


Overactive Bladder Health Care Burden in the US Long-Term Care Setting: A Retrospective Cohort Study
Abstract
Overactive bladder (OAB) is highly prevalent in long-term care (LTC) facilities and may negatively impact health care resource utilization (HCRU) and costs. We undertook this retrospective study using LTC claims and hospital chargemaster data (2012-2019) to describe and evaluate the population, treatment patterns, HCRU, and costs associated with OAB in the US LTC setting by comparing residents with vs without OAB, and pharmacologically treated vs untreated residents with OAB. More residents with vs without OAB (n=159,785 each) had osteoarthritis and received antidepressants or CYP2D6 substrates. Residents with vs without OAB had significantly higher utilization of physician office and disease-specific outpatient visits and 17% higher all-cause health care costs. Fewer OAB pharmacologically treated (n=52,569) vs untreated (n=217,929) residents had physician office visits for urinary incontinence (22.8% vs 97.7%, respectively) and urinary catheterization (60.3% vs 99.3%). All-cause health care expenditures minus pharmacy costs were 23% lower for OAB treated vs untreated residents. Overall, OAB is associated with significant HCRU and economic burden in the US LTC setting; treating OAB resulted in reduced nonpharmacy costs, highlighting the need for better treatment management.
Supplementary Materials can be viewed in the PDF version of this article.
Introduction
More than 30 million Americans aged ≥40 years are affected by bothersome symptoms of overactive bladder (OAB),1 which negatively impact patient-reported quality of life.2 In long-term (LTC) residents of nursing homes (NHs) aged ≥65 years, the prevalence of OAB and/or urinary incontinence is estimated at 70%; in contrast, the prevalence in age-matched noninstitutionalized persons is estimated at 44%.3 Furthermore, the presence and severity of urinary incontinence has been shown to be a predictive factor for placement of older adults into LTC settings.4-6 Adults aged ≥65 years with OAB are more likely to have comorbid conditions and subsequent polypharmacy vs those without OAB.7 Few studies have assessed the impact of OAB in the LTC setting. However, one study showed that adults ≥65 years with OAB have higher health care resource utilization (HCRU) and associated costs than those without OAB during the 6-month period after NH admission.8 While the cost-effectiveness associated with individual OAB treatments has been established,9 it is unknown whether treating OAB reduces OAB-related HCRU and costs in the LTC setting.
The American Urological Association (AUA) recommends behavioral therapy as first-line treatment for OAB, which may be combined with medications; second-line therapy includes anticholinergics and β3-adrenergic agonists.10 While anticholinergics are effective in reducing urinary symptoms, they have side effects such as dry mouth, constipation, blurred vision, urinary retention, and impaired cognitive function.10 Therefore, the American Geriatrics Society Beers Criteria recommends avoiding anticholinergics in older adults.11 Use of anticholinergics is also associated with an increased risk of falls and fractures compared with no anticholinergic use, with greater cumulative anticholinergic burden associated with increased rate of falls and fractures.12-14 In a study of NH residents treated for OAB, most had concomitant moderate to severe cognitive impairment and/or severe mobility impairment,15 highlighting the high-risk population of OAB. Thus, describing the characteristics and burden of illness of residents with OAB in the LTC setting is important to inform appropriate treatments.
The overall objective of this study was to describe and evaluate the population, treatment patterns, HCRU, and costs associated with OAB in the LTC setting in the United States. Specific objectives included evaluating the burden of illness of OAB by examining differences in direct HCRU and costs among residents with OAB compared with a matched cohort of residents without OAB and among residents with OAB who were pharmacologically treated for OAB compared with residents with OAB who were not pharmacologically treated for OAB.
Methods
Study Design and Database
This retrospective cohort analysis of residents of LTC facilities was conducted using deidentified claims from IQVIA’s LTC pharmacy data linked to IQVIA’s New Data Warehouse. The New Data Warehouse includes about 1 billion professional fee claims/year representing more than 870,000 practitioners/month, prescription claims including more than 1.6 billion retail/mail order claims representing dispensed prescriptions for approximately 85% of US pharmacies, and a hospital charge data master including records from over 500 hospitals covering 7 million annual inpatient stays and 60 million annual outpatient visits. The database has prescriber- and patient-level data for about 165 pharmacies located within Community Mental Health Center Clinics (>3000 clinics). All datasets are compliant with the Health Insurance Portability and Accountability Act to protect patient privacy.
The overall study period was May 1, 2012, to May 31, 2019. The selection window to identify study cohorts of interest was May 1, 2013, to May 31, 2018, which allowed for a 12-month pre- and post-index period.
Eligibility, Cohort Matching, and Treatment Groups
Because the databases are open source, proxies for continuous enrollment were applied. Residents were required to have ≥1 office visit (in the diagnosis database) and ≥1 prescription claim (in the prescription or LTC database) during the 12-month pre- and post-index periods.
OAB and non-OAB cohorts: Adults with ≥2 non-same-day prescriptions for medications indicated for the treatment of OAB in the database between May 1, 2013, and May 31, 2018, were included in the OAB cohort (Supplementary Figure 1). Residents were also required to have pharmacy stability, defined as consistent reporting of data from the most frequently visited pharmacy (reporting of prescriptions from the same pharmacy each month for a period of 12 months during the selection window and during the 12-month pre- and post-index periods) and ≥80% coverage for each month in the 12-month pre- and post-index periods. Patient-level data were linked to the LTC, professional fee claims, and prescription claims databases. Residents were excluded if there were data quality issues (eg, invalid birth year, sex, region).
