Misconceptions in Plastic Surgery: Crowdsourcing Public Perceptions of Plastic Surgery Urban Myths
© 2025 HMP Global. All Rights Reserved.
Any views and opinions expressed are those of the author(s) and/or participants and do not necessarily reflect the views, policy, or position of ePlasty or HMP Global, their employees, and affiliates.
Abstract
Background: Understanding public misconceptions about plastic surgery can inform plastic surgeons of the knowledge gaps among their patients and non-plastic surgeon colleagues about the field. This deepened understanding may aid in optimizing patient satisfaction and health outcomes. The objective of this study was to investigate the extent to which laypeople agree with common plastic surgery urban myths.
Methods: A Likert scale-based survey of 10 popular plastic surgery myths was distributed via Amazon Mechanical Turk. Descriptive analyses and multinomial logistical regressions were performed to assess associations between respondent demographics and the likelihood of agreeing with each myth.
Results: A total of 2000 completed surveys were included in this study. Of the respondents, 41% believed that hand dominance is associated with a larger ipsilateral breast, 40% believed that underwire bras cause breast cancer, and 59% believed that typing causes carpal tunnel syndrome. Respondents who were male or younger than 35 years were more likely to believe in inaccurate myths. Health care workers had higher odds of agreeing with the claims that plastic surgery uses plastic (odd ratio [OR] = 2.49 [95% CI, 1.82–3.41]; P < .001) and that plastic surgery is almost always cosmetic (OR = 1.85 [95% CI, 1.32-2.61]; P < .001). Participants who underwent a plastic surgery procedure or consultation were generally more likely to agree with the listed myths.
Conclusions: The general public and non-plastic-surgeon health care workers appear to have misconceptions about the scope and practice of plastic surgery. Open-ended patient-physician communication and patient-centered educational resources can potentially overcome plastic surgery misconceptions, thereby optimizing patient health outcomes and satisfaction.
Introduction
The general public and non-plastic-surgery health care professionals share a multitude of misconceptions regarding the scope of plastic surgery and the conditions treated by plastic surgeons, some of which have been described in the lay media.1-3 These misconceptions about medical facts may lead to urban myths that can impede the understanding of and communication about medical conditions between plastic surgeons and their patients. Furthermore, plastic surgeons rely heavily on other health care providers for patient referrals, and a misconception of plastic surgery may lead to loss of potential referrals or delayed management of critical cases.4 For patients, a limited understanding of the field may lead to hesitations in seeking out non-cosmetic care by plastic surgeons, which can further delay and even prevent them from receiving medically indicated plastic surgery treatment.5,6
While several studies have examined the perceptions of plastic surgery held by the public,6-15 none have explored the extent to which the public agrees or disagrees with urban myths commonly associated with plastic surgery. Understanding what misconceptions are held by the public would allow the plastic surgery community to become aware of which knowledge gaps need to be bridged and represents an essential step toward optimizing patient satisfaction and health outcomes. Thus, the objective of this study was to leverage crowdsourcing methods to gain insight into laypeople’s misconceptions about plastic surgery.
Methods and Materials
This cross-sectional study was conducted between November and December 2023 through an anonymous questionnaire using Google Forms and distributed to respondents using crowdsourcing via Amazon Mechanical Turk (MTurk).16,17 Internet crowdsourcing is a method of obtaining ideas, opinions, services, or data whereby members of the public complete an online task for a small monetary compensation, allowing users to outsource tasks to a large, diverse group of internet users.18 MTurk is an internet service that provides an on-demand human workforce from around the globe, allowing for diverse and rapid responses. This methodology has been used in prior survey-based plastic surgery research.19-24 This study was reviewed and approved by the Institutional Review Board as minimal risk human subjects research.
Participant recruitment
The survey was limited to MTurk participants who had previously completed more than 1000 assignments with an assignment approval rating greater than 95%, as this generally suggests that a respondent has a reputable survey history.25 Participants were offered 5 cents ($0.05) for completing the survey. Each user was required to share a unique identification code to receive payment upon survey completion. Unique and non-repeated codes ensured that each respondent completed the survey only once. Our goal was to reach a total of 2000 respondents, consistent with prior survey-based studies in plastic surgery.7,9,10
Survey development
The following demographic information was requested in the survey: age, gender, prior plastic surgery procedure, prior plastic surgery consultation, and whether the participant is a health care professional. The senior author asked several dozen colleagues at national plastic surgery conferences about myths they have encountered in their discussions with patients. From these discussions, as well as myths circulating in the media, a list of 10 common anecdotal misconceptions was created. The myths were then rewritten into positive phrasing to maintain consistency. For example, the myth that plastic surgeons do not perform emergency surgeries (false) was transformed into the positive statement that plastic surgeons do perform these procedures.
The final survey statements are the following: (1) Plastic surgery leaves scars; (2) Plastic surgery uses plastic; (3) Plastic surgery is almost always cosmetic; (4) Plastic surgeons perform emergency and trauma surgeries; (5) Wounds heal faster when left open to air and allowed to dry out; (6) If someone is right-hand dominant, they will have a larger right breast (and vice versa); (7) Underwire bras cause breast cancer (8) Typing causes carpal tunnel syndrome; (9) It is dangerous to wash your hands while recovering from hand surgery; and (10) Poor hygiene causes acne and hidradenitis (a condition that features lumps in places such as the armpits or groin).
For each statement, the participant was requested to answer with their level of agreement according to the following Likert scale: 1 = Strongly Disagree, 2 = Somewhat Disagree, 3 = Unsure, 4 = Somewhat Agree, 5 = Strongly Disagree. Throughout this article, “agreed” refers to the combination of strongly and somewhat agree (ie, options 1 and 2), and “disagreed” refers to the combination of strongly and somewhat disagree (ie, options 4 and 5).
