


Original Research
Copper Oxide Impregnated Wound Dressing: Biocidal and Safety Studies
December 2010
WOUNDS. 2010;22(12):301-310.
Abstract: Copper plays a key role in angiogenesis and in the expression and stabilization of extracellular skin proteins. Copper also exhibits broad biocidal properties. The authors hypothesized that introducing copper into a wound dressing would not only reduce the risk of wound and dressing contamination, but would also stimulate wound repair. To test this hypothesis, non-stick dressings composed of a highly absorbent internal mesh fabric and an external non-woven fabric were fabricated, and each was impregnated with ~2.65% (weight/weight) copper oxide particles. The application to wounds inflicted in genetically engineered diabetic mice resulted in increased gene and in-situ upregulation of proangiogenic factors, increased blood vessel formation, and enhanced wound closure. The present study reports both the potent broad spectrum antimicrobial and antifungal properties of these wound dressings and the lack of adverse reactions as determined in rabbits and a porcine wound model. The prolonged efficacy of the wound dressing is demonstrated by its capacity to reduce the microbial challenge by more than 99.9% even when spiked 5 consecutive times with a high bacterial titer. The dressing’s antimicrobial efficacy is exerted within minutes. The dressing did not cause any skin irritation or sensitization to closed skin. Furthermore, no histological differences were found between open wounds exposed to copper oxide containing wound dressings or control dressings. Therefore, copper containing wound dressings hold significant promise in wound healing and their clinical use should be explored.
Copper ions, either alone or in copper complexes, have been used for centuries to disinfect liquids, solids, and human tissue. Several mechanisms for the potent biocidal activity of copper have been proposed, which include alteration of proteins, and inhibition of their biological assembly and activity; plasma membrane permeabilization; and membrane lipid peroxidation.1 Sensitivity to copper may vary significantly among different bacteria2 or among bacteria of the same strains. For example, Enterococci bacteria isolated from the gut of pigs whose diet included high copper concentrations over many months were 7-fold less susceptible to copper than Enterococci bacteria isolated from pigs that were not fed copper.3 The increased tolerance to copper is achieved by the induction of an efflux pump in the tolerant bacteria. Similarly, reduced sensitivity to copper was found in nitrifying soil microorganisms exposed to copper for nearly 80 years under field conditions.4 However, copper-tolerant microbes are extremely rare, even though copper has been a part of the earth for millions of years and in use by humans for thousands of years.5 Furthermore, the microorganisms described above were up to 10-fold less sensitive to copper than the sensitive bacteria. This is a clear distinction from antibiotic resistant microbes that have evolved in less than 50 years of use, which in some cases have up to 2200-fold decreased sensitivity to the antibiotic (eg, erythromycin).6 This lack of resistance to copper may be explained by the capacity of copper to damage in parallel many key components of microorganisms in a nonspecific mechanism.1
Human skin, in contrast to microorganisms, is not sensitive to copper and the risk of adverse reactions due to dermal exposure to copper is extremely low.7,8 Copper is not only considered safe for humans, as demonstrated by the widespread and prolonged use of copper intrauterine devices (IUDs) by women,9,10 but it is an essential metal that facilitates normal metabolic processes.11 The US National Academy of Sciences Committee recommends a daily allowance of 0.9 mg of copper for normal adults. This committee also noted that daily intake of up to 3 mg/d in children and 8 mg–10 mg/d for adults is considered tolerable and nontoxic.12
More data are being gathered to support the hypothesis that copper is involved and may be a key player in many of the complicated processes that comprise the wound repair mechanism. Some obvious examples include stimulation of angiogenesis facilitated by the Cu2+ -dependent formation of multiprotein complexes containing the S100A13 protein13; stimulation of angiogenesis facilitated by induction of vascular endothelial growth factor (VEGF)14–16; expression of integrin17; stabilization of fibrinogen and collagen18–20; upregulation of copper-dependent enzymes, such as lysyl oxidase, important for matrix remodeling, cell proliferation, and re-epithelization21,22; reduction of tissue oxidative damage after injury23; and activation of tissue remodeling.24 The importance of copper in wound healing is further demonstrated by the positive and beneficial effect of its administration in cases of severe burn trauma in children25 and in the management of phosphorus burns.26
Evidence continues to show that bacteria in chronic wounds live within biofilm communities, in which the bacteria are protected from host defenses and develop resistance to antibiotic treatment.27 Considering the potent biocidal activities of copper,1 the minimal risk of adverse skin reactions associated with copper,7,8 and its roles in the wound healing process, the authors hypothesized28 that the addition or application of copper or copper containing products to wounds, such as copper containing Band-Aids and pads, would not only reduce the risk of wound and dressing contamination, as does silver, but, more importantly, may significantly enhance the wound healing process, especially in cases where the healing process is impaired (eg, diabetic ulcers).
