


Off-Label Use of Precision Oncology Therapeutics in Advanced Solid Cancers Following Identification of Associated Variants via Multicancer Next-Generation Sequencing Panel: A Real-World Evidence Pilot Study
Abstract
Background: Off-label use of pharmaceuticals, including in precision oncology, is common but not necessarily lacking in evidence of efficacy and safety. Concerns about payer coverage hindering comprehensive genomic profiling (CGP) in precision oncology are raised, yet studies show that CGP rarely leads to prescribing of off-label therapies (2%-7%). We investigated off-label therapy utilization post- CGP via liquid biopsy using a clinicogenomic database. Variants associated with US Food and Drug Administration (FDA)-approved therapies were identified in patients. Methods: We reviewed clinical reports for FDA-approved therapy-associated variants, focusing on five genes (EGFR, PIK3CA, ATM, BRCA1, BRCA2) with >1% frequency. We then used the GuardantINFORM database (137 000+ patients) to assess off-label use impact, including variants of uncertain significance (VUSs) influence. Results: Among variants with an associated FDA-approved therapy in another indication (n = 18 660), only 0.8% had subsequent off-label therapy claims unrelated to on-label cancer types. Clinical trial enrollment post-CGP in the group receiving off-label therapy was 19%. For VUSs in five genes, 1.2% received off-label therapies (n = 21 606). Conclusions: CGP via validated liquid biopsy seems to result in minimal inappropriate use of off-label therapies. These findings can inform payer coverage policies regarding CGP’s impact on advanced solid cancers.
Introduction
An off-label drug is used to treat a disease that is inconsistent with the prescribing information issued by the US Food and Drug Administration (FDA). These inconsistencies can include unapproved indication, varied population group, unapproved route of administration, or unapproved dosage. Despite lacking the endorsement of the FDA, off-label drug use remains a common clinical practice for pharmaceuticals ranging from over-the-counter analgesics to high-cost immunotherapies. However, off-label is not synonymous with a lack of evidence supporting efficacy and safety, and in oncology, off-label utilization may be included in best practice guidelines.1 While off-label drug use may be a known practice in oncology, US health plans have traditionally considered off-label drug use as a concerning practice, particularly in precision oncology for patients with advanced/metastatic solid tumors, where the genetic makeup of a tumor may guide expensive targeted treatments. Payers reported that multicancer next-generation sequencing (NGS) testing of an advanced solid tumor would report genomic variants for other cancer types, leading to off-label use of precision oncology therapy resulting in costs or harm.2 This is a key barrier to health plan coverage for such testing, despite lack of studies reporting such behavior following genetic testing.2
Insurance coverage and reimbursement policies play a significant role in managing the genetic testing that informs therapy in precision oncology, with the primary goals of cost containment and quality, effective care. Insurance coverage of FDA-approved therapeutics is relatively straightforward compared to the diverse coverage of the genetic testing that identified eligibility for a precision oncology therapy. Some insurers manage precision oncology therapies by requiring documentation of the FDA-approved biomarker identified by genetic testing to ensure on-label use.3 The Centers for Medicare & Medicaid Services (CMS) and private insurers typically reimburse drugs based on their FDA approval status or approved compendia. Compendia are created by drug assessment experts that compile off-label drug lists, based on reviewed evidence.4 In the era of precision medicine, several tools are useful to match the appropriate drug to each particular patient, and insurance coverage is varied. For patients with advanced/metastatic solid tumors (mostly stage IV disease), comprehensive genomic profiling (CGP) via NGS panels test many genes at once on tissue from the tumor itself and/ or via circulating tumor DNA (ctDNA) and is highly utilized by oncologists to complete guideline-recommended tumor genetic testing. Another tool in precision oncology is molecular tumor boards (MTBs), which provide expert review of tumor genetic results to interpret guideline-recommended genetic testing and guide treatment. While CGP