To maximize response validity, the following attention check question was included midway through the survey: “What planet do we live on?”: (1) Saturn, (2) Earth, (3) Mars, (4) Jupiter, or (5) Mars. Respondents who answered any option other than “Earth” were excluded and prevented from taking the survey a second time.
Statistical analysis
Descriptive analyses with frequencies and proportions of the survey responses were performed. A chi-square test of independence was performed to assess whether the respondents’ characteristics were significantly associated with their responses to each survey question. Multinomial logistical regressions were performed to assess the strength of the associations between gender, age group, prior plastic surgery experience, and role as a health care professional and responses to the statements in the survey. For age categories, survey respondent ages were grouped into the following age ranges: 18 to 24, 25 to 34, 35 to 44, 45 to 54, 55 to 64, and 65 to 80 years. The 25- to 34-year age group was set as the reference for the multinomial logistical regression because most of the respondents (43%) were in this age group. Odds ratios (ORs) and corresponding 95% confidence intervals (CIs) were reported. All analyses were conducted using RStudio (RStudio Team, 2020), and P values of less than .05 were deemed statistically significant.
Results
Baseline demographics
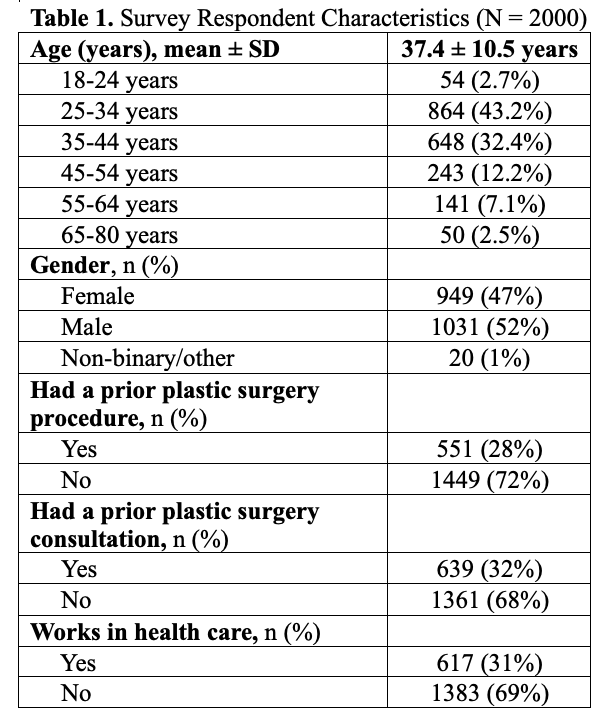