A random sample of claimants with no OAB-related prescriptions and ≥2 non-same-day prescriptions for non-OAB medications were extracted from the LTC data set. The non-OAB and OAB cohorts were compared pre- and post-match using standardized mean differences (SMDs). Residents with an SMD of ≥0.1 for clinical variables of interest before matching were matched to the OAB cohort using 1:1 propensity score matching with a maximum allowed propensity score difference of <0.000001. Variables for matching included use of durable medical equipment, comorbidities, age (categorical), sex, region, payer, index year, provider specialty at index date, Charlson Comorbidity Index, and days in LTC before index (categorical). The cohorts were considered well balanced for a variable if SMD was <0.10 post-match. Unsuccessfully matched residents (SMD >0.1) were excluded from further analyses.
OAB treated and untreated cohorts: Residents in the treated cohort had ≥2 prescriptions for an OAB medication of interest during the selection window in the LTC database (Supplementary Figure 2). Medications for OAB included urinary anticholinergics (darifenacin, fesoterodine, flavoxate, oxybutynin, solifenacin, tolterodine, trospium) and a β3-adrenergic agonist (mirabegron). The date of first prescription observed during the selection window was the index date.
Residents in the untreated cohort had ≥2 OAB diagnoses (any diagnosis of OAB, urinary incontinence, or hypertonic bladder) during the selection window and ≥1 non-OAB prescription in the LTC database. The date of first diagnosis was the index date; residents were required to have no prescriptions for OAB medications during the entire study period (May 1, 2012, to May 31, 2019 [inclusive of pre- and post-index periods]).
Statistics
Statistical analyses were performed using SAS v9.4. Differences in baseline demographic and clinical characteristics between the OAB and non-OAB cohorts were examined using standardized differences. Significance was demonstrated by SMD ≥0.1. For the matched cohorts (OAB vs non-OAB), differences in HCRU and costs were examined using McNemar’s test (categorical variables) and the Wilcoxon signed-rank test (continuous variables). For the unmatched cohorts (OAB treated vs untreated), comparisons were conducted using the chi-square test (categorical variables) and the Wilcoxon rank-sum test (continuous variables); because cohorts were unmatched, significance was measured using P values. Adjusted cost ratios for the OAB vs non-OAB cohorts and treated vs untreated cohorts were estimated using a generalized estimating equation model with log link and gamma distribution. Covariates considered for inclusion into the models included demographic and clinical characteristics of interest guided by univariate findings and were adjusted for using a general linear regression model. Candidate variables were considered and retained in the model if significant (P<.10).
Results
OAB vs Non-OAB Cohorts
After attrition, the OAB cohort included 159,785 residents, and the unmatched non-OAB cohort included 212,616 residents. After matching, both cohorts included 159,785 residents (Supplementary Figure 1). The OAB and non-OAB cohorts were relatively well balanced in terms of demographic characteristics except sex (as expected, most OAB residents were women) and year of index date (Table 1). Mean age was similar between cohorts (OAB, 75.3 years; non-OAB, 74.7 years). 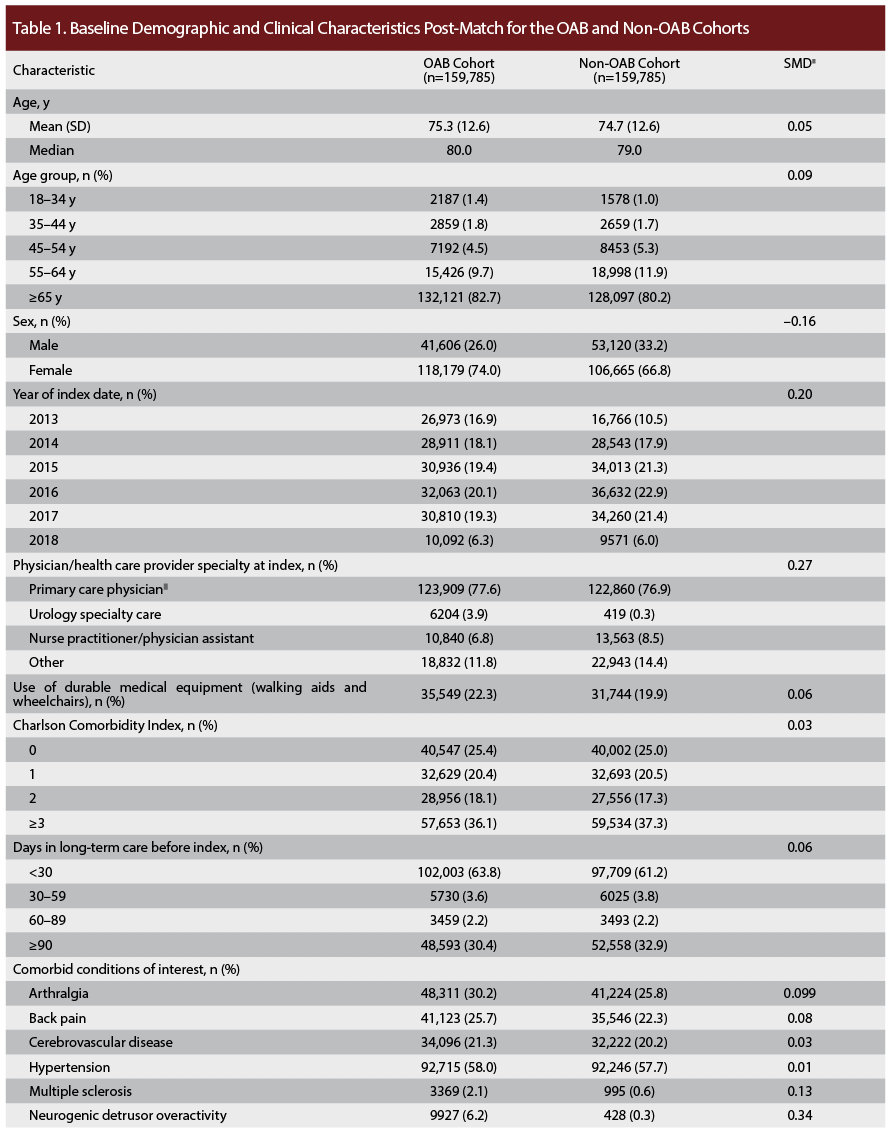
Differences were observed between the OAB and non-OAB cohorts with respect to select baseline clinical characteristics regarding comorbid conditions of interest (multiple sclerosis and osteoarthritis in residents with OAB) and medications of interest (Table 1). Overall prescription claims for medications that are substrates of cytochrome P450 (CYP) 2D6 were significantly greater in the OAB vs non-OAB cohort (73.8% vs 67.3%, respectively; SMD, 0.14), including those associated with QTc prolongation (38.5% vs 28.7%; SMD, 0.21). Use of antidepressants was also significantly greater in the OAB vs non-OAB cohort (54.3% vs 45.7%; SMD, 0.17), as was use of analgesics (71.5% vs 65.1%, respectively; SMD, 0.14). At baseline, residents in the OAB cohort had higher all-cause and disease-specific HCRU compared with residents in the non-OAB cohort (Supplementary Table 1).
