


Interpreting MRI Findings of Ankle Impingement Syndrome in Athletes
Click here for a related slideshow.
Years ago, I presented my first unpublished case series highlighting ankle impingement issues post–ankle open reduction and internal fixation (ORIF), post-Bröstrom, and then post–cartilage repair. Repeatedly I encountered fellow surgeons who scoffed at the notion that many soldiers and athletes would lose function and have persistent pain—or worse, require additional surgery due to ankle impingement. I would show them case after case of soldiers unable to resume pain-free activity and sports. All required repeat arthroscopy and every time I noted a combination of synovitis, undiagnosed cartilage damage, scar tissue, meniscoid lesions, or chondromalacia of varying degrees. Subsequently, I found most of these patients do resume normal activity post-debridement.
With significant evolution in arthroscopy over the past 20 years, led by the technique advancements and research from China, Korea, and the Netherlands,1-3 I feel that the world finally recognizes that ankle impingement is not just osseous, but a soft tissue issue one must not ignore (see Table 1).

Throughout the years, I reviewed numerous magnetic resonance images (MRIs), for trends and compared them with intraoperative findings like Lee and colleagues presented in 2004.2 Unlike a radiologist, I have the advantage of confirming predicted pathology during surgery. More importantly, I am able to retrospectively compare the MRIs with my arthroscopic findings. Looking backwards after surgery is a critical step for all providers. I believe we all improve by contrasting intraoperative findings with imaging findings. Honing my skills in doing so, and not relying on reports with possible over- or under-reads, has proven valuable. Once you are comfortable reading MRIs, you will be amazed at how much obvious intra-articular pathology becomes visible, just as Robinson described in his research in 2007.4
During courses and in collaboration with colleagues, it’s clear to me that soft tissue is not usually fully explored. So much of the focus I’ve observed in multiple specialties has been on cartilage, tendons, spurs and then lastly, bone bruising. I can safely state that after 4,000 ankle scopes in my own practice, it is soft tissue pathology that truly keeps soldiers and athletes from returning to pain-free activity. It is the stuff that sits in gutters, rubbing between the cartilage surfaces and the loss of cartilage resiliency that leads to loss of motion, painful motion and simply joint aching with activity. Radiologists like Donovan and Rosenberg in 2010 stressed the importance of MRI for assessing ankle impingement both osseous and soft tissue etiologies.5
How MRI Findings Can Lead Surgeons to Success
The focus of this column is to highlight the MRI findings that will yield intra-articular pathology and surgical success. Radiologists and surgeons have been working hand-in-hand and have seen significant strides in diagnostic capabilities since 2010 with featured articles and research expanding our understanding and diagnostic accuracy as we compare MRI to intraoperative findings.6-12
One of the other trends that I see ignored so often is joint line tenderness. There is essentially lateral side bias. If the ankle hurts, it has to be lateral pain, right? Well, maybe … but maybe not. There has been so much attention on the lateral ankle but rarely the medial ankle. I can show hundreds of cases from my practice for which the patients have lateral impingement symptoms only but have significant medial joint pathology intraoperatively. There is this notion or assumption that if you don’t have pain on one side of the ankle joint, then there must not be pathology. This is especially true with posterior ankle impingement, which we covered in my posterior ankle column in 2020.13
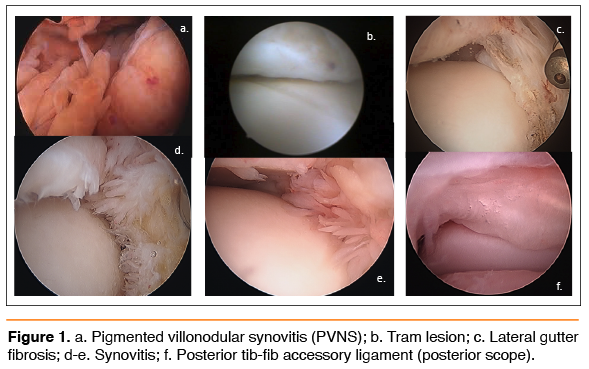
Today, many surgeons utilize an arthroscopic Bröstrom or will do an open Bröstrom with an arthroscope. I can tell you with a high certainty in my experience that athletes/soldiers will end up needing a secondary scope within 6–8 months because of the development of arthrofibrosis in the lateral gutter, or worse, improper inspection and debridement of the joint. As a result, I rarely scope during my initial Bröstrom. I will schedule my scope 3–4 months post-Bröstrom, or sooner if I know I have a cartilage lesion to address. Either way, athletes often end up with multiple surgeries, especially if they bounce from surgeon to surgeon. There is nothing wrong with staging; and I must emphasize that there is nothing wrong with the Bröstrom/scope combo as long as we warn our patients of the likelihood of needing a second scope in the future. Remember, the whole goal of the Bröstrom is to develop scar tissue and restore stability, which often complicates ankle range of motion. I have scoped over 1,500 of my own Bröstroms due to fibrosis and inability to resume pain-free running. The results are consistently the same: scarring within the lateral gutter along with widespread synovitis, which was present prior to the Bröstrom as shown in Figure 1c.