via NGS is covered by CMS and many payers, some payer policy stakeholders limit coverage of NGS testing, pointing to off-label precision oncology drug use as a potential risk for clinical and financial harm arising from CGP to guide precision medicine, despite also acknowledging the benefit to patients and potential to transform care.2 Apart from payers, notable associations like the European Society for Medical Oncology (ESMO) cite cost concerns arising from off-label precision oncology drug use as a pitfall of multigene CGP panels via NGS.5 The potential for CGP to result in off-label drug use without clinical trial evidence of efficacy is also a concern and a challenge of applying traditional evidence frameworks to precision oncology.6
Mirroring the concerns above, off-label drug use in general oncology has been estimated to be as high as 70%.7 However, real-world evidence billing data from oncology practices demonstrates an average of 30% off-label use for common chemotherapies and 18%-30% for immunotherapies (which may be biomarker driven).7,8 In precision oncology, however, several studies of mixed methodologies show that off-label prescribing of precision oncology therapies (associated with a specific genetic variant[s]) based on CGP results is in reality quite minimal—as little as 2%-7%.9–13 Similarly, several other studies demonstrate that patients experience clinical benefit when receiving on-label matched therapies based on ctDNA results or are directed to clinical trials as supported by guidelines, suggesting the benefits outweigh the concern for off-label prescribing.14-16 In patients with advanced metastatic cancers with no further options, patients who have exhausted all the approved treatments, or patients in hospice, off-label drugs (those that share driving mutations/molecular signaling pathways) can be justified as “extended” compassionate care. Compassionate drug use (expanded access) refers to the prescribing of investigational therapies when patients suffer from chronic/deadly illness, with no possibility of availing approved treatments/ineligible for clinical trials.17 Harms to patients from genetic testing have made headlines in hereditary or germline cancer, where testing was used to guide surgery or treatment inappropriately, often due to physicians’ misinterpretation of test results.18,19 This legacy of harm in the hereditary cancer space, where oncologists are often faced with cancer prevention, has certainly been a concern applied—perhaps inappropriately—to tumor genetic testing, where oncologists are urgently looking for specific genetic changes to guide specific treatments in critically ill patients.
Despite the broad acceptance of multicancer NGS molecular profiling by oncologists and some payers such as CMS, perceptions of harm and concern over increased spending from off-label precision oncology therapies remain barriers to broad coverage of NGS testing by commercial payer medical policies. Existing literature and personal communication with payer representatives shaped the research question for the present study: What is the frequency of off-label use of precision oncology therapies among patients with associated variants and variants of uncertain significance (VUSs) identified via multicancer NGS molecular profiling? Therefore, the present study analyzes the observed frequency of real-world off-label precision oncology FDA-approved therapies following reporting of select variants and VUSs associated with these therapies via CGP (Guardant360 CDx and Guardant360) using a 55-74 or 83 gene NGS plasma-based tumor profiling multigene panel.
Methods
Ethics, Data Source, and Extraction
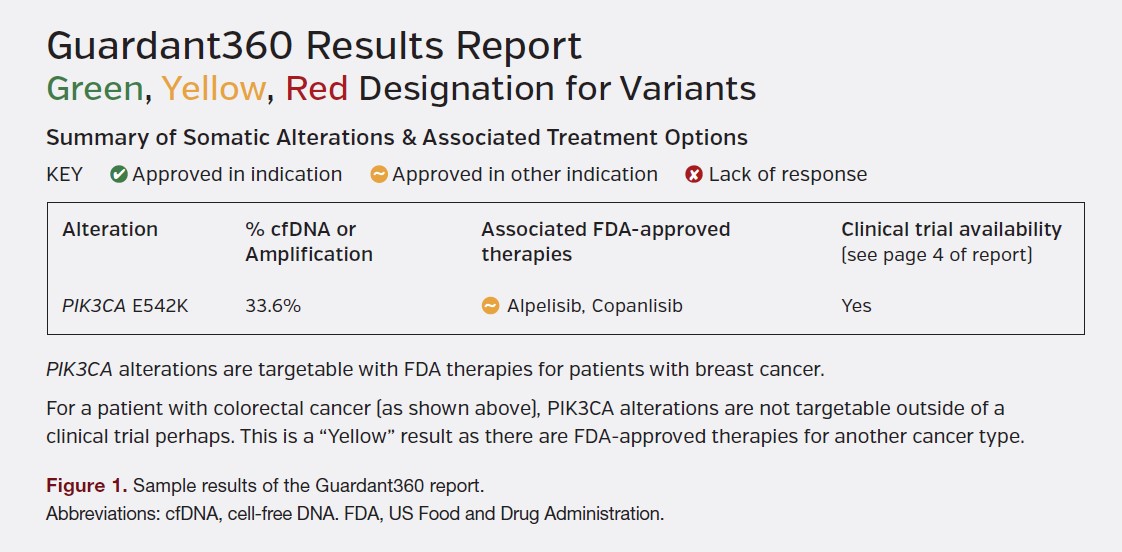
The ethics and GuardantINFORM database information was published by Nakamura et al in 2022.20 The database comprises deidentified genomic report data for the patients with advanced/metastatic solid cancers who were prescribed the Guardant360 (G360) test. Representatives from a national payer, regional payer, and lab benefit manager provided input as to what type of variants or reporting were most concerning for off-label therapy use. The variants most likely to lead to off-label therapy were thought to be those variants that are reported with an FDA-approved therapy annotation on the report, and secondarily any VUSs on the report (Supplementary Figure 1). The G360 test reports are designed with color annotations, and the variants of interest in this study fall in the category designated on reports as “yellow” (Figure 1).