HCRU for the OAB and non-OAB cohorts during the 12-month post-index period is shown in Figure 1. A significantly greater proportion of residents with vs without OAB had physician office visits (SMD, 0.14; P<.001) and outpatient visits related to urinary conditions (urinary tract infection [UTI]: SMD, 0.28; P<.001; urinary catheterization: SMD, 0.42; P<.001; OAB/hypertonic bladder/urinary incontinence: SMD, 0.55; P<.001) and falls/fractures (SMD, 0.12; P<.001), suggesting significant all-cause and disease-specific burden among residents with OAB in the LTC setting. During the 12-month post-index period, the median number of prescriptions per month was 9 and 6 for the OAB and non-OAB cohort, respectively (SMD, 0.52; P<.001).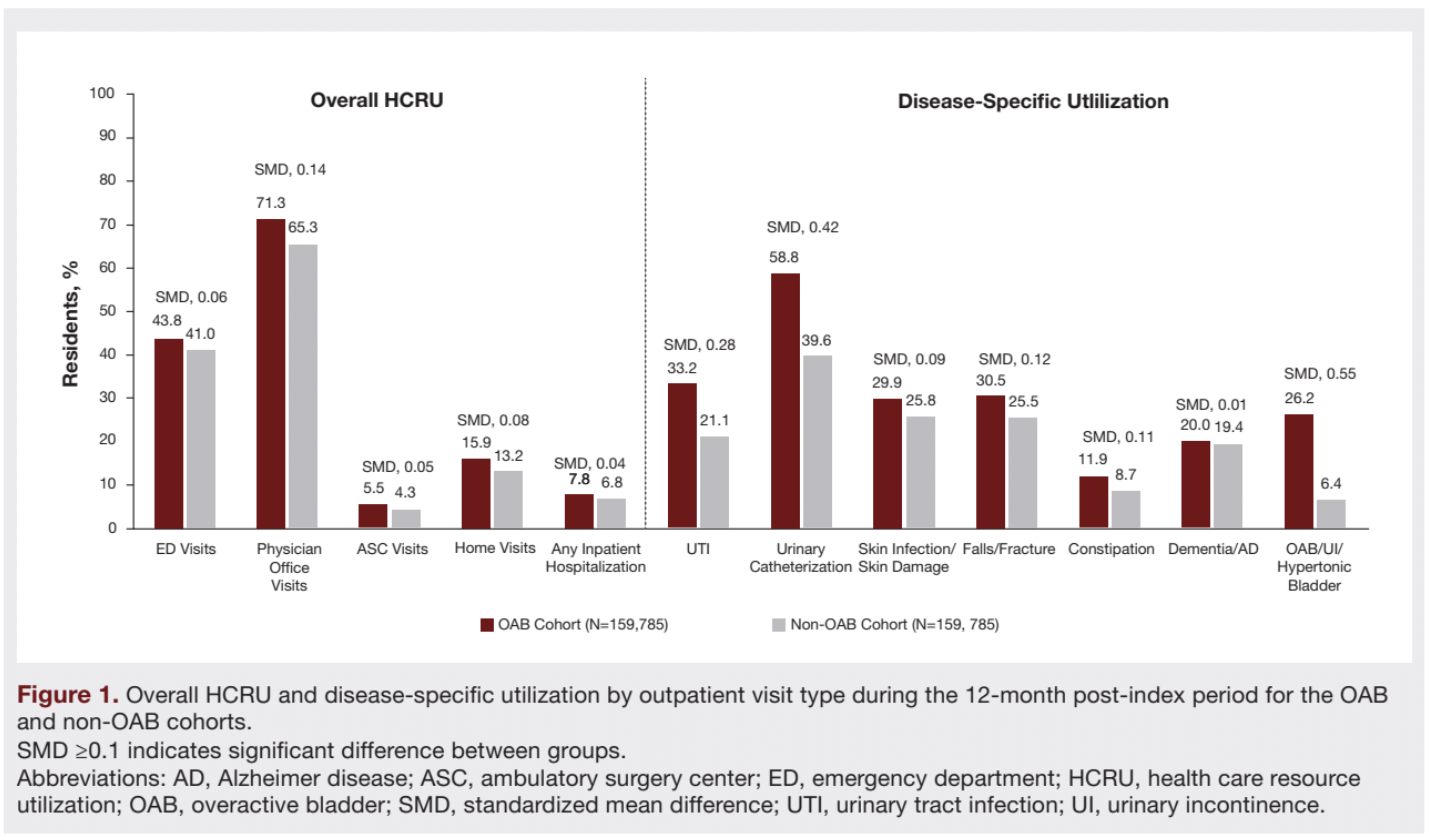
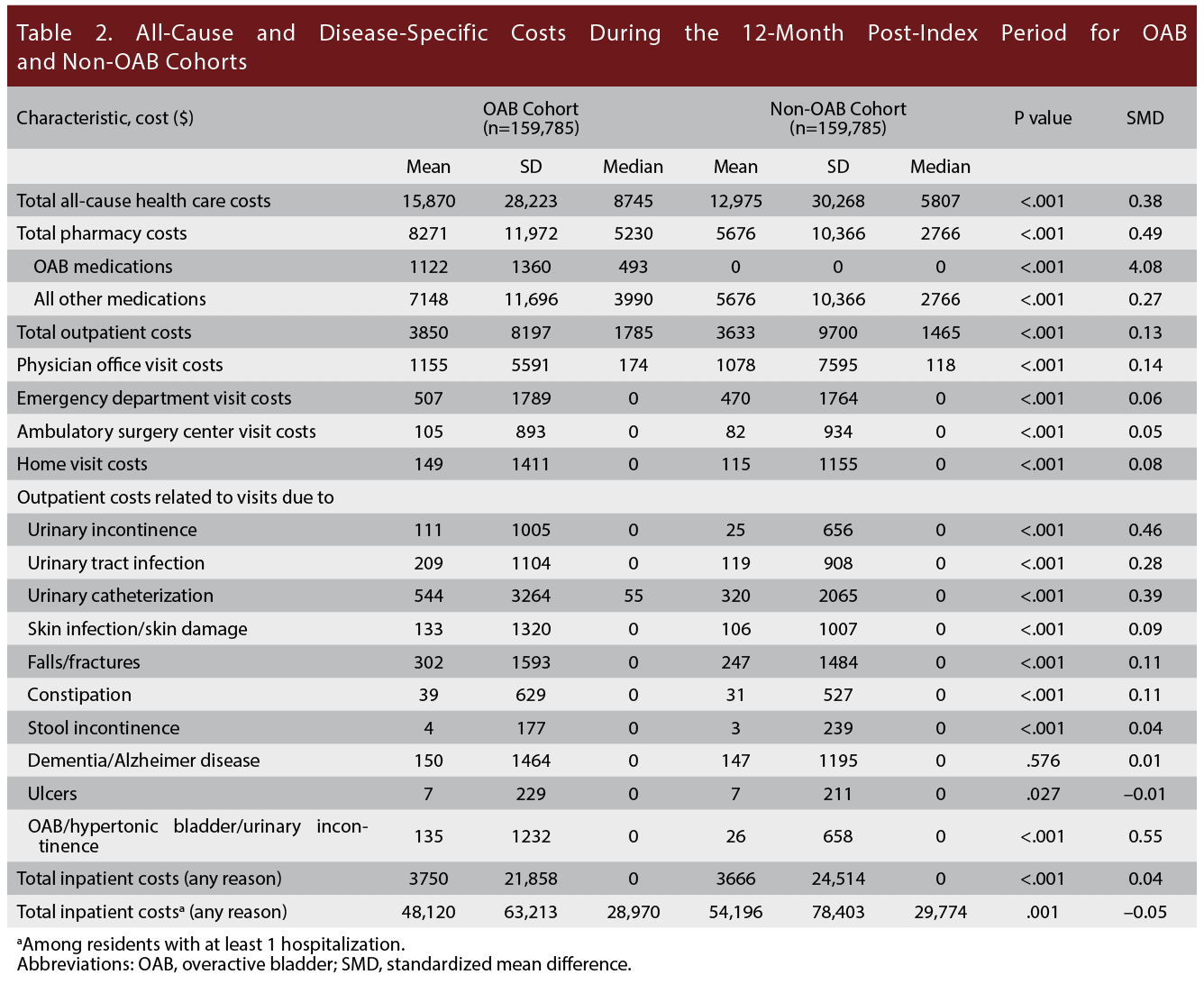
Consistent with higher HCRU, the OAB cohort had significantly higher costs than the non-OAB cohort during the 12-month post-index period (Table 2). Median total all-cause health care costs were $8745 in the OAB cohort vs $5807 in the non-OAB cohort (SMD, 0.38; P<.001); total pharmacy costs were $5230 vs $2766, respectively (SMD, 0.49; P<.001); and outpatient costs were $1785 vs $1465 (SMD, 0.13; P<.001). Specific costs related to the following conditions were also significantly higher for residents in the OAB cohort compared with the non-OAB cohort: fall/fractures, UTI, urinary catheterization, urinary incontinence, constipation, and OAB/hypertonic bladder/urinary incontinence (SMD range, 0.10-0.55; P<.001, each). The full list of costs is shown in Table 2.