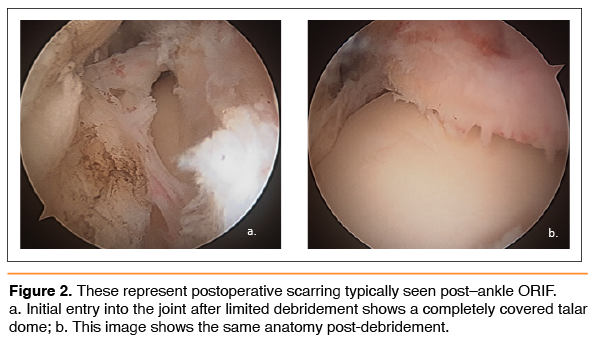
So don’t get fooled. I did an unpublished retrospective study many years ago comparing exam findings to intra-articular pathology findings. I found it very rare that a patient complained of lateral and medial ankle joint pain together despite finding widespread pathology. More often I saw synovitis throughout the joint, almost never on an isolated side. Let us not forget that tibial spurs more often are lateral, but talar spurs are almost always medial. In my experience, there is no correlation with the exam to intra-articular pathology. We can’t ignore inspecting the entire joint as Ferkel recommended so many years ago.14 If you don’t follow an organized pattern of inspection, you will miss pathology, especially when you are dealing with a post-ORIF ankle. So often the entire joint is filled with scar tissue as shown in Figure 2. Let us not forget, one goal of arthroscopy is to inspect the cartilage, and that can’t be done until one clears the scar tissue. I have seen many new patients arrive with scope images from a previous surgery. Far too often, images of the medial gutter, posterior ankle or syndesmosis aren’t included.
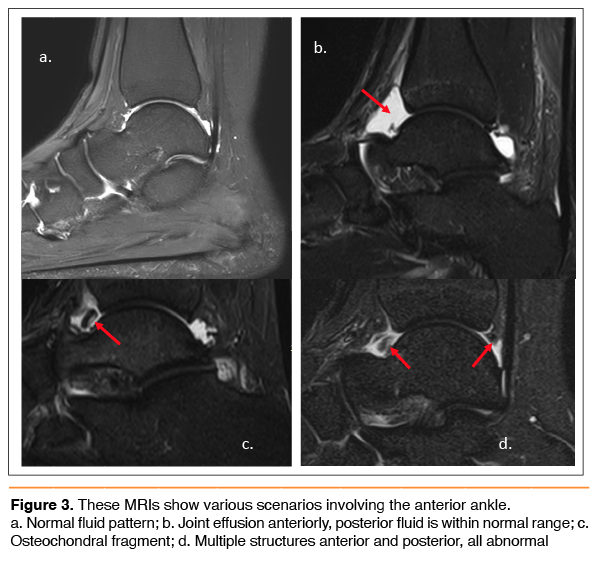
Now to the MRIs: I recommend one reviews the T1 and T2 sagittal images first. The T1 will be very helpful in assessing the joint morphology, and T2 will aid in determining the location and volume of the anterior and posterior joint capsule. Once we can start identifying pathology, we can then pinpoint the true location by triangulating with the coronals for medial/lateral positioning.