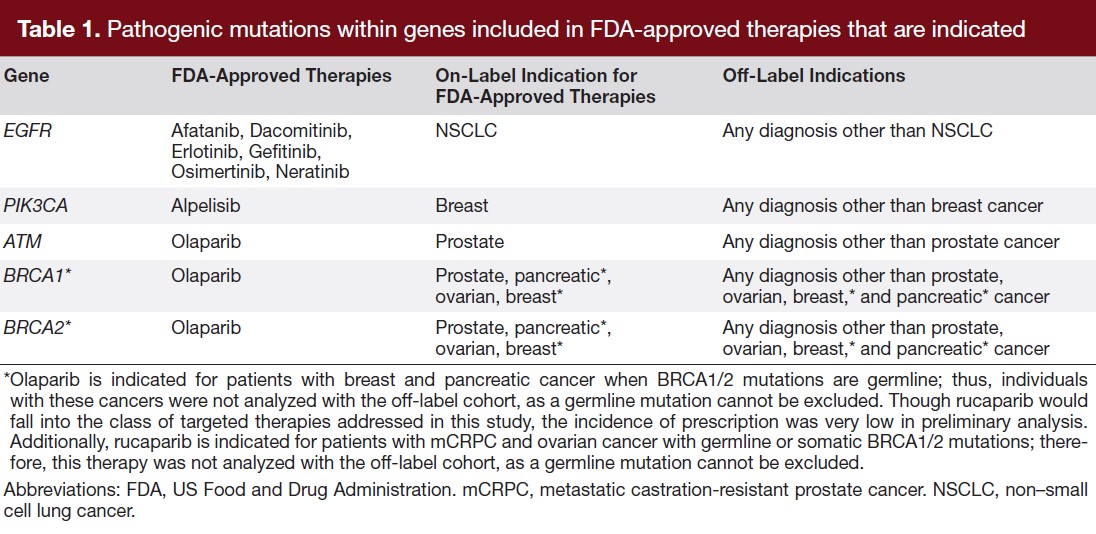
We used the reports to identify all “yellow” variants and then excluded those that occurred in less than 1% of all tested patients, which by virtue of low frequency may have skewed off-label use (eg, RET and ARID1A). Five genes (EGFR, PIK3CA, ATM, BRCA1, and BRCA2) were identified as having “yellow” variants for which there is an associated FDA-approved therapy for an indication other than the patient’s cancer diagnosis (Supplementary Table 1). These five genes and associated variants also have a multiyear history of FDA approval as precision oncology therapies. To further investigate the impact of VUSs, we analyzed all VUSs in the five genes studied. Neither a disease-causing variant nor a VUS in these genes would be on-label for an FDA-approved therapy (Supplementary Figure 2). During the study period, GuardantINFORM contained 137 490 US patients across 60 cancer types. Table 1 summarizes the off-label indications we addressed in this study.
Study Population
Patients (n = 18 660) harboring “yellow” variants of interest and patients (n = 21 606) harboring VUSs in EGFR, PIK3CA, ATM, BRCA1, or BRCA2 genes were then identified within GuardantINFORM. Then we evaluated patients who had claims available for off-label therapies as indicated in their G360 reports. Among the patients with the listed therapies and results, we identified patients who had on-label primary cancer diagnosis codes (ICD-9/10) from claims (Supplementary Table 1).
This on-label cohort (n = 74) was then characterized into multiple primaries or unknown/misaligned diagnosis by following individual patient diagnosis history. The remaining patients (n = 414) represent the true off-label cohort, 149 with “yellow” variants and 265 with VUSs. We evaluated demographic characteristics along with evidence of compassionate care for the “yellow” variant cohort. Compassionate care was categorized as: (1) death within 90 days of therapy prescription, (2) use of hospice services within 90 days of therapy prescription, and (3) no other treatment was given after therapy prescription.