A total of 2000 completed surveys were included in this study (Table 1). The average age of the respondents was 37.4 ± 10.5 years (range, 18-79 years). Of the respondents, 949 (47%) and 1031 (52%) identified as female and male, respectively; 20 (1%) respondents identified as non-binary or other. Most respondents had not had a prior plastic surgery procedure (n = 1449, 72%) or a prior plastic surgery consultation (n = 1361, 68%). There were 617 respondents (31%) who reported working or training in health care.
Overall Likert responses
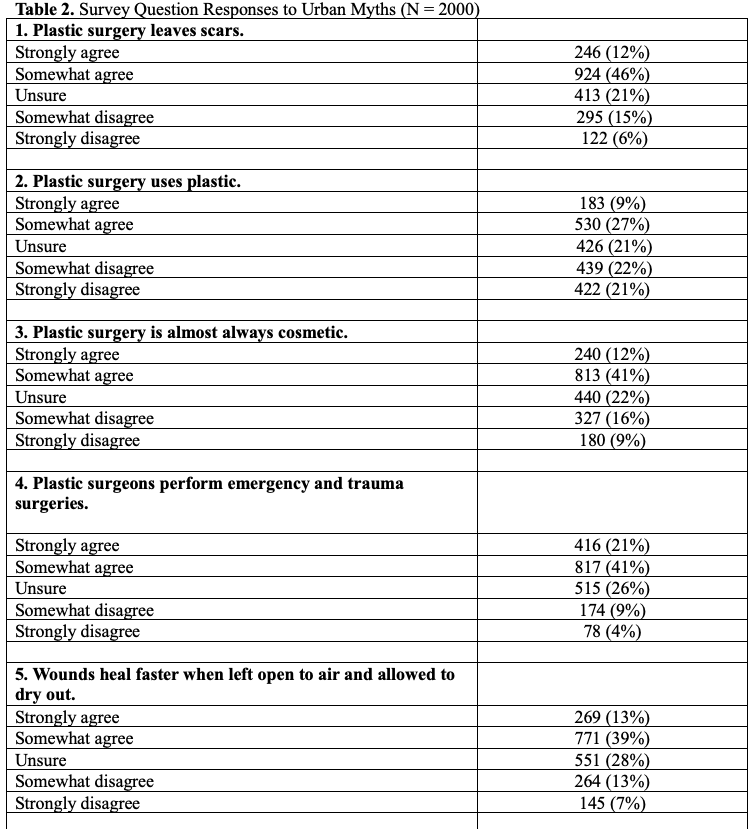
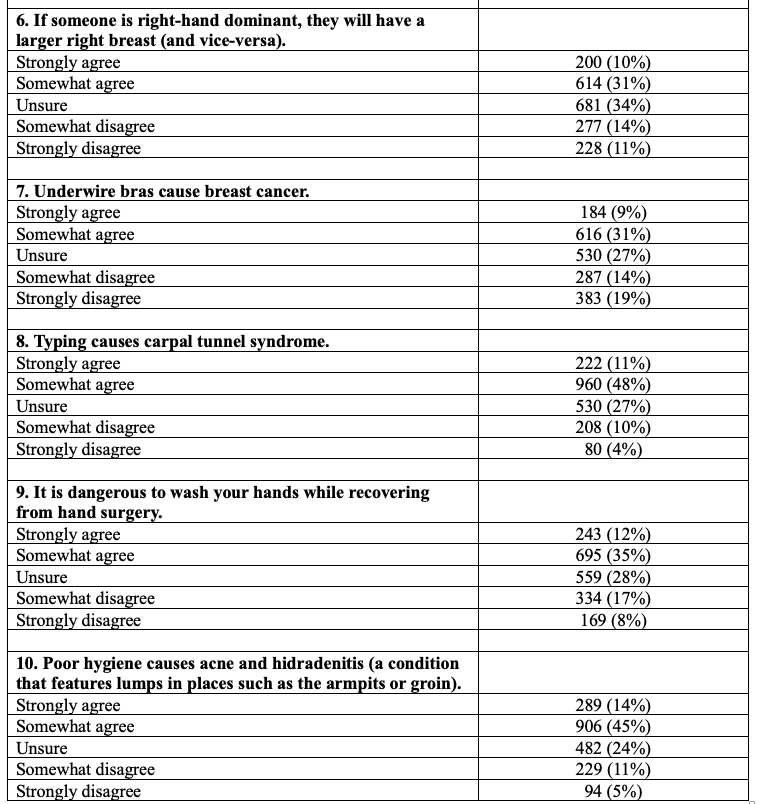
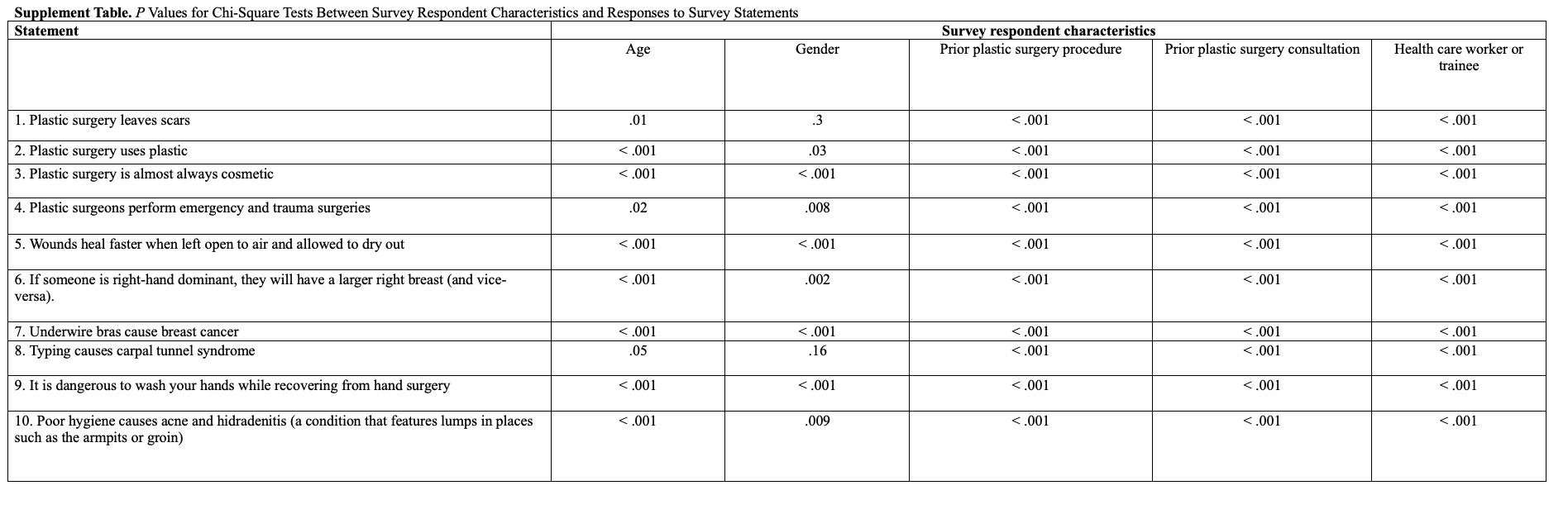
The Likert-scale responses to all the survey statements are presented in Figure 1 and Table 2. Over half of the respondents (52.7%) believed that plastic surgery is almost always cosmetic. Over a quarter of the respondents were unsure (25.8%) or disagreed (12.6%) that plastic surgeons perform emergency and trauma surgeries. Many respondents (40.0%) believed that wearing underwire bras causes breast cancer, and 40.7% of the respondents believed that hand dominance is associated with a larger ipsilateral breast. The chi-square test of independence indicated that health care worker or trainee status and a prior plastic surgery consultation or procedure were statistically significantly associated with the participants’ responses to each of the myths examined. Age and gender were significantly associated with a portion of the myths (Supplemental Table).