I did an unpublished review of over 1000 ankle MRIs over the past 10 years. MRI pathology has to correlate with an exam to assess the level of disability. Obviously, a positive MRI doesn’t require surgery in every patient. With athletes, pathology seems to catch up with them over time. They have a habit of adding years of wear and tear or sustaining repeated ankle injuries which exacerbate the current pathology.
In Conclusion
My focus is simple: I want to highlight commonly missed MRI pathology. It is probably not critical to identify what you see as much as recognizing that this structure or signal is abnormal (Figure 3). That is critical for educating patients. So when you see a large object or structure that shouldn’t be there, the patient will be able to comprehend why their ankle actually hurts, clicks, pops, or locks up. This educates not just our patients but ourselves on the benefits of surgery.
A. Douglas Spitalny, DPM, is a Staff Podiatrist at Ft. Leonard Wood, MO.
References
- Tol JL, van Dijk CN. Anterior ankle impingement. Foot Ankle Clin. 2006 Jun;11(2):297-310, vi. doi: 10.1016/j.fcl.2006.02.002. PMID: 16798513.
- Lee JW, Suh JS, Huh YM, Moon ES, Kim SJ. Soft tissue impingement syndrome of the ankle: diagnostic efficacy of MRI and clinical results after arthroscopic treatment. Foot Ankle Int. 2004 Dec;25(12):
- 896-902. doi: 10.1177/107110070402501209. PMID: 15680103.
- Egol KA, Parisien JS. Impingement syndrome of the ankle caused by a medial meniscoid lesion. Arthroscopy. 1997 Aug;13(4):522-5. doi: 10.1016/s0749-8063(97)90136-5. PMID: 9276064.
- Robinson P. Impingement syndromes of the ankle. Eur Radiol. 2007 Dec;17(12):3056-65.
- Donovan A, Rosenberg ZS. MRI of ankle and lateral hindfoot impingement syndromes. AJR Am J Roentgenol. 2010 Sep;195(3):595-604. doi: 10.2214/AJR.09.4199. PMID: 20729435.
- Dimmick S, Linklater J. Ankle impingement syndromes. Radiol Clin North Am. 2013 May;51(3):479-510.
- Russo A, Zappia M, Reginelli A, Carfora M, D’Agosto GF, La Porta M, Genovese EA, Fonio P. Ankle impingement: a review of multimodality imaging approach. Musculoskelet Surg. 2013 Aug;97 Suppl 2:S161-8. doi: 10.1007/s12306-013-0286-8. Epub 2013 Aug 15. PMID: 23949938.
- Lavery KP, McHale KJ, Rossy WH, Theodore G. Ankle impingement. J Orthop Surg Res. 2016 Sep 9;11(1):97. doi: 10.1186/s13018-016-0430-x. PMID: 27608626; PMCID: PMC5016963.
- 9. Shane AM, Reeves CL, Vazales R, Farley Z. Soft tissue impingement of the ankle: pathophysiology, evaluation, and arthroscopic treatment. Clin Podiatr Med Surg. 2016 Oct;33(4):503-20. doi: 10.1016/j.cpm.2016.06.003. PMID: 27599436.
- Al-Riyami AM, Tan HK, Peh WCG. Imaging of ankle impingement syndromes. Can Assoc Radiol J. 2017 Nov;68(4):431-437. doi: 10.1016/j.carj.2017.04.001. Epub 2017 Aug 31. PMID: 28865671.
- LiMarzi GM, Khan O, Shah Y, Yablon CM. Imaging manifestations of ankle impingement syndromes. Radiol Clin North Am. 2018 Nov;56(6):893-916. doi: 10.1016/j.rcl.2018.06.005. PMID: 30322489.
- Zbojniewicz AM. Impingement syndromes of the ankle and hindfoot. Pediatr Radiol. 2019 Nov;49(12):1691-1701.
- Spitalny AD. A guide to posterior ankle arthroscopy in athletes. Podiatry Today. 2020; 33(8).
- 14. Ferkel R. Arthroscopic Surgery: The Foot and Ankle. Lippincott Williams & Wilkins. 1995.