All the patients in different cohorts were analyzed for their demographic characteristics. We evaluated the means, medians, and SD for continuous variables, and counts and proportions for categorical variables. All analyses were conducted using SAS software package 9.4.
Results
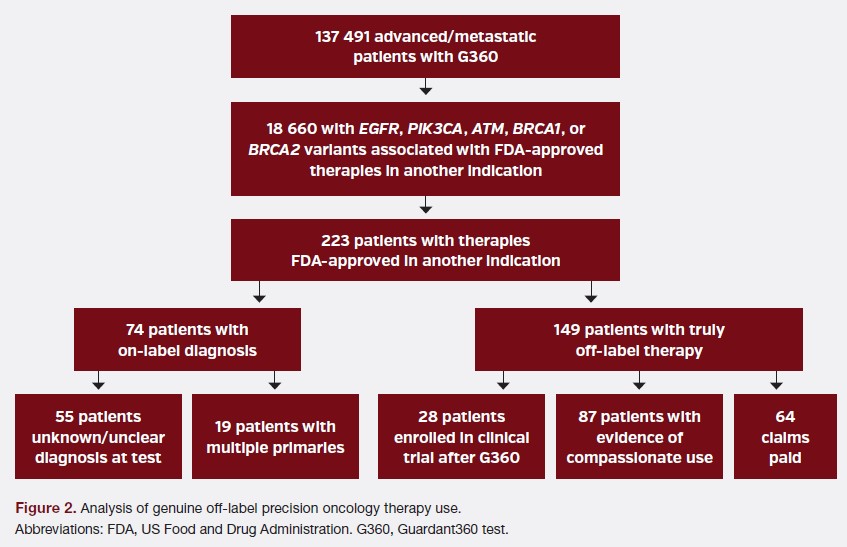
“Yellow” variants were present in 18 660 patients (n = 137 491; 14%). Only 149 patients with “yellow” variants (n = 137 491; 0.08%) subsequently had claims for the associated off-label precision oncology therapy without any evidence of on-label cancer type. Upon initial analysis, 223 patients with “yellow” variants had off-label precision oncology drug claims, but of this initial cohort of presumed off-label use, 74 patients had claims data and/or diagnosis codes consistent with on-label cancer indication upon further analysis, resulting in a genuinely off-label precision oncology therapy cohort of 149 patients with “yellow” variants (Figure 2). Of 74 patients with on-label cancer type, 19 (26%) had evidence of multiple primary lesions, and 55 (74%) had an unclarified diagnosis such as cancer of unknown primary site, neuroendocrine tumor, or a misaligned diagnosis at the time of testing.
Following exclusion of patients with on-label diagnoses codes, genuine off-label precision oncology therapy use was seen in 0.8% of patients with “yellow” variants (149/18 660) and 0.08% of all tested patients (149/137 491). Of the 149 patients with off-label precision oncology therapy use, claims for off-label therapies were paid for only 64 patients, representing 0.3% of patients with studied variants and 0.04% of all patients tested.
In the off-label cohort of 149 patients with “yellow” variants, ages ranged from 30 to 89 years, and the mean age was 65.6 years (SD 12.2). Roughly half of the patients were 65 years and over. There were 80 males and 69 females. Because compassionate use or expanded access is a circumstance where off-label therapy may be used, we analyzed the cohort with off-label precision oncology claims for clinical signs of compassionate use, which may suggest end-stage disease or last line of therapy use case. There was evidence of compassionate use for 87 (58%) patients with off-label precision oncology therapies prescribed: 55 patients died within 90 days of therapy, and 51 patients began hospice within 90 days of therapy (categories were not mutually exclusive). Twenty-eight patients (19%) enrolled in clinical trials following testing.