Indeed, application of the wound dressings containing copper oxide to wounds inflicted in genetically engineered diabetic mice (C57BL/KsOlaHsd-Leprdb) resulted in increased gene and in-situ upregulation of proangiogenic factors (eg, placental growth factor, HIF-1a, and VEGF), increased blood vessel formation (P 0.05) and enhanced wound closure (P 0.01), as compared to control dressings (without copper) or commercial wound dressings containing silver.29 The following study presents the biocidal properties of nonstick dressings containing copper oxide particles and their safety in animal models.
 The fibers were examined by scanning electron microscopy (SEM) and the presence of copper was determined by x-ray photoelectron spectrum analysis, as shown in Figure 1.
Determination of antibacterial and antifungal properties. The antibacterial and antifungal properties of the internal and envelope layers of the test dressings were determined according to the American Association of Textile Chemists and Colorists (AATCC) Test Method 100-1993. Briefly, sterile swatches weighing 0.50 g ± 0.01 g of the copper containing fabrics and of similar fabrics without copper (control fabrics) were placed in sterile vials and exposed to 0.5 mL saline solution containing 1 x 105 to 4 x 106 colony forming units (CFUs). The spiked samples were then incubated at room temperature for 4 hours unless otherwise specified. After the incubation period, the test samples were transferred aseptically to Stomager bags containing 100 mL of saline solution and 0.1% of Tween 80 (wash buffer). The bags were then shaken vigorously for 2 minutes. Aliquots of 0.1 mL, 1 mL, and 10 mL of the liquid from each bag were then added to the wash buffer to a final volume of 20 mL. The 20-mL samples were then passed through a 0.45-µm membrane using a vacuum pump and a Gelman/Pall filtration device. The membranes containing the bacteria/fungi were washed with 50 mL of wash buffer and then placed in Petri dishes containing selective culture media. The plates were incubated at 35˚C ± 1˚C for 24 hours and the number of bacterial or fungi colonies were counted. Tests in which the incubation time was minutes, 10 mL of sterile standard DE (Dey/Engley) Neutralizing Broth was added to the spiked samples in order to neutralize antimicrobial activity. The log reduction of bacterial or fungal titers was calculated with the following formula: Log A – Log B = Log R to the nearest hundred, where R = reduction; A = population of the challenge organism; B = the number of test organisms recovered from the inoculated test sample. The test organisms studied were: Escherichia coli (ATCC # 8739); Klebsiella pneumoniae (ATCC# 13883); Enterococcus fecalis (ATCC 29212); Pseudomonas aeruginosa (ATCC 9027); Staphylococcus aureus (ATCC 6538); and Candida albicans (ATCC 10231).
The fibers were examined by scanning electron microscopy (SEM) and the presence of copper was determined by x-ray photoelectron spectrum analysis, as shown in Figure 1.
