59-year-old woman with a history of biopolymer injections of unknown material to the buttocks 10 years previously. She began to develop nodularity, discomfort, skin changes, and fatigue approximately 7 years post-injection. The patient underwent 3 years of medical management without improvement and slowly worsening renal function. Computed tomography revealed the presence of biopolymer granulomatosis within the tissue planes of the skin, subcutaneous tissue, and gluteus maximus muscle, consistent with Stage 3 biopolymer granulomatosis. Preoperatively, the patient had a serum calcium of 13.6 mg/dL (reference: 8.5-10.2 mg/dL) and a serum creatinine of 4.5 mg/dL (reference in women: 0.59-1.04 mg/dL), consistent with stage 5 chronic kidney disease. Preoperative 1,25-hydroxycholecalciferol was 161 pg/mL (reference in women: 18-78 pg/mL), consistent with granulomatosis. The patient underwent direct excision and wide debridement of the granulomatous tissue, including the superficial portion of the gluteus maximus. Immediate reconstruction was performed with local flaps, hydrolyzed type 1 collagen (CellerateRX, Sanara MedTech), quilting sutures, closed suction drains, and incisional negative pressure wound therapy. The drains were removed at 2 weeks. Reconstruction was complicated by a seroma and localized wound dehiscence at 4 weeks postoperative. The patient was taken back to the operating room with revision of the closure. Hypercalcemia was found to have fully resolved 3 months following her final procedure with a serum calcium of 9.7 mg/dL (reference: 8.5-10.2 mg/dL). Renal function improved with a creatinine of 2.8 mg/dL (reference in women: 0.59-1.04 mg/dL), consistent with stage 4 chronic kidney disease. Granuloma activity was decreased, with a final postoperative serum 1,25-hydroxycholecalciferol normalized at 46 pg/mL (reference in women: 18-78 pg/mL). The patient was satisfied with the final result and has continued close follow-up with nephrology to monitor her renal function.
Systematic review of the literature for the surgical management of biopolymer-induced granulomatous hypercalcemia found 3 case reports with 4 patients that met inclusion criteria for a total of 6 patients when combined with those of the present study.12-14 In terms of primary end points, preoperative laboratory investigations revealed an average serum calcium of 13.8 mg/dL (reference: 8.5-10.2 mg/dL, study range: 11.5-17.3 mg/dL), creatinine of 1.35 mg/dL (reference in women: 0.59-1.04 mg/dL, study range: 1.1-4.5 mg/dL), and 1,25 hydroxycholecalciferol of 109 pg/mL (reference in women: 18-78 pg/mL, study range: 71-232 pg/mL). Postoperative laboratory investigations revealed an average serum calcium of 9.7 mg/dL (reference: 8.5-10.2 mg/dL, study range: 9.1-10.2 mg/dL), serum creatinine of 0.83 mg/dL (reference in women: 0.59-1.04 mg/dL, study range: 0.66-2.8 mg/dL), and 1,25-hydroxycholecalciferol of 69 pg/mL (reference in women: 18-78 pg/mL, study range: 46-81 pg/mL). In terms of secondary end points, the average age was 56 years (range, 39-74 years). All patients were female. Four (66.66%) patients had a history of biopolymer injections in the buttocks, 1 (16.66%) patient had a history of gluteal implants, and 1 (16.66%) patient had a history of breast implants. The average time from biopolymer exposure to presentation was 10.4 years (range, 6-20 years) and the average duration of medical management was 2.6 years (range, 1-5 years). The average number of procedures was 2 (range, 1-5), with all patients undergoing debridement. The most common reconstructive technique was coverage with local tissue flaps in 4 (66.66%) patients, with split-thickness skin grafting in 1 (16.66%) patient and primary closure in 1 (16.66%) patient. The most frequent complication was dehiscence in 6 (46.15%) procedures, followed by seroma in 2 (15.38%) and surgical site infection in 1 (7.69%). No patients proceeded to dialysis-dependent renal failure. All patients experienced a resolution of serum hypercalcemia, an improvement in renal function, and a decrease in 1,25-hydroxyvitamin D level.
Discussion
Biopolymer-induced granulomatous hypercalcemia has traditionally been treated medically because of the morbidity associated with surgical debridement of the granulomatous tissue. Systemic disease activity is mediated through elevated serum 1,25-hydroxycholecalciferol. An unchecked host foreign body–granuloma response drives this increase through the increased expression and upregulation of 1-alpha-hydroxylase on host macrophages (Figure 8).8 Initial management of hypercalcemia begins with volume resuscitation and restoration of electrolyte balance followed by targeted inhibition of the pathways involved in calcium elevation including calcitonin, bisphosphonates, and desonumab, among other medications. Of particular importance in biopolymer-induced granulomatous hypercalcemia are corticosteroids, which directly downregulate the host macrophages responsible for the granuloma response. Other immunomodulatory agents have also been successfully used, including tetracycline antibiotics, 5-fluoro-uracil, methotrexate, and tumor necrosis factor inhibitors. Medical management is often only temporarily effective, with recurrence following treatment in up to 45% of cases and 82% of these cases progressing to renal failure.13 In cases recalcitrant to medical management, surgical intervention may play a role.