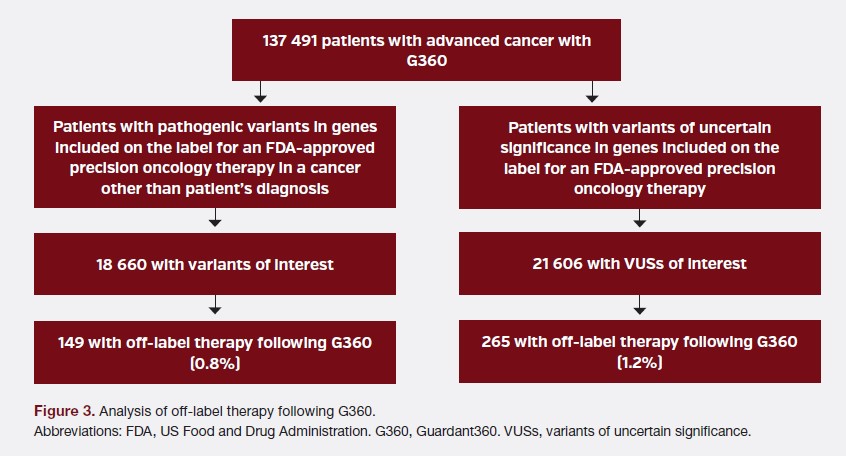
Secondary analysis was performed for 21 606 patients with VUSs, showing that only 265 patients had subsequent off-label therapy claims (n = 21 606; 1.2%). Of all patients tested, only 0.19% had off-label therapy following a VUS reported in the five genes studied. Considering the two analyses, only 414 patients (1.2%) with “yellow” variants or VUSs had any off-label drug use following G360 (Figure 3). A majority of the off-label drug use in both the “yellow” variant and VUS cohorts was for EGFR tyrosine kinase inhibition therapy or alpelisib (Supplementary Figure 3).
Discussion
Off-label utilization of FDA-approved precision oncology drugs associated with five genes designated on the Guardant360 reports was 1.2% in our study. Only 414 patients with advanced solid cancer with the studied variants reported on molecular profiling subsequently received the associated precision oncology therapy outside FDA label–intended use. This is the first study, to our knowledge, to specifically examine the off-label utilization of precision oncology drugs for which mutation status guides the intended use of an FDA-approved targeted therapy, though the scope was limited to five genes’ associated variants and VUSs. These mutation-drug pairings have been the source of concern from providers and payers objecting to comprehensive genomic profiling via NGS panel tests containing additional genomic targets beyond those actionable in a single indication.2,5 However, the current study suggests the real-world prescription of these select precision oncology drugs following testing was infrequent.
Risk of Harm Associated With CGP NGS Panels
Mitigating the risk for harm is a consideration of medical policy and assessment of genetic testing for advanced cancers. Specific harms may include ineffective or dangerous treatment resulting from genetic testing, which is misused, misinterpreted, or unreliable. Notable examples of harm exist in hereditary cancer testing, with physician misinterpretation of genetic variants resulting in an unnecessary mastectomy in up to half of average-risk patients.18 Genomic malpractice litigation in the areas of hereditary cancer, carrier screening, and pharmacogenomic testing occur at a rate of 12 cases per year.19 There is not an active genomic malpractice suit involving oncologists misinterpreting somatic test results.19 There is little evidence in the literature to support that somatic genetic tests lead to treatments that may harm the patient. Studies have suggested that providers may even utilize off-label therapy at a low rate following NGS genetic testing.11,12
When considering the other risks of harm for patients with advanced cancers, a chief concern may be incomplete or underutilized genetic testing for proven biomarkers to guide therapy and improve patient outcomes. Targeted testing, single-gene testing, and testing dependent on tissue samples have been shown to lead to undergenotyping of patients with advanced non–small cell lung cancer (NSCLC), colorectal cancer, and breast cancer, to name a few.15,21–24 Undergenotyping in NSCLC, for example, may have dire consequences, as EGFR mutation–positive patients may not benefit from, or may experience adverse effects with, immunotherapy.25,26 Comprehensive genomic profiling via multicancer NGS panels has been shown to increase the complete genotyping rate for patients with advanced cancer.16,23,24 The prevalence of patients with on-label diagnoses (n = 74) among the study cohort demonstrates that an indication-specific approach limits diagnostic and clinical utility.