After adjusting for demographic and clinical characteristics, the OAB cohort had 17% higher all-cause health care costs compared with the non-OAB cohort (95% CI, 15.4%-18.4%; P<.001; Table 3; Supplementary Table 2).
Treated vs Untreated Cohorts
A total of 52,569 diagnosed and pharmacologically treated and 217,929 diagnosed but not pharmacologically treated residents with OAB were identified. 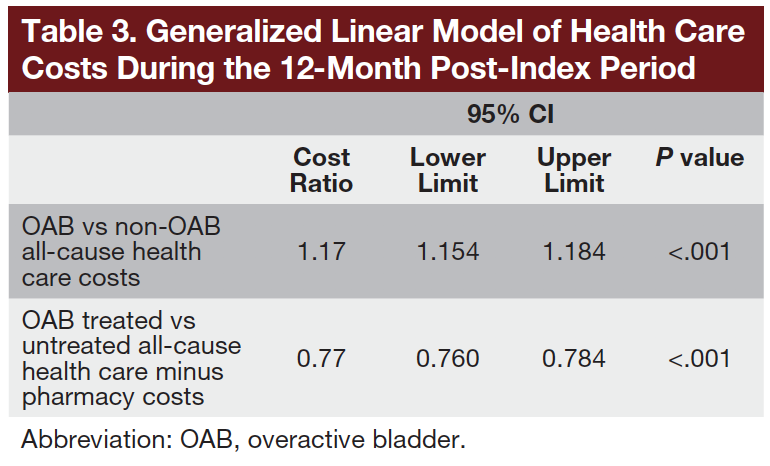 Baseline demographics for these residents are provided in Supplementary Table 3. Overall, residents in the treated vs untreated cohort were older (mean age, 74.4 vs 71.8 years, respectively), and most were female (70.1% vs 65.3%). The prevalence of most baseline comorbidities (eg, arthralgia, cerebrovascular disease, multiple sclerosis, stroke) and prescription claims for select medications of interest (eg, antidepressants, analgesics, antipsychotics, CYP2D6 substrates [QTc-related and sensitive substrates]) were higher in the treated vs untreated cohort (P<.001). In the treated cohort, 90.0% of residents receiving an OAB medication had a prescription claim for urinary anticholinergics (59.8% of whom received oxybutynin), and 17.0% had a prescription for mirabegron.