Surgical management through the excision of the inflamed tissue has long been an established treatment for the skin changes, nodularity, and fibrosis that follow biopolymer exposure.14 Wide excision has also shown promise in alleviating the systemic symptoms of this disease, including chronic pain, fatigue, and associated autoimmune conditions.15 Surgical excision was first described as a successful treatment of granulomatous hypercalcemia in 1993 in a patient with sarcoidosis and giant cell granulomas of the spleen.16 Only more recently, however, has surgical management of biopolymer-induced granulomatous hypercalcemia been described.17-19
Different techniques have been described depending on the plane affected, including ultrasound-assisted lipoplasty with or without immediate fat transfer and wide debridement with local, regional, or free-flap coverage.11,17-19 While it may be impossible to remove all the biopolymer, the primary surgical goal is to remove the maximum amount of active granulomatous tissue and biopolymer, thus reducing the body burden to a manageable level. Biopolymer-exposed patients are at a high risk of local wound complications including seroma, dehiscence, surgical site infection, and fistula formation.10 Complications should be expected and preemptive measures taken to mitigate their risk. Even with the use of quilting sutures, tissue sealants, drains, negative pressure wound therapy, and postoperative antibiotics, a high rate of complications still occurred in this study. This may be due to the chronic inflammatory milieu surrounding the biopolymer particles or as of yet unknown properties intrinsic to the particles themselves. While not utilized in this study, solutions to facilitate the removal of biopolymer have become increasingly popular and include 20% poloxamer 188 (Shur-clens, ConvaTec), 10% povidone-iodine, and a 0.6% to 0.9% clindamycin-saline admixture.20-22 These may work through surfactant, coagulant, and flocculant mechanisms to facilitate silicone removal.
Surgical resection of biopolymer or foreign body granulomas may normalize serum calcium and improve renal insufficiency. This case report and systematic review is the largest report to date investigating this topic, with all patients experiencing a resolution of hypercalcemia and improvement in renal function. Larger series and comparative studies may further elucidate what patients may most benefit from surgical management of biopolymer-induced granulomatous hypercalcemia; they may also elucidate what amount of biopolymer must be resected to experience an improvement, as well as what modifying factors may be involved in the progression of biopolymer-induced granulomatous hypercalcemia to renal failure in an effort to minimize the number of operative interventions and risk of complications.
Acknowledgments
Authors: Dieter Brummund, MD1; Angela Chang, MD2; Christopher Salagdo, MD3
Affiliations: 1Larkin Community Hospital, Miami, Florida; 2HCA Florida - Mercy Hospital, Miami, Florida; 3Constructive Surgery Associates, Miami, Florida.
Correspondence: Dieter Brummund, MD. Larkin Community Hospital, 7031 SW 62nd Ave, Miami, Florida 33143, USA. E-mail: dbrummund@larkinhospital.com
Ethics: This review of 2 cases and the publicly available published literature was exempt from review by the institutional review board.
Disclosures: Dr Salgado is a speaker for Sanara MedTech (Fort Worth, Texas), the manufacturer of CellerateRX Surgical Powder. The remaining authors disclose no financial or other conflicts of interest.
References
- Salzman MJ. Silent rupture of silicone gel breast implants: high-resolution ultrasound scans and surveys of 584 women. Plast Reconstr Surg. 2022;149(1):7-14. doi:10.1097/PRS.0000000000008632
- Mayer JE, Goldberg DJ. Injuries attributable to cosmetic procedures performed by unlicensed individuals in the United States. J Clin Aesthet Dermatol. 2015;8(10):35-37.
