

Beyond Adherence: Clinical Pathways at Roswell Park
Founded by Mishellene McKinney, MHA, RN, OCN, in 2016, the Clinical Pathways Forum is a community of pathways professionals–now totaling over 12 institutions from across the US–who are utilizing clinical pathways in their practices and institutions to improve cancer care.
The Journal organizes quarterly conference calls with Forum members to facilitate discussion of shared experiences and lessons learned regarding pathway use as clinical pathways become more prevalent and evolve to meet the needs of value-based health care systems and reimbursement models.
Highlights from each of the Forum conference calls that occur throughout the year are published in the Journal of Clinical Pathways (JCP). This third installment for 2023 summarizes the speakers and discussion from the August 2023 call. Health care professionals from across the continuum of care are encouraged to join in these collaborative discussions
Opportunities for Prospective Pathway Use
On August 15, 2023, Stephen B. Edge, MD, vice president of System Quality and Outcomes, Roswell Park Comprehensive Cancer Center, addressed the Clinical Pathways Forum with an update on the clinical pathways program at Roswell Park (RP). Dr Edge is also the medical director of the Clinical Oncology Pathways program at RP, professor of oncology, and a breast surgeon. He is on the National Comprehensive Cancer Network (NCCN) Board of Directors, and the Executive Committee of the American Joint Committee on Cancer (AJCC). He is a past member of the American Society of Clinical Oncology (ASCO) Board of Directors, past chair of the Commission on Cancer, and past editor in chief of the AJCC Cancer Staging Manual. He also served on the ASCO Clinical Pathways Taskforce.
I (Mishellene McKinney, MHA, RN, OCN) also addressed the Clinical Pathways Forum to inform the group that after 7 years of organizing and moderating the panel, this will be my last Forum session. The Forum is being transferred to the competent hands of Nicole DeGennaro, associate editorial director for JCP. Many thanks to the members of the Forum for your collegiality and to the JCP team for your ongoing support over the years.
The Clinical Pathways Program at Roswell Park
RP is a National Cancer Institute (NCI) cancer center located in Buffalo, New York, and it is the only NCI center in western New York. The center has a dedicated pathways department that was established in 2015, consisting of two leaders overseeing pathway development and operations and analytics, a pathways coordinator, a data analyst, and a nurse quality coordinator. The team is responsible for operations and oversight of drug treatment pathways and quality oversight across the Roswell Park Care Network, which spans western New York from Buffalo to Albany, and south to the Pennsylvania border. The Pathways Department is responsible for annual affiliate quality reviews, Quality Oncology Practice Initiative (QOPI) certification support, and case reviews if there are patient complaints regarding quality of care. They run a quality council across the network and are in the process of establishing a patient family advisory group across the network.
Compelling Reasons for Pathway Use at Roswell Park
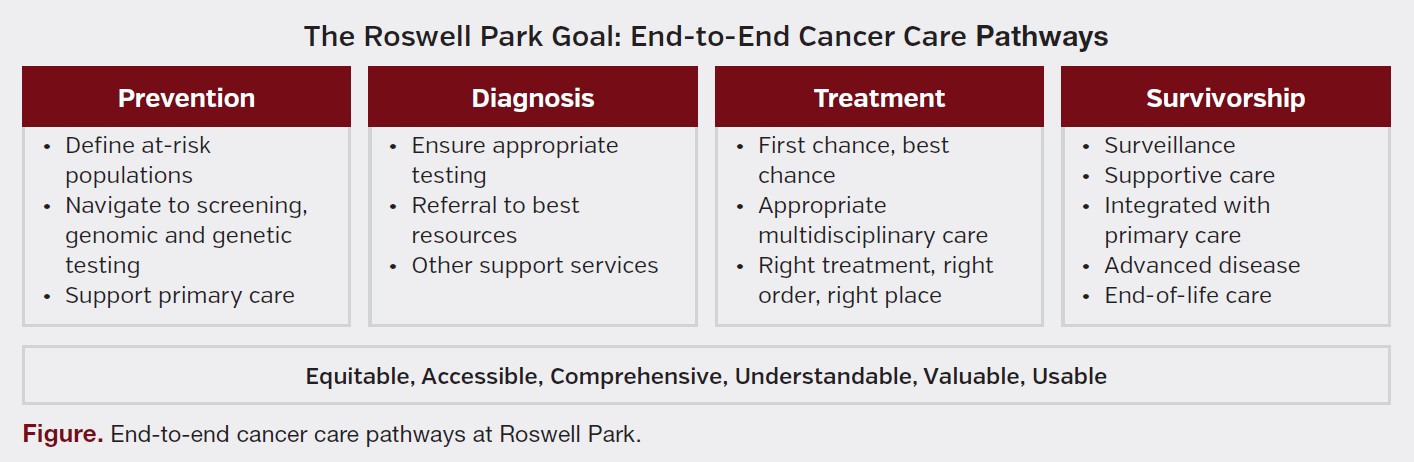
As previously reported to the Forum in 2021, clinical pathways at RP are used to document quality of care for every location in the network, present clinical trials at the point of care for all patients, and serve as a cornerstone for education and treatment planning (Figure). Additionally, RP uses pathways data to inform and coordinate care. For example, providers identify individuals with advanced cancer and promote goals of care (GOC) and the use of hospice care to these patients. Finally, through pathways RP provides information to payers regarding its quality of care, including benchmarks, preauthorization documents, and rationale for off-pathway therapy treatment decisions. Dr Edge stated, “If we are going to put our name on a practice, we want to know what the quality of care is.”