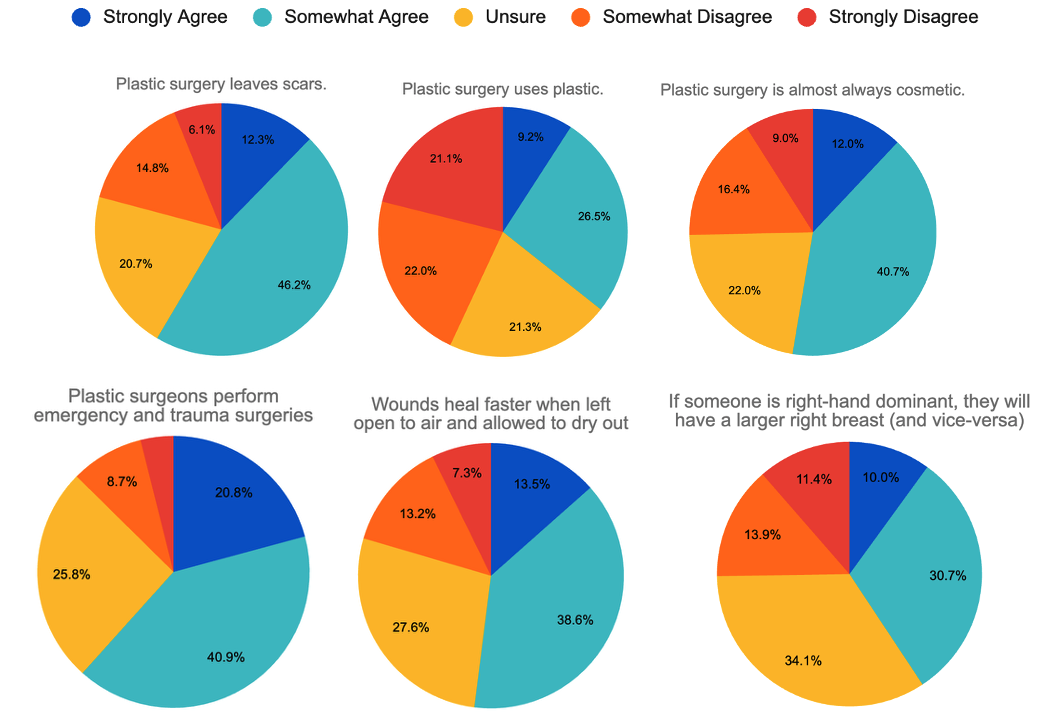
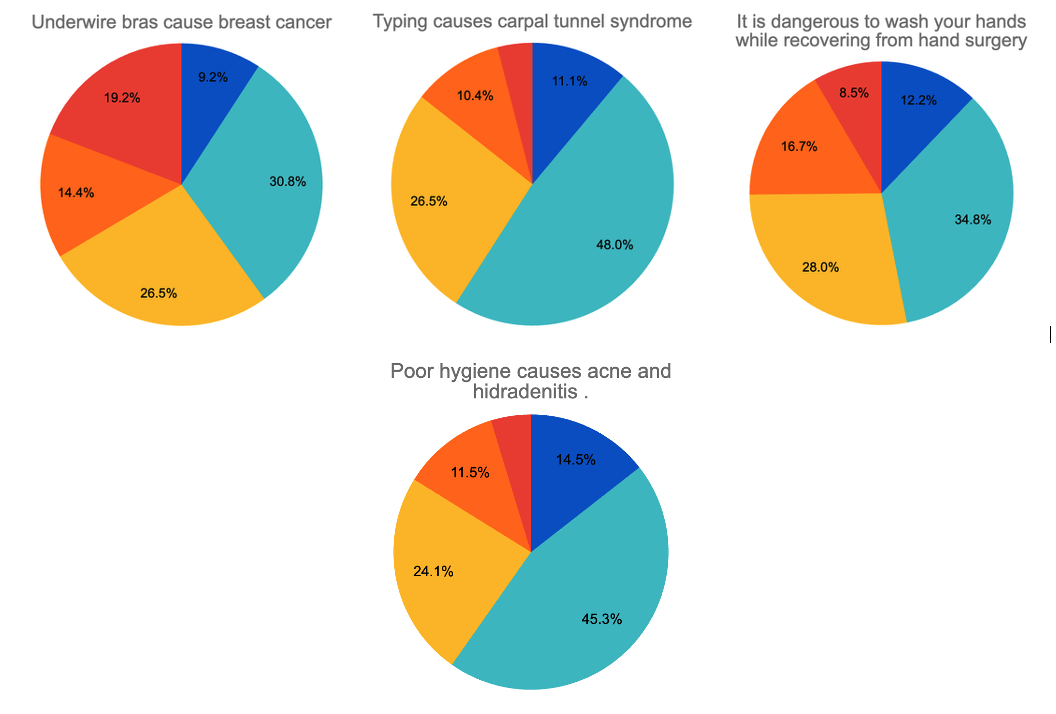
Figure 1. Urban myths in plastic surgery: survey of the general population on Amazon Mechanical Turk.
