Topical Steroid Allergy
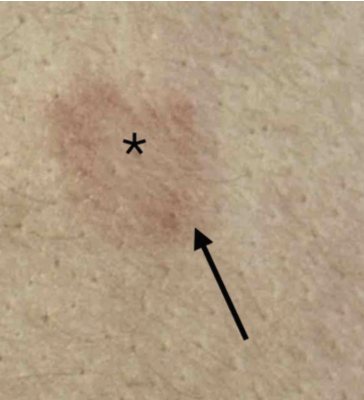
A 47-year-old Asian woman with a history of atopic dermatitis (AD) presented to the dermatology clinic with an ongoing rash on her hands, face, and bilateral axillae. Multiple rounds of topical steroids did not resolve her symptoms. She underwent patch testing with the Thin-layer Rapid Use Epicutaneous (TRUE) test, with placement on day 1 and reads on days 3 and 5. Physical examination during the day 5 reading revealed a rectangular-shaped, erythematous, scaly, thin plaque with central clearing, corresponding to a positive reaction to tixocortol-21-pivalate (Figure 1 and Figure 2).

Clinical Presentation
Topical steroid allergy is an underreported cause of persistent dermatitis, with studies reporting prevalence rates of 0.2% to 6% in patch-tested populations.1 Tixocortol is the most common topical steroid allergen.2 Positive patch tests to steroid allergens may typically present at delayed reads and show peripheral erythema, along with a central area of clearing where the presence of topical steroid partially treats the dermatitis resulting from the test, as was observed in our patient. Equivocal cases can be confirmed with intradermal testing.2 Other compounds that may cause a delayed positive reaction on patch testing include metals and topical antibiotics; however, these haptens would not cause the “edge effect” and would instead show a uniformly erythematous patch, plaque, or small vesicle at the application site. Counseling on avoidance of allergens is also difficult, as optimal classification for topical steroid cross-reactors remains an active area of research. Using the Coopman method, which groups steroids based on structural similarities at the molecular level, tixocortol is classified as a group A steroid, which may cross-react with members of group D2.3
Other classification schemes have been proposed that focus on the allergenicity of various compounds rather than their structural similarities. For example, Wilkinson et al. hypothesized that a lower degree of methylation at certain molecular positions, especially C16/17, drives T cell recognition of antigens that produces the type IV hypersensitivity response.4 Under this system, there are 3 steroid groups, with lower methylation equating to higher allergenicity: highly allergenic steroids include tixocortol and hydrocortisone, moderately allergenic steroids include triamcinolone and desonide, and low allergenic steroids include budesonide and clobetasol. Both the Coopman and Wilkinson classifications agree that tixocortol and hydrocortisone are among the most allergenic topical steroids, which justifies their presence in many common screening series, including the TRUE test.5
Further research is needed into topical steroid cross-reactivity. For patients with topical steroid allergy, it may be more practical for them to avoid steroids as much as possible and use alternative agents, such as calcineurin inhibitors or phosphodiesterase inhibitors, if feasible.
Patient Follow Up
Further medical history revealed that the patient had been prescribed desonide and hydrocortisone topical creams in the past, which may have triggered contact dermatitis and exacerbated underlying AD. The patient was advised to discontinue all topical steroids and switch to pimecrolimus cream, which resolved her symptoms.
References
1. Jagodzinski LJ, Taylor JS, Oriba H. Allergic contact dermatitis from topical corticosteroid preparations. Am J Contact Dermat. 1995;6(2):67-74. doi:10.1053/ ajcd.1995.3302
2. Mimesh S, Pratt M. Allergic contact dermatitis from corticosteroids: reproduc- ibility of patch testing and correlation with intradermal testing. Dermatitis. 2006;17(3):137-142. doi:10.2310/6620.2006.05048
3. Jacob SE, Steele T. Corticosteroid classes: a quick reference guide including patch test substances and cross-reactivity. J Am Acad Dermatol. 2006;54(4):723-727. doi:10.1016/j.jaad.2005.12.028
4. Wilkinson SM. Corticosteroid cross-reactions: an alternative view. Contact Dermatitis. 2000;42(2):59-63. doi:10.1034/j.1600-0536.2000.042002059.x
5. Baeck M, Marot L, Nicolas JF, Pilette C, Tennstedt D, Goossens A. Allergic hypersensitivity to topical and systemic corticosteroids: a review. Allergy. 2009;64(7):978-994. doi:10.1111/j.1398-9995.2009.02038.x