Pathways Endorsed by Medical Societies
Pathways have become a standard tool for quality in oncology. Many large systems have implemented them since The US Oncology Network and their Chief Medical Officer Marcus Neubauer, MD, first started promoting their use in 2005. Pathways are required by national payers, and recently ASCO and the Community Oncology Associates Oncology Medical Home (OMH) have endorsed the use of pathways in their standards, stating, “The OMH practice uses value- and evidence-based treatment and supportive care pathways, measures and reports on physician compliance with pathways, and requires documentation for off-pathway treatment.”
Scope of Pathways
Because of variation in care and the rapidly escalating costs in drug therapy for cancer, pathways were developed to standardize care and, consequently, reduce cost of care. Oncology pathways in the US primarily address the decisions surrounding systemic drug therapy. They are not comprehensive, end-to-end pathways. Dr Edge questions this approach, stating, “I’m actually skeptical that pathways actually do reduce cost of care, and I think the papers that say that we do really are comparing apples and oranges because the people who are treated off pathway are simply different than the people who are treated on pathway. There’s been limited attention [paid] to comprehensive pathways, but I think that’s where we need to be moving.”
How Adherence Findings Are Used Across the Network
RP has a network of affiliated practices, and the pathways are used across the entire network. RP owns several medical oncology practices in the Buffalo area. They also have affiliations with hospitals across the state, including in Niagara Falls, which is a historically underserved community, and in small, rural communities across the state, including Jamestown, Watertown, Ithaca, and Oneida. RP also has affiliates in the Capital District near Albany and an affiliation with a four-hospital system in Long Island.
RP uses the ClinicalPath pathways program by Elsevier for their pathways. Their objective is to include the pathway with each patient interaction to guide treatment selection. ClinicalPath is integrated into AllScripts, the electronic health record (EHR) system, for scheduling, and treatment selection is directly linked to order sets. A note summarizing the pathway selection is uploaded into the EHR, and this summary can be imported into the treatment note.
Dr Edge emphasized that all care should not be expected to be on pathway and that there are many patient factors to consider. He stated, “I think this is all very arbitrary, saying that 75, 85, or 90 percent of patients should be on pathways. There’s no data to support that the quality of care is better with some arbitrary rate of adherence. I like to say that 100 percent of patients should get appropriate care, but the rate may vary based on cancer type status, status of the patient, whether this is adjuvant therapy, or they have advanced disease.” Because of this philosophy, Dr Edge believes that off-pathway review is one of “the most important things about the pathways program at Roswell Park.”
The pathways team at RP performs an adjudication of off-pathway treatments to evaluate the reasons for off-pathway care. This adjudication service does not delay care or result in an increase in physician work. The findings are used for feedback to providers and payers for value-based quality payments. Dr Edge explained that he has spent a considerable amount of time with payers to convince them that off-pathway care is usually the right care.
He referred to a paper that RP presented at ASCO in 2019, which stated that RP had an 85% rate of on-pathway care. The on-pathway rate for people receiving adjuvant therapy was higher, and not surprisingly, for people who had metastatic disease it was somewhat lower. He explained that is to be expected. More importantly, the study team looked at the reasons for the off-pathway care and demonstrated that the vast majority were for appropriate reasons. He stated, “This is why I don’t think that cost is really something we’ll control. Certainly, you may standardize care with pathways, but we found that most of the patients are getting the pathway recommended care anyway. So off pathway here is usually the appropriate care. In fact, I think that the financial incentives which are offered by some payers right now for being on pathway may paradoxically result in lower than optimal care.”