Likert responses based on age
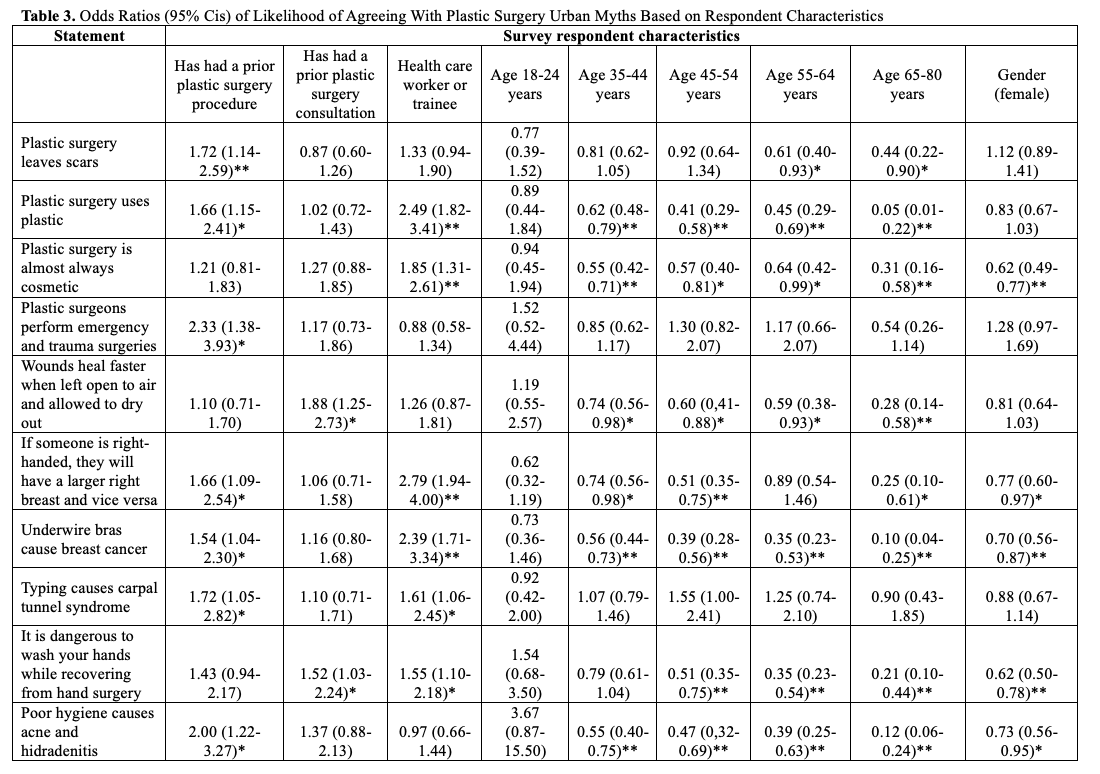
Older respondents were more likely to have accurate perceptions regarding the plastic surgery urban myths (Table 3). For example, participants aged 35 to 80 years were significantly less likely to agree that plastic surgery uses plastic, that hand dominance is associated with an increased ipsilateral breast size, and that washing hands is dangerous after hand surgery. Likewise, all age groups older than 25 to 34 years were significantly less likely to agree that wounds heal faster when left open, that underwire bra use causes cancer, and that poor hygiene causes acne or hidradenitis, with a stepwise decrease in ORs observed with each increasing age category.
 *P < .05; **P < .001
*P < .05; **P < .001
The likelihood of agreeing to a statement for each survey respondent characteristic is compared to its counterpart. The responses of respondents with prior plastic surgery procedures are compared to the responses of those who have not had past plastic surgery exposure.The responses of respondents with a prior plastic surgery consultation are compared to the responses of those who have not had past plastic surgery consultations. The responses of respondents who are health care workers/trainees are compared to the responses of those are not health care workers/trainees. The responses of all age groups are compared to the responses of those aged 25-34 years. The responses of female and non-binary/other gender respondents are compared to the responses of male respondents.
Likert responses based on gender
Male respondents were more likely to have inaccurate perceptions of the myths. Female respondents had lower odds of agreeing that plastic surgery is almost always cosmetic (OR = 0.62; 95% CI, 0.49-0.77; P < .001), hand dominance is associated with a larger ipsilateral breast (OR = 0.77; 95% CI, 0.60-0.97; P = .027), underwire bras cause breast cancer (OR = 0.70; 95% CI, 0.56-0.87; P = .001), it is dangerous to wash hands after hand surgery (OR = 0.62; 95% CI, 0.50-0.78; P < .001), and poor hygiene causes acne or hidradenitis (OR = 0.73; 95% CI, 0.56-0.95; P = .017) compared with those who identified as male.
Likert responses based on prior plastic surgery procedure
Respondents with past plastic surgery procedures had mixed accuracy in their beliefs of different myths. For example, participants with a prior plastic surgery procedure were more likely to accurately agree (OR = 1.72; 95% CI, 1.14-2.59; P = .010) and less likely to be unsure (OR = 0.54; 95% CI, 0.32-0.93; P = .026) that plastic surgery leaves scars compared with respondents who did not have a prior plastic surgery procedure. These participants were also more likely to agree that plastic surgeons perform emergency or trauma surgeries (OR = 2.33; 95% CI, 1.38-3.93; P = .002).
However, respondents with prior plastic surgery procedures were also more likely to have certain inaccurate perceptions. For example, they were more likely to believe the following myths: plastic surgery uses plastic (OR = 1.66; 95% CI, 1.15-2.41; P = .007); hand dominance is associated with ipsilateral larger breasts (OR = 1.66; 95% CI, 1.09-2.54; P = .018); wearing underwire bras can cause breast cancer (OR = 1.54; 95% CI, 1.04-2.30; P = .033); typing causes carpel tunnel (OR = 1.72; 95% CI, 1.05-2.82; P = .032); and poor hygiene causes acne and hidradenitis (OR = 2.00; 95% CI, 1.22-3.27; P = .006).
Likert responses based on prior plastic surgery consultation
Respondents who had a prior plastic surgery consultation had higher odds of agreeing that wounds heal faster when left open (OR = 1.88; 95% CI, 1.25-2.83; P = .002) and that it is dangerous to wash hands while recovering from hand surgery (OR = 1.52; 95% CI, 1.03-2.24; P = .035).
Likert responses based on health care worker or trainee
Health care workers and trainees hold many misconceptions about the field of plastic surgery. For example, health care workers/trainees had higher odds of agreeing that plastic surgery uses plastic (OR = 2.49; CI, 1.82-3.41; P < .001) and that plastic surgery is almost always cosmetic (OR = 1.85; 95% CI, 1.32-2.61; P < .001) compared with those who were not in health care.
Health care workers/trainees also had higher odds of agreeing that hand dominance is associated with a larger ipsilateral breast (OR = 2.79; 95% CI, 1.94-4.00; P < .001), wearing underwire bras can cause breast cancer (OR = 2.39; 95% CI, 1.71-3.34; P < .001), typing causes carpel tunnel (OR = 1.61; 95% CI, 1.06-2.45; P = .024), and it is dangerous to wash hands while recovering from hand surgery (OR = 1.55; 95% CI, 1.10-2.18; P = .012).