Determination of antibacterial and antifungal properties. The antibacterial and antifungal properties of the internal and envelope layers of the test dressings were determined according to the American Association of Textile Chemists and Colorists (AATCC) Test Method 100-1993. Briefly, sterile swatches weighing 0.50 g ± 0.01 g of the copper containing fabrics and of similar fabrics without copper (control fabrics) were placed in sterile vials and exposed to 0.5 mL saline solution containing 1 x 105 to 4 x 106 colony forming units (CFUs). The spiked samples were then incubated at room temperature for 4 hours unless otherwise specified. After the incubation period, the test samples were transferred aseptically to Stomager bags containing 100 mL of saline solution and 0.1% of Tween 80 (wash buffer). The bags were then shaken vigorously for 2 minutes. Aliquots of 0.1 mL, 1 mL, and 10 mL of the liquid from each bag were then added to the wash buffer to a final volume of 20 mL. The 20-mL samples were then passed through a 0.45-µm membrane using a vacuum pump and a Gelman/Pall filtration device. The membranes containing the bacteria/fungi were washed with 50 mL of wash buffer and then placed in Petri dishes containing selective culture media. The plates were incubated at 35˚C ± 1˚C for 24 hours and the number of bacterial or fungi colonies were counted. Tests in which the incubation time was minutes, 10 mL of sterile standard DE (Dey/Engley) Neutralizing Broth was added to the spiked samples in order to neutralize antimicrobial activity. The log reduction of bacterial or fungal titers was calculated with the following formula: Log A – Log B = Log R to the nearest hundred, where R = reduction; A = population of the challenge organism; B = the number of test organisms recovered from the inoculated test sample. The test organisms studied were: Escherichia coli (ATCC # 8739); Klebsiella pneumoniae (ATCC# 13883); Enterococcus fecalis (ATCC 29212); Pseudomonas aeruginosa (ATCC 9027); Staphylococcus aureus (ATCC 6538); and Candida albicans (ATCC 10231).
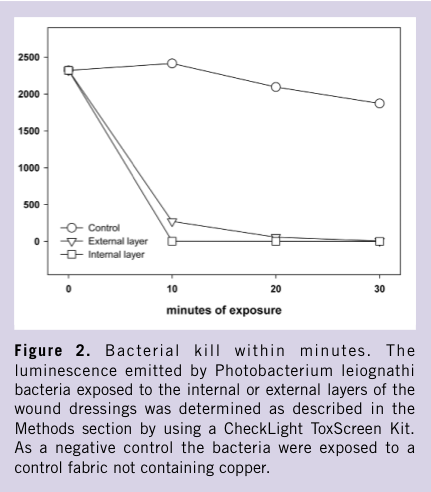
 In addition to the viability tests, a highly sensitive CheckLight ToxScreen Kit (CheckLight Ltd, Qiryat-Tivon, Israel) was used to determine the biocidal efficacy of the control and test items. The assay is based on the luminescence emitted by the marine bacterium Photobacterium leiognathi. The reduction of the bacteria luminescence is correlated with the bacteria viability, which can be measured within minutes of the bacterial exposure to the test items or liquid that came into contact with the test items. The assay was performed according to manufacturer’s instructions. Briefly, a 1.5-mL buffer supplied with the kit was added to 1 cm2 of the control or test item. After 1 minute of vigorous mixing, 1 mL of each mix was withdrawn into a fresh tube containing the bacteria. The tubes were incubated at 27˚C for 10–30 minutes, during which aliquots were withdrawn and the luminescence was determined using a luminometer with a spectral sensitivity range of 380 nm–630 nm. Negative (buffer only) and positive controls (1:100 dilution of a copper chloride solution provided in the kit in buffer) were included and the light level emitted by the test items was compared to that emitted by the positive and negative controls.