Baseline demographics for these residents are provided in Supplementary Table 3. Overall, residents in the treated vs untreated cohort were older (mean age, 74.4 vs 71.8 years, respectively), and most were female (70.1% vs 65.3%). The prevalence of most baseline comorbidities (eg, arthralgia, cerebrovascular disease, multiple sclerosis, stroke) and prescription claims for select medications of interest (eg, antidepressants, analgesics, antipsychotics, CYP2D6 substrates [QTc-related and sensitive substrates]) were higher in the treated vs untreated cohort (P<.001). In the treated cohort, 90.0% of residents receiving an OAB medication had a prescription claim for urinary anticholinergics (59.8% of whom received oxybutynin), and 17.0% had a prescription for mirabegron.
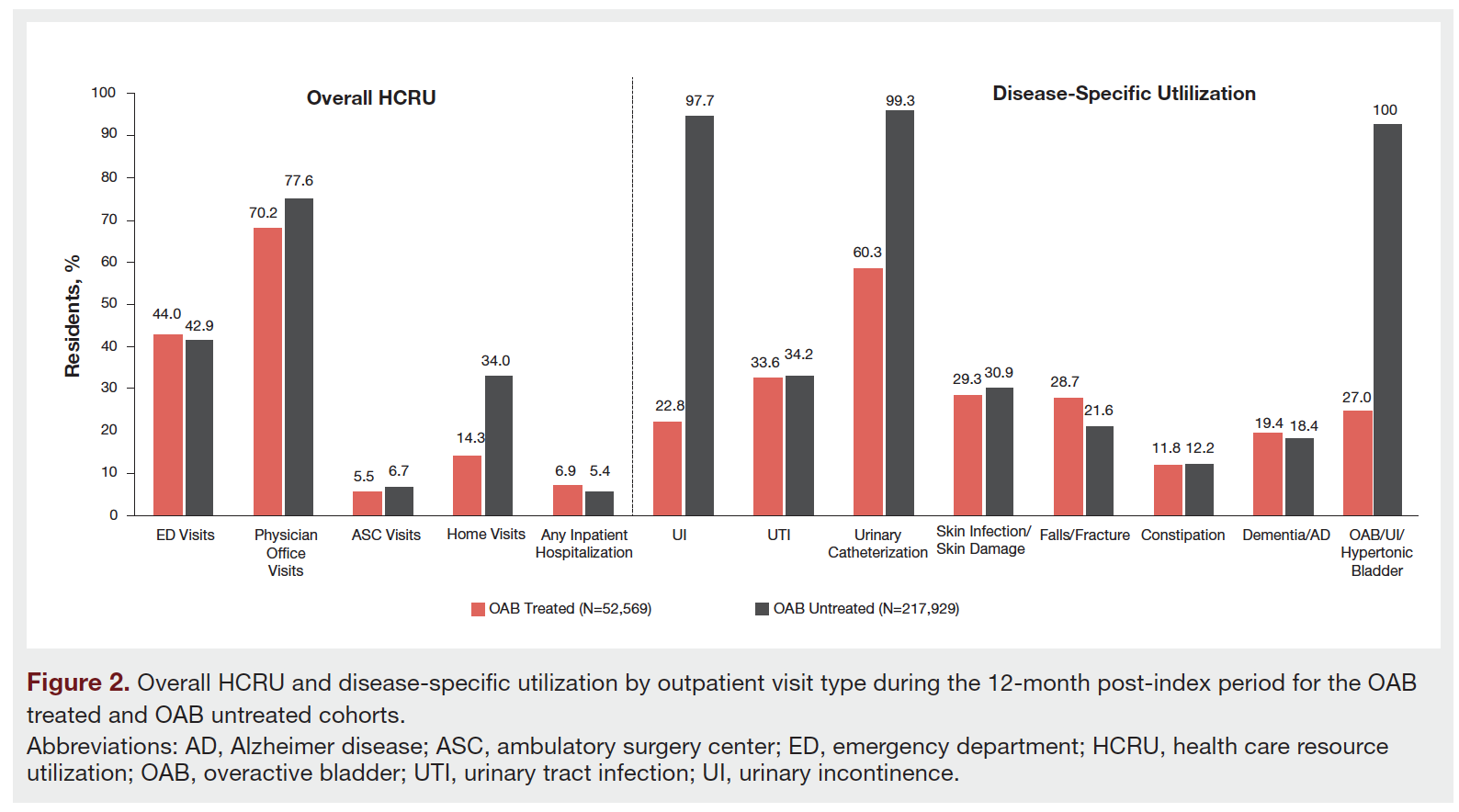
With respect to HCRU, a lower percentage of treated vs untreated residents had physician office visits due to urinary incontinence (22.8% vs 97.7%, respectively), urinary catheterization (60.3% vs 99.3%), and stool incontinence (1.0% vs 4.7%) during the 12-month post-index period (Figure 2).