Discussion
Understanding the public’s knowledge gaps regarding plastic surgery can help lay the framework for better education, communication, and patient health outcomes. This study sought to crowdsource beliefs regarding various urban myths related to plastic surgery. We found that the public holds common beliefs in various myths. The limited understanding of plastic surgery even extends to those who are in health care or those who have had past exposure to plastic surgery.
A common misconception is that plastic surgery is purely cosmetic, when in fact plastic surgery is one of the most wide-ranging fields in medicine, encompassing both reconstructive and aesthetic surgery. In 2020, surgeons certified by the American Board of Plastic Surgery (ABPS) performed nearly 7 million reconstructive procedures, which is 3 times more than the aesthetic procedures that were performed.26 In 2022, reconstructive procedures made up 40% of the total surgeries conducted by ABPS plastic surgeons.27 Most respondents in our study believed that the scope of plastic surgery is almost entirely cosmetic, consistent with findings in other survey-based studies.5-11,15,23 In 2016, Denadai et al found that their survey respondents strongly associated plastic surgeons with aesthetic surgery and not with craniofacial, chest wall, or tumor removal surgery.10 Interestingly, in their 2015 analysis of 899 of survey respondents, Blacam et al found that laypeople attending the emergency department ranked plastic surgery as the lowest of 30 specialties in terms of importance in providing care for patients at the hospital.6 The versatility of plastic surgery can lead to confusion among those outside the field about what a plastic surgeon actually does,7 a problem that gets compounded by the media’s emphasis on cosmetic procedures.28-30
In this study, health care workers were more likely to agree that plastic surgery uses plastic, and that plastic surgery is almost always cosmetic, demonstrating an inadequate awareness about the field even within health care professions. While some studies show that general practitioners and medical students demonstrate a better understanding of the diversity of the specialty than the general public,7,15 many other studies have found that health care professionals or trainees, including but not limited to primary care physicians, medical students, nurses, and physical therapists, have limited awareness of the scope of plastic surgery, associating the field more with cosmetics than other areas.12-14,31-34 While this is not directly answered by our study or prior studies, a lack of awareness about the breadth of plastic surgery from other health care professionals can potentially lead to delays in appropriate treatment. For example, plastic surgeons rely heavily on primary care physicians for patient referrals, and a misconception of plastic surgery may lead to loss of potential referrals or delayed management of critical cases.4
In addition to exploring perceptions about the field’s scope, we explored the public’s levels of agreement with common misconceptions regarding plastic surgery and its related conditions. This is the first study to explore the public’s beliefs in specific plastic surgery urban myths. For example, one-third of the participants believed that plastic surgery uses plastic, demonstrating an underlying lack of understanding of the field. Plastic surgery gets its name from the Greek word “plastikos,” which means to form or to mold—not because it involves the use of plastic. Furthermore, we found that an alarming 40% of respondents believed that wearing underwire bras can cause breast cancer. This misconception, stemming from the belief that underwire bras press against tissue and impede lymph drainage, has no scientific credence.35 Our findings demonstrate that the public has inaccurate belief systems about many topics that plastic surgeons may consider basic knowledge, highlighting the importance of patient education and communication.
This study found that certain groups had more inaccurate perceptions of certain urban myths than others. For example, male respondents and younger survey respondents were significantly more likely to believe in inaccurate myths. This may be because the female and older participants have had more exposure to or knowledge about these topics, or because social media is exacerbating misconceptions among the youth and males. Targeted educational interventions towards males and younger age groups may help curb the spread of disinformation among these groups.
Compassionate, open, and effective patient-physician communication will be integral to disproving misconceptions about the field. With clear communication, patient involvement, and strong interpersonal skills, patient satisfaction has been shown to increase.36 This open environment may encourage patients to be more comfortable asking questions they otherwise may be too nervous to ask. In this study, inaccurate perceptions were held even among respondents who have had past plastic surgery exposure, whether through a consultation or a procedure. One study of 510 participants found that the health literacy among plastic surgery patients was inadequate, similar to the general population.37 Thus, it is of utmost importance that plastic surgeons provide clear pre- and postoperative instructions and general education about relevant medical conditions to their patients. Throughout a patient’s care, it will be important to confirm and clarify expectations about the condition and treatment; this includes any care that the plastic surgeon may think is intuitive, such as hand washing after hand surgery and wound management protocols, that the patient will need to perform on his or her own. No assumptions should be made about what the patient knows.
A multi-pronged approach will be an instrumental step to increase awareness about the scope of the field and dispel myths in bettering patient care and health outcomes. For example, it will be important to educate health care staff and doctors in different specialties about the field. Educating and encouraging health care trainees at earlier stages of training to explore plastic surgery subspecialties will promote a stronger grasp of the field in future generations of health care workers. Furthermore, given that many people develop their perception of plastic surgery-related topics through the media, including social media, television, magazines, and more,8,15,29,30,33,38,39 it is important to develop and disseminate educational materials through these various platforms to spread maximal awareness about the field and debunk related urban myths.
Limitations
This study has important limitations. First, the cross-sectional nature of the study and the use of MTurk are inherent limitations. Compensation may motivate participants to provide non-meaningful responses to questions if individuals are strongly motivated by the financial reward provided by completing the survey. However, our use of attention check questions likely minimized the likelihood of this occurrence.21,22,40 Second, to maintain brevity, we did not ask certain clarifying questions following our demographic questions. For example, we did not ask about specific plastic surgery exposures, such as whether respondents received nonoperative procedures or minimally invasive surgeries. Thus, we do not know the nature of the participants’ past exposures to plastic surgery, which may influence their knowledge base. Furthermore, we did not ask respondents to specify which type of health care worker or trainee they are. A more detailed set of demographical questions may be warranted in future survey-based studies. Third, we only focused on 10 urban myths that plastic surgeons have encountered and that the authors viewed in media outlets. We acknowledge that there are likely additional misconceptions that non-plastic surgeons may have about the field. The purpose of this pilot study is to lay the groundwork for future surveys that can be administered to larger populations with more questions to better understand what knowledge gaps exist among the public, ultimately leading to better communication and patient care.