Cost Impact of Multicancer NGS Panels for Tumor Profiling
Cost of testing is not typically included in most payer policy evidence frameworks and is prohibited in public payer coverage decisions; however, in considering a service “medically necessary,” common definitions include that a service is “likely to produce incremental health benefits relative to the next best alternative that justify any added cost.”27–29 Nearly a third of payers felt panels containing novel targets would not necessarily preclude coverage if labeled as such and “associated treatments are not submitted for reimbursement.”2 Our study shows that among the 149 patients with “yellow” variants and claims for true off-label therapy, only 43% were paid. This would be consistent with payer practice of “payment on exception basis,” and our study shows that payer concern that CGP NGS panels will “drive higher exception volume” may not be supported by real-world evidence with such a small number of claims.2
Cost-benefit of multicancer CGP NGS panels compared to standard of care sequential or hot-spot testing has been shown in several economic model studies for NSCLC, including one CVS Health project demonstrating an $8000 reduction per member per month in 6 months post-test.28,30-32 Contributing to cost-effectiveness, CGP was noted to reduce utilization of immunotherapy in the first line, as targetable drivers are identified. Notably, these studies did not account for KRAS G12C as a targetable driver, which has changed with regulatory approval of a RAS-associated drug in May 2021 and increased the potential for targeted therapy in the NSCLC population by 13%.33 An additional benefit was seen in that 19% of patients in the off-label cohort were subsequently enrolled in clinical trials. Though specific trials could not be identified in the data set, direction to clinical trials is considered best practice for eligible patients. Because clinical trials often absorb the costs of any treatment falling outside the standard of care, there may be an economic benefit. However, this was not analyzed in the current study derived from payer claims data.
Limitations
Limitations of the study include those inherent to the data set: (1) This is an observational data set with confounding variables such as Eastern Cooperative Oncology Group score, the severity of disease, and provider type. (2) Due to the patient dynamics of health insurance, missing claims data may exist, but queries for only patients with complete records were executed for this study. (3) The patients were not individually staged for this project, though the data set as a whole represents patients with advanced/metastatic solid cancer. (4) Ethnic and racial data were not available. (5) Access to off-label therapy may occur outside of claims billed, such as patient access programs through pharmaceutical sponsors. G360 assays mayidentify potential germline variants but cannot definitively rule in or out the presence of a germline mutation. For this reason, precision oncology therapies indicated when germline variants for particular cancer types are present were excluded from off-label cohort analysis (Table 1). We analyzed five actionable genes for this analysis. Exclusion of therapies or variants with low occurrence (less than 1% of reported variants) in our total tested cohort may limit assessment, though this cutoff was selected to allow sufficient subanalyses. By excluding variants with low occurrence, our analysis may under- or over-represent off-label therapy resulting from CGP as a whole. All patients in this study received G360 testing, which may present a biased selection of patients and providers with interest or comfort utilizing CGP via plasma-based technologies, thus lacking a control arm for this study. However, the population studied reflects diverse practitioners who vary in the treatment of patients with advanced cancer and coding for services/therapies. Additionally, Guardant Health employs a medical affairs team to support provider interpretation of G360 results, limiting the application of study results across laboratories and assays without robust provider support.
Future studies may expand on this work by examining off-label utilization for precision oncology drugs among all tested patients or untested cohorts. The economic impact of off-label paid claims may be weighed against the outcomes seen in clinical trial participants and those patients who were found to have an on-label diagnosis.
Conclusions
This study is the first to examine the utilization of precision oncology drugs outside of labeled indications following CGP in a large cohort. Off-label utilization of precision oncology therapy was low, even in the patients with variants clearly associated with the drug of interest. With transparent, guideline-aligned reporting and support for providers, comprehensive genomic profiling of advanced solid tumors can identify targeted therapies and direct more patients to clinical trials without increasing off-label utilization of precision oncology therapies.
This article has supplementary material, which can be accessed here and here.
Author Information
Authors: Julie Wiedower, PhDc; Nicole Zhang, MPH; Rebecca Nagy, MS; Kathryn Lang, MD; Jayati Saha, PhD, MPH
Affiliations: Guardant Health, Redwood City, CA
Address correspondence to:
Julie Wiedower Kaylor, MS, CGC
5 Degray Cove Maumelle, AR 72113
Phone: 501-450-0406
Email: jkaylor@guardanthealth.com
Disclosures: At the time of study, all authors are employees of and hold stock in Guardant Health.