Median total outpatient costs were significantly lower for treated vs untreated residents ($1760 vs $2571; P<.001; Supplementary Table 4). Adjusted analyses showed that OAB treated residents incurred 23% lower all-cause health care costs minus pharmacy costs than OAB untreated residents during the 12-month post-index period (95% CI, 21.6%-24.0%; P<.001; Table 3; Supplementary Table 5). Significant differences were observed between the OAB treated and OAB untreated cohorts for several components of total outpatient costs, including costs related to urinary incontinence, urinary catheterization, and OAB/hypertonic bladder/urinary incontinence (P<.001, each;Supplementary Table 4).
Discussion
OAB vs Non-OAB Cohorts
Patients with OAB experience high levels of functional impairment and physical limitations, comorbidities, and concomitant medication use.7 In this study, residents with OAB in the LTC setting were found to have higher HCRU and 17% higher all-cause costs compared with non-OAB matched LTC residents. Our results are generally consistent with those from other studies, which have also demonstrated greater health care costs for patients with vs without OAB.16-18 A systematic review and meta-analysis of studies examining total and OAB-specific costs reported ranges for annual total direct, pharmacy, and outpatient health care costs (in 2016 US dollars) of $8168-$15,569, $1182-$3900, and $1495-$6824, respectively.19 These ranges are generally in line with the average total costs ($15,870) and outpatient-related health care costs ($3850) reported for LTC residents with OAB in the present study. The results from our study extend those of previous studies by demonstrating increased HCRU and costs associated with residents with OAB in the LTC setting.
As anticipated in LTC with an older population, polypharmacy was common in the OAB cohort (median, 9 medications). Medications of interest in this study included those with anticholinergic effects, as these are associated with adverse neurologic effects, such as cognitive impairment and falls.20 In the OAB cohort, a higher proportion of residents received antidepressants, some of which have strong anticholinergic effects (eg, tricyclic antidepressants [TCAs], selective serotonin reuptake inhibitors [SSRIs; paroxetine, fluoxetine]), compared with the non-OAB cohort. In addition, many anticholinergics are CYP2D6 substrates and when used in combination with CYP2D6 inhibitors may lead to increased anticholinergic burden or safety and tolerability issues associated with anticholinergics, such as QT prolongation.21,22 Cardiovascular comorbidities such as hypertension are substantial in older adults with OAB.7 As a result, older adults with OAB and cardiovascular comorbidities receiving polypharmacy may be at increased risk for clinically significant drug-drug interactions and adverse effects.22 In this study, a significantly higher proportion of residents in the OAB cohort had prescriptions for medications that are CYP2D6 substrates compared with the non-OAB cohort (74% vs 67%, respectively). Increased polypharmacy reflected in the high proportion of residents receiving CYP2D6 substrates increases the likelihood of greater anticholinergic burden and associated adverse effects in residents with OAB. Furthermore, a significantly higher proportion of residents in the OAB cohort had outpatient visits related to falls/fractures compared with the non-OAB cohort during the 12-month post-index period.
Compared with residents without OAB, residents in the OAB cohort had a higher prevalence of comorbid conditions of interest such as multiple sclerosis and osteoarthritis; however, the true proportion of residents with comorbid multiple sclerosis may be artificially inflated owing to OAB medications used to treat neurogenic bladder. Comorbid conditions such as osteoarthritis may predispose residents with OAB to falls and subsequent fracture, as lower-extremity osteoarthritis has been shown to increase risk of falls, independent of age and sex.23 The increased use of antidepressants and analgesics further highlights increased levels of depression and clinical burden in patients with OAB. Patients with OAB report higher levels of depression compared with age-matched controls, with greater OAB symptom burden being positively correlated with severity of depression symptoms.24 Other studies have identified associations between OAB and pain disorders such as arthritis and neurologic comorbidities.25 The findings of greater health care utilization, costs, and disease burden in residents with OAB further underscores the importance of appropriate and timely diagnosis of OAB.
Treated vs Untreated Cohorts
Overall, all-cause health care costs minus pharmacy costs were 23% lower for residents who were pharmacologically treated for OAB compared with those who were untreated. HCRU was also generally lower for treated vs untreated residents. During the 12-month post-index period, fewer residents in the OAB treated cohort had outpatient visits related to urinary incontinence or catheterization compared with those in the OAB-untreated cohort. Residents who were treated for OAB tended to be older and had greater use of medications such as antidepressants and analgesics than those who were not treated, which is consistent with comorbidities reported for patients with OAB in previous studies.7,16
Although behavioral treatment may be sufficient in some patient populations, it may not be able to address all aspects of OAB symptoms. AUA guidelines recommend behavioral management in combination with pharmacologic treatment as first-line treatment.26 However, some medications used for the treatment of common OAB comorbidities have anticholinergic properties and are CYP2D6 substrates (eg, TCAs, SSRIs).27-29 These treatments are sometimes used with OAB treatments that are CYP2D6 inhibitors (eg, mirabegron, darifenacin),28,30,31 so any potential benefits of using anticholinergics to treat OAB must be weighed against the significant risk of common anticholinergic side effects and potential for drug-drug interactions in residents receiving polypharmacy. Among treated residents in our analysis, 90% had prescription claims for urinary anticholinergics, with ~60% of residents receiving a prescription for oxybutynin. A significantly higher proportion of treated residents had outpatient visits for falls/fractures (29%) compared with the OAB-untreated cohort (22%), which may be associated in part with increased anticholinergic burden. In adults with OAB receiving pharmacologic treatment, anticholinergic medications and subsequent increased anticholinergic burden has been shown to contribute to increased risk of falls.12-14 Patients with OAB also commonly have comorbidities that increase fall risk, and OAB itself may contribute to an increased risk of falling.25,32
Given the high prevalence of OAB in the LTC setting and associated economic burden,3 the results reported here may be an important factor for residents and payers when considering cost and making risk-benefit decisions involving OAB treatment. Prior studies have demonstrated that intervention in older patients with OAB improves quality of life.33 This study highlights the differences in burden with respect to HCRU and costs in treated vs untreated residents with OAB and suggests that physicians in LTC settings should investigate opportunities for OAB treatments with their residents. The physician’s role in educating staff and residents about OAB and potential treatment strategies is therefore of great importance, especially in older patient populations. Additionally, consultant pharmacists may be well positioned to mitigate the potential for drug interactions and adverse events.