Beyond Adherence
Dr Edge then turned the discussion to clinical pathway use beyond treatment and provided examples of ancillary use cases at RP. These included supporting research studies, increasing patient engagement, allowing more detailed evaluation of practice patterns, allowing quick care coordination, and providing assurance of multidisciplinary care.
Clinical Trial Enrollment and Equity in Trial Enrollment
Clinicals trials are embedded into the pathways at RP and are presented to the initial outpatient provider to increase awareness and accrual and improve institutional trial management. ClinicalPath provides a Bypass Report that shows all active trials that are presented as a “hard stop,” meaning that the provider must make a selection related to the trial to either continue with selecting the trial or give a simple reason for why they did not select the trial. RP can then identify the number of people who meet the basic eligibility criteria for each trial, which assists the team with internal auditing of clinical trials and identifying trials for retention to community sites.
For example, the COMPASSHER2 trial has 27 patients that are eligible and RP might want to open it—if feasible—at a community site. In contrast, RP would not want to open at their community sites a trial that only has 3 eligible patients because “the gain is not worth the run.” RP recently extracted the race ethnicity information from demographic information at the hospital and linked it to the Bypass Report. Clinical Research Services are now examining this data to see whether there are variations in the offering of clinical trials based on race and ethnicity to better understand minority trial enrollment.
Pathways data is also used to rapidly identify the number of people with certain eligibility criteria to support trial openings and grant submissions. This information, which includes demographics, can be provided in minutes to investigators. “I would challenge people that don’t have pathways data to have the ability to do that. Our electronic medical records (EMRs) simply do not provide the ability to get down to this level that quickly,” said Dr Edge.
Patient Education
Pathways are a key element in patient education at RP. A graphic posted in exam rooms states that pathways are used at the center and that they provide doctor expertise, the best standards, clinical trial options, and address patient needs to provide the best care possible. The sign encourages patients to ask questions about their treatment, clinical trials, and pathways.
Palliative Care
Pathways are used to prompt and direct palliative care at RP. The “surprise” question, “Would you be surprised if the patient were to die in the next year?”, has been helpful in identifying patients that would benefit from palliative care. RP also checks the EMR for a documented GOC question for patients who have a metastatic treatment decision in the pathway. Then, they match this information to the physician schedule and send out a prompt if the GOC discussion has not been documented.
When this check was implemented, RP wanted to see an increase in documentation of GOC. This process, known as the “nudge” concept, is something that RP continues to work on in collaboration with others, including Dr Finly Zachariah at City of Hope, who has created a validated tool that more accurately predicts short-term survival. The Association of Dedicated Cancer Centers are working to study the value of these nudges across the network.
RP also uses pathways to identify patients for more advanced therapies, both at the main campus and across the network. Because clinical trials are built into the pathways as a mechanism to recruit from all sites, they can also be used to identify patients at a potentially earlier line of therapy. For example, if there is a chimeric antigen receptor T-cell product that needs to be applied relatively early for a patient or if the patient has refractory diffuse large B-cell lymphoma or a relapse, RP can scan the pathways and know the treatment recommendation within a few days. If it’s the first treatment recommendation, the pathways team will follow up after a repeat PET in about 3 months, and if there hasn’t been a documented discussion with the patient, the team will contact the doctor to ensure they are aware of the treatment opportunity.
Understanding and Monitoring the Practice
Over an 18-month period, RP investigated whether patients with pancreas cancer were receiving appropriate multidisciplinary care across the network. They reviewed pathways decisions for patients with borderline resectable, resectable, and unresectable pancreas cancer. They also checked whether a surgeon reviewed each case to determine whether the cancer was potentially resectable. RP were pleased to find that of the 23 patients that had pancreas cancer, all 23 had seen the surgical specialist prior to starting chemotherapy. RP presented 19 of the 23 cases at the multidisciplinary conference.
Additional use cases that are under development include developing a tracking program with patient-reported outcomes linked to pathway data, establishing pathways for symptom management, prospective review of multidisciplinary care, and patient engagement with a network-wide patient family advisory council. RP has not found an example of a system-wide, network-wide patient family engagement council that includes the community network. Dr Edge requested that if anyone on the call knows of such a program to please reach out to him or his team.
In closing, Dr Edge cited an article that was recently published in JAMA titled, “Preparing physicians for the clinical algorithm era.” “Isn’t that what we have been doing for the past several years with pathways?” he queried. He posited that algorithms for pathway care are going to have to go beyond the unidimensional systemic treatment therapy and into screening, population health and survivorship, and ensuring access to equitable care. In conclusion, he stated that we are “only scratching the surface of the value of pathways data.”