References
1. Mazières J, Zalcman G, Crinò L, et al. Crizotinib therapy for advanced lung adenocarcinoma and a ROS1 rearrangement: results from the EUROS1 cohort. J Clin Oncol. 2015;33(9):992-999. doi:10.1200/JCO.2014.58.3302
2. Trosman JR, Weldon CB, Kate Kelley R, Phillips KA. Challenges of coverage policy development for next-generation tumor sequencing panels: experts and payers weigh in. J Natl Compr Cancer Netw JNCCN. 2015;13(3):311-318. doi:10.6004/ jnccn.2015.0043
3. Hamilton SA, Sagar B, Christensen K, Bowers A, Dollear T. Increased adherence to molecular profiling recommendations in non–small cell lung cancer through use of prior authorization and peer review. J Clin Oncol. 2022;40(16_suppl):9129-9129. doi:10.1200/JCO.2022.40.16_suppl.9129
4. “Off-label” indications for oncology drug use and drug compendia: history and current status. J Oncol Pract. 2005;1(3):102-105. doi:10.1200/JOP.2005.1.3.102
5. Mosele F, Remon J, Mateo J, et al. Recommendations for the use of next-generation sequencing (NGS) for patients with metastatic cancers: a report from the ESMO Precision Medicine Working Group. Ann Oncol Off J Eur Soc Med Oncol. 2020;31(11):1491-1505. doi:10.1016/j.annonc.2020.07.014
6. Moscow JA, Fojo T, Schilsky RL. The evidence framework for precision cancer medicine. Nat Rev Clin Oncol. 2018;15(3):183-192. doi:10.1038/nrclinonc.2017.186
7. Conti RM, Bernstein AC, Villaflor VM, Schilsky RL, Rosenthal MB, Bach PB. Prevalence of off-label use and spending in 2010 among patent-protected chemotherapies in a population-based cohort of medical oncologists. J Clin Oncol Off J Am Soc Clin Oncol. 2013;31(9):1134-1139. doi:10.1200/JCO.2012.42.7252
8. De Souza JA, Duong YY. Off-label immunotherapy prescription: financial implications for payers and patients. J Clin Oncol. 2017;35(8_suppl):6-6. doi:10.1200/ JCO.2017.35.8_suppl.6
9. Schram AM, Reales D, Galle J, et al. Oncologist use and perception of large panel next-generation tumor sequencing. Ann Oncol Off J Eur Soc Med Oncol. 2017;28(9):2298-2304. doi:10.1093/annonc/mdx294
10. Cobain EF, Wu YM, Vats P, et al. Assessment of clinical benefit of integrative genomic profiling in advanced solid tumors. JAMA Oncol. 2021;7(4):1-9. doi:10.1001/ jamaoncol.2020.7987
11. VanderWalde A, Grothey A, Vaena D, et al. Establishment of a Molecular Tumor Board (MTB) and uptake of recommendations in a community setting. J Pers Med. 2020;10(4). doi:10.3390/jpm10040252
12. Dalton WB, Forde PM, Kang H, et al. Personalized medicine in the oncology clinic: implementation and outcomes of the Johns Hopkins Molecular Tumor Board. JCO Precis Oncol. 2017. doi:10.1200/PO.16.00046
13. Rodler S, Jung A, Greif PA, et al. Routine application of next-generation sequencing testing in uro-oncology-Are we ready for the next step of personalised medicine? Eur J Cancer Oxf Engl 1990. 2021;146:1-10. doi:10.1016/j.ejca.2020.12.024
14. Palmero R, Taus A, Viteri S, et al. Biomarker discovery and outcomes for comprehensive cell-free circulating tumor DNA versus standard-of-care tissue testing in advanced non–small-cell lung cancer. JCO Precis Oncol. 2021;(5):93-102. doi:10.1200/PO.20.00241
15. Vidula N, Rich TA, Sartor O, et al. Routine plasma-based genotyping to comprehensively detect germline, somatic, and reversion BRCA mutations among patients with advanced solid tumors. Clin Cancer Res Off J Am Assoc Cancer Res. 2020;26(11):2546-2555. doi:10.1158/1078-0432.CCR-19-2933
16. Nakamura Y, Taniguchi H, Ikeda M, et al. Clinical utility of circulating tumor DNA sequencing in advanced gastrointestinal cancer: SCRUM-Japan GI-SCREEN and GOZILA studies. Nat Med. Published online October 5, 2020. doi:10.1038/s41591- 020-1063-5
17. Whitfield K, Huemer KH, Winter D, et al. Compassionate use of interventions: results of a European Clinical Research Infrastructures Network (ECRIN) survey of ten European countries. Trials. 2010;11:104. doi:10.1186/1745-6215-11-104