Limitations
This analysis used a large data set of residents with OAB and a matched non-OAB cohort to identify characteristics, health care utilization, and cost patterns uniquely associated with OAB. Limitations of this analysis include those common to retrospective database studies, such as the reliance on reported and often incomplete data. The population of residents in LTC facilities may also bias the results as these residents have increased comorbidities and polypharmacy, which often leads to high caregiver burden and may partially explain increased HCRU and costs in the OAB cohort. However, the regression model used to analyze differences between cohorts accounted for variances in comorbidities. It is unknown to what extent residents with OAB who were not receiving prescription medications as treatment for OAB were receiving or following behavioral or dietary modifications, which are among the recommended first-line interventions for OAB.10 Use of OAB medication as a primary identifier allowed for inclusion of residents without a formal diagnosis claim who likely would not have been included in standard database analyses, although a prescription claim does not guarantee that the patient took the medication. Additionally, the claims database does not provide visibility into use of over-the-counter medications. Lastly, while our model for the treated and untreated cohorts accounted for relevant variables of interest, additional confounds that were unaccounted for may have biased results.
Conclusion
This study demonstrates that OAB is associated with significant health care utilization and financial burden in the US LTC setting. Residents with OAB had significantly higher HCRU and 17% higher all-cause health care costs compared with matched residents without OAB during a 12-month period.
A significantly lower proportion of residents with OAB who were pharmacologically treated had outpatient visits related to urinary conditions during the 12-month period vs pharmacologically untreated residents. Treatment of OAB was associated with 23% lower all-cause health care costs minus pharmacy costs. These results highlight the need for better management of OAB with respect to OAB treatment in the LTC setting.
Supplementary Materials can be viewed in the PDF version of this article.
Acknowledgements
Authors: Richard G Stefanacci, DO1; Jason Yeaw, MPH2; Drishti Shah, PhD2; Amy Kincaid, MA3;Paul N Mudd Jr, PharmD, MBA3
Affiliations: 1Jefferson College of Population Health, Thomas Jefferson University, Philadelphia, PA
2IQVIA, Falls Church, VA
3Urovant Sciences, Irvine, CA
Correspondence: Richard Stefanacci, DO
Jefferson College of Population Health
Thomas Jefferson University
901 Walnut Street, 10th Floor
Philadelphia, PA 19107
Email: richard.stefanacci@jefferson.edu
Disclosures: Portions of this research were presented as a poster at the 2020 International Society for Pharmacoeconomics and Outcomes Research (ISPOR) virtual meeting; May 18-20, 2020. Funding for this study was provided by Urovant Sciences. Urovant Sciences participated in study design, interpretation of data, and manuscript writing; reviewed the manuscript for accuracy; and provided approval for submission. The authors retained direction on the manuscript content. IQVIA received funding from the study sponsor to conduct this study. Medical writing and editorial assistance were provided by The Curry Rockefeller Group, LLC (Tarrytown, NY), and funded by Urovant Sciences. RGS is an advisor to Urovant Sciences. JY and DS are employees of IQVIA, which received funding for this study from Urovant Sciences. AK and PNM are employees of Urovant Sciences.
References
1. Coyne KS, Sexton CC, Vats V, Thompson C, Kopp ZS, Milsom I. National community prevalence of overactive bladder in the United States stratified by sex and age. Urology. 2011;77(5):1081-1087. doi:10.1016/j.urology.2010.08.039
2. Coyne KS, Payne C, Bhattacharyya SK, et al. The impact of urinary urgency and frequency on health-related quality of life in overactive bladder: results from a national community survey. Value Health. 2004;7(4):455-463. doi:10.1111/j.1524-4733.2004.74008.x
3. Gorina Y, Schappert S, Bercovitz A, Elgaddal N, Kramarow E. Prevalence of incontinence among older Americans. Vital Health Stat 3. 2014;(36):1-33.