- Knox KR, Granick MS, Mitchell AT, Fonseca RB. Infection with nontuberculous mycobacterium after injection of adulterated silicone fluid. Aesthet Surg J. 2004;24(4):342-345. doi:10.1016/j.asj.2004.04.003
- Montemurro P, Pellegatta T, Burton H, Pafitanis G. Silicone migration from breast implants: a case of ocular siliconoma and literature review. Aesthet Surg J. 2023;43(9):972-977. doi: 10.1093/asj/sjad086
- Bartsich S, Wu JK. Silicon emboli syndrome: a sequela of clandestine liquid silicone injections. A case report and review of the literature. J Plast Reconstr Aesthet Surg. 2010;63(1):e1-3. doi:10.1016/j.bjps.2009.04.004
- Jakobsen SR, Diaz-delCastillo M, Jensen MB, Andersen TL, Eldrup E, Nielsen TS. Case report: death caused by multi-organ metastatic calcifications as a result of intramuscular injections with paraffin oil. Bone Rep. 2024;20:101749. doi:10.1016/j.bonr.2024.101749
- Lemperle G, Gauthier-Hazan N, Wolters M, Eisemann-Klein M, Zimmermann U, Duffy DM. Foreign body granulomas after all injectable dermal fillers: part 1. Possible causes. Plast Reconstr Surg. 2009;123(6):1842-1863. doi:10.1097/PRS.0b013e31818236d7
- Shikama Y, Kobayashi K, Kasahara K, et al. Granuloma formation by artificial microparticles in vitro. Macrophages and monokines play a critical role in granuloma formation. Am J Pathol. 1989;134(6):1189-1199.
- Naim JO, Lanzafame RJ, van Oss CJ. The effect of silicone-gel on the immune response. J Biomater Sci Polym Ed. 1995;7(2):123-132. doi:10.1163/156856295x00643
- Lee JM, Kim YJ. Foreign Body Granulomas after the use of dermal fillers: pathophysiology, clinical appearance, histologic features, and treatment. Arch Plast Surg. 2015;42(2):232-239. doi:10.5999/aps.2015.42.2.232
- Novo RC, Salgado CJ, Yim E, Sinha V, Chim HW, Romanelli P. A staging system for gluteal foreign body reaction to injectables. J Plast Reconstr Aesthet Surg. 2016;69(8):e174-e179. doi:10.1016/j.bjps.2016.05.007
- Yahyavi-Firouz-Abadi N, Menias CO, Bhalla S, Siegel C, Gayer G, Katz DS. Imaging of cosmetic plastic procedures and implants in the body and their potential complications. AJR Am J Roentgenol. 2015;204(4):707-715. doi:10.2214/AJR.14.13516
- Tachamo N, Donato A, Timilsina B, et al. Hypercalcemia associated with cosmetic injections: a systematic review. Eur J Endocrinol. 2018;178(4):425-430. doi:10.1530/EJE-17-0938
- Salgado CJ, Sinha VR, Desai U. Liposuction and lipofilling for treatment of symptomatic silicone toxicosis of the gluteal region. Aesthet Surg J. 2014;34(4):571-577. doi: 10.1177/1090820X14527107
- Montealegre G, Uribe R, Martínez-Ceballos MA, Rojas-Villarraga A. ASIA syndrome symptoms induced by gluteal biopolymer injections: case-series and narrative review. Toxicol Rep. 2021;8:303-314. doi:10.1016/j.toxrep.2021.01.011
- Kruithoff KL, Gyetko MR, Scheiman JM. Giant splenomegaly and refractory hypercalcemia due to extrapulmonary sarcoidosis. Successful treatment by splenectomy. Arch Intern Med. 1993;153(24):2793-2796.
- Edwards BJ, Saraykar S, Sun M, Murphy WA Jr, Lin P, Gagel R. Resection of granulomatous tissue resolves silicone induced hypercalcemia. Bone Rep. 2015;5:163-167. doi:10.1016/j.bonr.2015.07.001
- Huff ML, Mehta N, Jacobs AM, Miles MG. A severe case of siliconoma-induced hypercalcemia due to illicit gluteal silicone injections. Plast Reconstr Surg Glob Open. 2022;10(3):e4184. doi:10.1097/GOX.0000000000004184
- Rodriguez IE, Deleyiannis FW. Hypercalcemia secondary to silicone breast implant rupture: a rare entity to keep in mind. Plast Reconstr Surg Glob Open. 2017;5(7):e1416. doi:10.1097/GOX.0000000000001416
- Bitar GJ, Nguyen DB, Knox LK, Dahman MI, Morgan RF, Rodeheaver GT. Shur-clens: an agent to remove silicone gel after breast implant rupture. Ann Plast Surg. 2002;48(2):148-153. doi:10.1097/00000637-200202000-00005
- Avila FR, Mazer LS, Borna S, et al. Breast pocket lavage with clindamycin solution for silicone removal after implant rupture. Aesthet Surg J. 2024;44(3):NP233-NP235. doi:10.1093/asj/sjad346
- Fell C, Kachare MD, Nixon A, et al. The "clinda-clumper" - a quick and efficient method to remove free silicone after a breast implant rupture using a clindamycin solution. Eplasty. 2024;24:QA8.