18. Kurian AW, Li Y, Hamilton AS, et al. Gaps in incorporating germline genetic testing into treatment decision-making for early-stage breast cancer. J Clin Oncol. Published online April 12, 2017;35(20): 2232-2239. doi:10.1200/JCO.2016.71.6480
19. Genomic malpractice: what healthcare providers need to know to reduce the risk. Precision Medicine Advisors. Accessed July 1, 2021. https://www.precisionmedicineadvisors.com/precisionmedicine-blog/2019/6/10/why-fear-of-genomic-malpractice-might-make-healthcare-providers-more-likely-to-use-genetic-tests
20. Nakamura Y, Olsen S, Zhang N, Liao J, Yoshino T. Comprehensive genomic profiling of circulating tumor DNA in patients with previously treated metastatic colorectal cancer: analysis of a real-world healthcare claims database. Curr Oncol Tor Ont. 2022;29(5):3433-3448. doi:10.3390/curroncol29050277
21. Gutierrez ME, Choi K, Lanman RB, et al. Genomic profiling of advanced non-small cell lung cancer in community settings: gaps and opportunities. Clin Lung Cancer. 2017;18(16):651-659. doi:10.1016/j.cllc.2017.04.004
22. Gutierrez ME, Price KS, Lanman RB, et al. Genomic profiling for KRAS, NRAS, BRAF, microsatellite instability, and mismatch repair deficiency among patients with metastatic colon cancer. JCO Precis Oncol. 2019;(3):1-9. doi:10.1200/PO.19.00274
23. Leighl NB, Page RD, Raymond VM, et al. Clinical utility of comprehensive cell-free DNA analysis to identify genomic biomarkers in patients with newly diagnosed metastatic non–small cell lung cancer. Clin Cancer Res. 2019;25(15):4691-4700. doi:10.1158/1078-0432.CCR-19-0624
24. Aggarwal C, Thompson JC, Black TA, et al. Clinical implications of plasma-based genotyping with the delivery of personalized therapy in metastatic non-small cell lung cancer. JAMA Oncol. 2019;5(2):173-180. doi:10.1001/jamaoncol.2018.4305
25. Calles A, Riess JW, Brahmer JR. Checkpoint blockade in lung cancer with driver mutation: choose the road wisely. Am Soc Clin Oncol Educ Book. 2020;(40):372- 384. doi:10.1200/EDBK_280795
26. Schoenfeld AJ, Arbour KC, Rizvi H, et al. Severe immune-related adverse events are common with sequential PD-(L)1 blockade and osimertinib. Ann Oncol Off J Eur Soc Med Oncol. 2019;30(5):839-844. doi:10.1093/annonc/mdz077
27. Trosman JR, Weldon CB, Gradishar WJ, et al. From the past to the present: insurer coverage frameworks for next-generation tumor sequencing. Value Health J Int Soc Pharmacoeconomics Outcomes Res. 2018;21(9):1062-1068. doi:10.1016/j. jval.2018.06.011
28. Pennell NA, Mutebi A, Zhou ZY, et al. Economic impact of next-generation sequencing versus single-gene testing to detect genomic alterations in metastatic non–small-cell lung cancer using a decision analytic model. JCO Precis Oncol. 2019;(3):1-9. doi:10.1200/PO.18.00356
29. Perspectives on Essential Health Benefits: Workshop Report. National Academies Press; 2012:13182. doi:10.17226/13182
30. Ezeife D, Spackman E, Juergens R, et al. OA16.02 The economic value of liquid biopsy for genomic profiling in advanced non-small cell lung cancer. J Thorac Oncol. 2021;16(10):S876. doi:10.1016/j.jtho.2021.08.087
31. Lopes G, Raymond V, Scott J, et al. P2.15-16 Clinical economic impact of improved genotyping in patients with advanced non-small cell lung adenocarcinoma (NSCLC). J Thorac Oncol. 2018;13(10):S823. doi:10.1016/j.jtho.2018.08.1457
32. Brito RA, Cullum B, Hastings K, Avalos-Reyes E, Karos R, Johnson KA. Total cost of lung cancer care associated with broad panel versus narrow panel sequencing. J Clin Oncol. 2020;38(15_suppl):7077-7077. doi:10.1200/JCO.2020.38.15_ suppl.7077
33. Pakkala S, Ramalingam SS. Personalized therapy for lung cancer: striking a moving target. JCI Insight. 2018;3(15):e120858. doi:10.1172/jci.insight.120858