4. Newman DK. Urinary incontinence in long-term care facilities: current clinical practice. Director. 2004;12(1):30-33.
5. Carvalho N, Fustinoni S, Abolhassani N, Blanco JM, Meylan L, Santos-Eggimann B. Impact of urine and mixed incontinence on long-term care preference: a vignette-survey study of community-dwelling older adults. BMC Geriatr. 2020;20(1):69. doi:10.1186/s12877-020-1439-x
6. Maxwell CJ, Soo A, Hogan DB, et al. Predictors of nursing home placement from assisted living settings in Canada. Can J Aging. 2013;32(4):333-348. doi:10.1017/S0714980813000469
7. Ganz ML, Liu J, Zou KH, Bhagnani T, Luo X. Real-world characteristics of elderly patients with overactive bladder in the United States. Curr Med Res Opin. 2016;32(12):1997-2005. doi:10.1080/03007995.2016.1226167
8. Sura S, Shiozawa A, Ng D, Aparasu RR. Higher resource utilization and costs in long-term nursing home residents with overactive bladder: a retrospective study of medicare beneficiaries. J Am Med Dir Assoc. 2020;S1525-8610(20)30743-X. doi:10.1016/j.jamda.2020.08.037
9. Murray B, Hessami SH, Gultyaev D, et al. Cost-effectiveness of overactive bladder treatments: from the US payer perspective. J Comp Eff Res. 2019;8(1):61-71. doi:10.2217/cer-2018-0079
10. Lightner DJ, Gomelsky A, Souter L, Vasavada SP. Diagnosis and treatment of overactive bladder (non-neurogenic) in adults: AUA/SUFU guideline amendment 2019. J Urol. 2019;202(3):558-563. doi:10.1097/ju.0000000000000309
11. American Geriatrics Society Beers Criteria Update Expert Panel. American Geriatrics Society 2019 Updated AGS Beers Criteria® for potentially inappropriate medication use in older adults. J Am Geriatr
Soc. 2019;67(4):674-694. doi:10.1111/jgs.15767
12. Szabo SM, Gooch K, Schermer C, et al. Association between cumulative anticholinergic burden and falls and fractures in patients with overactive bladder: US-based retrospective cohort study. BMJ
Open. 2019;9(5):e026391. doi:10.1136/bmjopen-2018-026391
13. Marcum ZA, Wirtz HS, Pettinger M, et al. Anticholinergic medication use and falls in postmenopausal women: findings from the Women’s Health Initiative Cohort study. BMC Geratr. 2016;16:76. doi:10.1186/s12877-016-0251-0
14. Green AR, Reifler LM, Bayliss EA, Weffald LA, Boyd CM. Drugs contributing to anticholinergic burden and risk of fall or fall-related injury among older adults with mild cognitive impairment, dementia and multiple chronic conditions: a retrospective cohort study. Drugs Aging. 2019;36(3):289-297. doi:10.1007/s40266-018-00630-z
15. Zarowitz BJ, Allen C, O’Shea T, Tangalos EG, Berner T, Ouslander JG. Challenges in the pharmacological management of nursing home residents with overactive bladder or urinary incontinence. J Am Geriatr Soc. 2015;63(11):2298-2307. doi:10.1111/jgs.13713
16. Darkow T, Fontes CL, Williamson TE. Costs associated with the management of overactive bladder and related comorbidities. Pharmacotherapy. 2005;25(4):511-519. doi:10.1592/phco.25.4.511.61033
17. Durden E, Walker D, Gray S, Fowler R, Juneau P, Gooch K. The economic burden of overactive bladder (OAB) and its effects on the costs associated with other chronic, age-related comorbidities in the United States. Neurourol Urodyn. 2018;37(5):1641-1649. doi:10.1002/nau.23513
18. Durden E, Walker D, Gray S, Fowler R, Juneau P, Gooch K. The direct and indirect costs associated with overactive bladder within a commercially-insured population in the United States. J Occup Environ Med. 2018;60(9):847-852. doi:10.1097/jom.0000000000001367
19. Powell LC, Szabo SM, Walker D, Gooch K. The economic burden of overactive bladder in the United States: a systematic literature review. Neurourol Urodyn. 2018;37(4):1241-1249. doi:10.1002/nau.23477
20. Ruxton K, Woodman RJ, Mangoni AA. Drugs with anticholinergic effects and cognitive impairment, falls and all-cause mortality in older adults: a systematic review and meta-analysis. Br J Clin Pharmacol. 2015;80(2):209-220. doi:10.1111/bcp.12617
21. Arana A, Margulis AV, McQuay LJ, et al. Variation in cardiovascular risk related to individual antimuscarinic drugs used to treat overactive bladder: a UK cohort study. Pharmacotherapy. 2018;38(6):628-637. doi:10.1002/phar.2121
22. Rutman MP, Horn JR, Newman DK, Stefanacci RG. Overactive bladder prescribing considerations: the role of polypharmacy, anticholinergic burden, and CYP2D6 drug‒drug interactions. Clin
Drug Investig. 2021;41(4):293-302. doi:10.1007/s40261-021-01020-x
23. Doré AL, Golightly YM, Mercer VS, et al. Lower-extremity osteoarthritis and the risk of falls in a community-based longitudinal study of adults with and without osteoarthritis. Arthritis Care Res. 2015;67(5):633-639. doi:10.1002/acr.22499
24. Lai HH, Shen B, Rawal A, Vetter J. The relationship between depression and overactive bladder/urinary incontinence symptoms in the clinical OAB population. BMC Urol. 2016;16(1):60. doi:10.1186/s12894-016-0179-x
25. Tannenbaum C, Gray M, Hoffstetter S, Cardozo L. Comorbidities associated with bladder dysfunction.
Int J Clin Pract. 2013;67(2):105-113. doi:10.1111/ijcp.12085
26. Diagnosis and Treatment of Overactive Bladder (Non-Neurogenic) in Adults: AUA/SUFU Guideline (2019). American Urological Association. Accessed January 28, 2021. https://www.auanet.org/guidelines/guidelines/overactive-bladder-(oab)-guideline
27. Dahlinger D, Aslan S, Pietsch M, Frechen S, Fuhr U. Assessment of inhibitory effects on major human cytochrome P450 enzymes by spasmolytics used in the treatment of overactive bladder syndrome. Ther Adv Urol. 2017;9(7):163-177. doi:10.1177/1756287217708951
28. Enablex (darifenacin). Prescribing information. Novartis Pharma Stein AG; 2008.
29. Detrol (tolterodine tartrate). Prescribing information. Pfizer; 2012.
30. Takusagawa S, Miyashita A, Iwatsubo T, et al. In vitro inhibition and induction of human cytochrome P450 enzymes by mirabegron, a potent and selective beta3-adrenoceptor agonist. Xenobiotica. 2012;42(12):1187-1196. doi:10.3109/00498254.2012.700140
31. Myrbetriq (mirabegron extended-release tablets). Prescribing information. Astellas Pharma US, Inc; 2018.
32. Marcum ZA, Perera S, Thorpe JM, et al. Anticholinergic use and recurrent falls in community-dwelling older adults: findings from the Health ABC Study. Ann Pharmacother. 2015;49(11):1214-1221. doi:10.1177/1060028015596998
33. Kraus SR, Bavendam T, Brake T, Griebling TL. Vulnerable elderly patients and overactive bladder syndrome. Drugs Aging. 2010;27(9):697-713. doi:10.2165/11539020-000000000-00000