Conclusions
This study suggests that the public has a limited understanding of the scope and practice of plastic surgery. Providing compassionate patient-physician communication and education to the general public and other health care professionals can help to dispel misconceptions about the field and the conditions treated by plastic surgeons, which may ultimately help improve patient care.
Acknowledgments
Authors: Navya Baranwal, BA1; Elijah M. Persad-Paisley, BA1; Nidhi Shinde, BDS, MPH2; Carole Spake, MD2; Jesse E. Menville, BA1; Raman Mehrzad, MD, MHL, MBA2; Nikhil Sobti, MD2; Loree K. Kalliainen, MD, MA2
Affiliations: 1The Warren Alpert Medical School of Brown University, Providence, Rhode Island; 2Divison of Plastic Surgery, The Warren Alpert Medical School of Brown University, Providence, Rhode Island
Correspondence: Navya Baranwal, BA, The Warren Alpert Medical School of Brown University, 222 Richmond Street, Providence, RI 02903, USA. Email: navya_baranwal@brown.edu
Ethics statement: This study was reviewed and approved by the Institutional Review Board as “Minimal Risk Human Subjects Research”: IRB Project Number-2083180.
Disclosures: The authors report no funding and no conflicts of interest concerning the methods or information used in this study.
References
1. Kim R. Top five plastic surgery myths. American Society of Plastic Surgeons. July 13, 2012. Accessed on December 28, 2023. https://www.plasticsurgery.org/news/blog/top-five-plastic-surgery-myths
2. Ray C. Bras and cancer. The New York Times. Accessed December 28, 2023
https://www.nytimes.com/2010/02/16/science/16qna.html?ref=science
3. Jackson-Gibson A. 7 things people of color should know about hidradenitis suppurativa. Self. February 24, 2023. Accessed on December 28, 2023 https://www.self.com/story/hidradenitis-suppurativa-people-of-color
4. Mrad MA, Al Qurashi AA, Mortada H, et al. Do our colleagues accurately know what we do? Plast Reconstr Surg Glob Open. 2022;10(2):e4104. doi:10.1097/GOX.0000000000004104
5. Almarghoub MA, Almarzouq SF, Alissa SI. Public perception of plastic surgery in Saudi Arabia. Plast Reconstr Surg Glob Open. 2019;7(3):e2143. doi:10.1097/GOX.0000000000002143
6. de Blacam C, Kilmartin D, Mc Dermott C, Kelly J. Public perception of plastic surgery. J Plast Reconstr Aesthet Surg. 2015;68(2):197-204. doi:10.1016/j.bjps.2014.10.008
7. Dunkin CS, Pleat JM, Jones SA, Goodacre TE. Perception and reality-a study of public and professional perceptions of plastic surgery. Br J Plast Surg. 2003;56(5):437-443. doi:10.1016/s0007-1226(03)00188-7
8. Gill P, Bruscino-Raiola F, Leung M. Public perception of the field of plastic surgery. ANZ J Surg. 2011;81(10):669-672. doi:10.1111/j.1445-2197.2011.05753.x
9. Sinno S, Barr J, Wilson S, Smith BD, Tanna N, Saadeh PB. Public perceptions of plastic surgery: analysis and implications. J Craniofac Surg. 2015;26(4):1238-1241. doi:10.1097/SCS.0000000000001756
10. Denadai R, Araujo KM, Samartine H Jr, Denadai R, Raposo-Amaral CE. Public perceptions of plastic surgery practice in Brazil. Indian J Surg. 2016;78(6):435-441. doi:10.1007/s12262-015-1388-3
11. Brown KW, Moss CA, McCandless MG, Mukit M, Walker ME. Plastic surgery: beware the candle burning at both ends. Plast Reconstr Surg Glob Open. 2023;11(12):e5495. doi:10.1097/GOX.0000000000005495
12. Tanna N, Patel NJ, Azhar H, Granzow JW. Professional perceptions of plastic and reconstructive surgery: what primary care physicians think. Plast Reconstr Surg. 2010;126(2):643-650. doi:10.1097/PRS.0b013e3181de1a16
13. Kumar V, Singh AK, Faisal A, Nandini R. Awareness among medical fraternity regarding the role of plastic surgeon. Indian J Plast Surg. 2011;44(3):494-497. doi:10.4103/0970-0358.90835
14. Agarwal JP, Mendenhall SD, Moran LA, Hopkins PN. Medical student perceptions of the scope of plastic and reconstructive surgery. Ann Plast Surg. 2013;70(3):343-349. doi:10.1097/SAP.0b013e31823b6c19
15. Agarwal P. Perception of plastic surgery in the society. Indian J Plast Surg. 2004;37(02): 110-114. doi:10.1055/s-0039-1697221
16. Buhrmester M, Kwang T, Gosling SD. Amazon's Mechanical Turk: a new source of inexpensive, yet high-quality, data? Perspect Psychol Sci. 2011;6(1):3-5. doi:10.1177/1745691610393980
17. Paolacci G, Chandler J, Ipeirotis PG. Running experiments on Amazon Mechanical Turk. Judgment and Decision Making. 2010;5(5):411-419. doi:10.1017/S1930297500002205
18. Estellés-Arolas E, González-Ladrón-de-Guevara F. Towards an integrated crowdsourcing
definition. Journal of Information Science. 2012;38(2):189-200. doi:10.1177/0165551512437638
19. Wu C, Scott Hultman C, Diegidio P, et al. What do our patients truly want? conjoint analysis of an aesthetic plastic surgery practice using internet crowdsourcing. Aesthet Surg J. 2017;37(1):105-118. doi:10.1093/asj/sjw143
20. Vartanian E, Gould DJ, Hammoudeh ZS, Azadgoli B, Stevens WG, Macias LH. The ideal thigh: a crowdsourcing-based assessment of ideal thigh aesthetic and implications for gluteal fat grafting. Aesthet Surg J. 2018;38(8):861-869. doi:10.1093/asj/sjx191
21. Bucknor A, Christensen J, Kamali P, et al. Crowdsourcing public perceptions of plastic surgeons: is there a gender bias? Plast Reconstr Surg Glob Open. 2018;6(4):e1728. doi:10.1097/GOX.0000000000001728
22. Nayyar A, Jadi J, Garimella R, et al. Are you on the right platform? A conjoint analysis of social media preferences in aesthetic surgery patients. Aesthet Surg J. 2019;39(9):1019-1032. doi:10.1093/asj/sjy238
23. Bustos VP, Xun H, McLarney J, et al. Misconceptions, myths, and mystery: a cross-sectional survey study on public knowledge and values of microsurgery. J Reconstr Microsurg. 2023;39(4):301-310. doi:10.1055/a-1896-5598
24. Lee E, Khavanin N, Xun H, et al. Identifying public perceptions, attitudes, and concerns about breast implants and their complications: a national survey. Plast Reconstr Surg. 2023;151(1):31e-39e. doi:10.1097/PRS.0000000000009820
25. Peer E, Vosgerau J, Acquisti A. Reputation as a sufficient condition for data quality on Amazon Mechanical Turk. Behav Res Methods. 2014;46(4):1023-1031. doi:10.3758/s13428-013-0434-y
26. Plastic surgery statistics report: ASPS national clearinghouse of plastic surgery procedural statistics. American Society of Plastic Surgeons. 2021. Accessed December 28, 2023. https://www.plasticsurgery.org/documents/News/Statistics/2020/plastic-surgery-statistics-full-report-2020.pdf
27. 2022 ASPS procedural statistics release. American Society of Plastic Surgeons. September 26, 2023. Accessed December 28, 2023. https://www.plasticsurgery.org/documents/News/Statistics/2022/plastic-surgery-statistics-report-2022.pdf
28. Reid AJ, Malone PS. Plastic surgery in the press. J Plast Reconstr Aesthet Surg. 2008;61(8):866-869. doi:10.1016/j.bjps.2008.06.012
29. Denadai R, Araujo KM, Samartine Junior H, Denadai R, Raposo-Amaral CE. Aesthetic surgery reality television shows: do they influence public perception of the scope of plastic surgery? Aesthetic Plast Surg. 2015;39(6):1000-1009. doi:10.1007/s00266-015-0577-6
30. Kalandar A, Al-Youha S, Al-Halabi B, Williams J. What does the public think? Examining plastic surgery perceptions through the Twitterverse. Plast Reconstr Surg. 2018;142(1):265-274. doi:10.1097/PRS.0000000000004484
31. Kling RE, Nayar HS, Harhay MO, et al. The scope of plastic surgery according to 2434 allopathic medical students in the United States. Plast Reconstr Surg. 2014;133(4):947-956. doi:10.1097/PRS.0000000000000164
32. Agarwal JP, Mendenhall SD, Hopkins PN. Medical student perceptions of plastic surgeons as hand surgery specialists. Ann Plast Surg. 2014;72(1):89-93. doi:10.1097/SAP.0b013e3182583f3b
33. Lupon E, Bedet A, Girard P, et al. The perception of plastic surgery by physiotherapists: a French national descriptive study. Ann Transl Med. 2020;8(5):184. doi:10.21037/atm.2020.01.109
34. Lupon E, Girard P, Lupon A, et al. The perception of plastic surgery by community-based, private practice nurses: a French national descriptive study. Plast Surg Nurs. 2021 Jan;41(1):18-25. doi:10.1097/PSN.0000000000000336
35. Chen L, Malone KE, Li CI. Bra wearing not associated with breast cancer risk: a population-based case-control study. Cancer Epidemiol Biomarkers Prev. 2014;23(10):2181-2185. doi:10.1158/1055-9965.EPI-14-0414
36. O'Rorke E, Mauch J, Liu Y, Friedrich J. Essential elements of surgeon communication impacting patient satisfaction: a systematic review. Plast Reconstr Surg Glob Open. 2021;9(10 Suppl):135-136. doi:10.1097/01.GOX.0000799800.31313.2b
37. Bustos VP, Haddad A, Kinney JR, et al. Evaluation of health literacy in plastic surgery using a crowdsourced patient survey. Plast Reconstr Surg Glob Open. 2023;11(2):e4803. doi:10.1097/GOX.0000000000004803
38. Park AJ, Scerri GV, Benamore R, McDiarmid JG, Lamberty BG. What do plastic surgeons do? J R Coll Surg Edinb. 1998;43(3):189-193.
39. Hardwicke J, Lam WL, Paterson P. 'What's in a name?'. J Plast Reconstr Aesthet Surg. 2007;60(8):955-956. doi:10.1016/j.bjps.2005.12.068
40. Mayfield CK, Thomas I, Shauly O, Gould DJ, Seruya M. Validating grading of aesthetic outcomes of web space reconstruction for finger syndactyly: crowdsourcing public perceptions using Amazon Mechanical Turk. Aesthet Surg J Open Forum. 2020;3(1):ojaa046. doi:10.1093/asjof/ojaa046