Rabbit skin sensitization test. The potential dermal irritation and delayed-type hypersensitivity of the spun-bond polypropylene and of the copper plated cellulosic fibers that comprise the test dressings and contain 2.3% and 3% copper oxide (w/w), respectively, were assessed in 6 Hsdlf:NZW rabbits (3 and 3, respectively) according to the International Standard (ISO 10993-10:2002). An independent laboratory (Harlan Biotech Israel, Ltd.) performed the test under GLP procedures. Briefly, two sites in each animal served as test sites and two others as control sites. Approximately 24 hours before the test, fur was removed by closely clipping a sufficient distance on both sides of the spine for application and observations of all sites (approx. 10 cm × 15 cm). Care was taken to avoid abrading the skin, and only animals with healthy, intact skin were used. Following application, each test site or control site was dressed for a total of 4 hours. At the end of the contact time, the dressings were removed and the positions of the patches were re-marked. Dermal reactions for erythema, eschar, and edema formation were scored according to the test guidelines and recorded at the standard time points of 1, 24, 48, and 72 hours after dressing removal.
In addition to the viability tests, a highly sensitive CheckLight ToxScreen Kit (CheckLight Ltd, Qiryat-Tivon, Israel) was used to determine the biocidal efficacy of the control and test items. The assay is based on the luminescence emitted by the marine bacterium Photobacterium leiognathi. The reduction of the bacteria luminescence is correlated with the bacteria viability, which can be measured within minutes of the bacterial exposure to the test items or liquid that came into contact with the test items. The assay was performed according to manufacturer’s instructions. Briefly, a 1.5-mL buffer supplied with the kit was added to 1 cm2 of the control or test item. After 1 minute of vigorous mixing, 1 mL of each mix was withdrawn into a fresh tube containing the bacteria. The tubes were incubated at 27˚C for 10–30 minutes, during which aliquots were withdrawn and the luminescence was determined using a luminometer with a spectral sensitivity range of 380 nm–630 nm. Negative (buffer only) and positive controls (1:100 dilution of a copper chloride solution provided in the kit in buffer) were included and the light level emitted by the test items was compared to that emitted by the positive and negative controls.
Rabbit skin sensitization test. The potential dermal irritation and delayed-type hypersensitivity of the spun-bond polypropylene and of the copper plated cellulosic fibers that comprise the test dressings and contain 2.3% and 3% copper oxide (w/w), respectively, were assessed in 6 Hsdlf:NZW rabbits (3 and 3, respectively) according to the International Standard (ISO 10993-10:2002). An independent laboratory (Harlan Biotech Israel, Ltd.) performed the test under GLP procedures. Briefly, two sites in each animal served as test sites and two others as control sites. Approximately 24 hours before the test, fur was removed by closely clipping a sufficient distance on both sides of the spine for application and observations of all sites (approx. 10 cm × 15 cm). Care was taken to avoid abrading the skin, and only animals with healthy, intact skin were used. Following application, each test site or control site was dressed for a total of 4 hours. At the end of the contact time, the dressings were removed and the positions of the patches were re-marked. Dermal reactions for erythema, eschar, and edema formation were scored according to the test guidelines and recorded at the standard time points of 1, 24, 48, and 72 hours after dressing removal.
 Porcine partial-thickness wound model. The skin of pigs is considered the closest model to human skin in terms of the anatomical and physiological characteristics of skin.32 We therefore examined possible adverse effects of applying the test dressings on wounds by using a porcine partial-thickness wound model. An independent laboratory (Harlan Biotech Israel, Ltd.) performed this experiment using a large, white, Landrace female pig weighing ~50 kg. Test sites comprised a total of 12 evenly bilateral allocated punch biopsy partial-thickness wounds each measuring approximately 12 mm in diameter and 5 mm in depth. Immediately after wounding, six randomly chosen wounds were covered with test dressings and the remaining 6 wounds with control commercial sterile dressing pads (hereafter referred to as control dressings). Comparable assessments of the test dressing and control dressing covered wound sites at day 3 and day 7 post-wounding were conducted by macroscopic examination and scoring of local dermal reactions (erythema, edema, and crust formation), and by microscopic examination following biopsy harvest. In addition to assessing the direct effects at the wound sites, blood samples were collected at the pre-test stage (baseline control) and at the time of the two respective biopsy harvest sessions on study days 3 and 7 post-wounding to resolve any potential treatment effects on clinical pathology parameters.
Porcine partial-thickness wound model. The skin of pigs is considered the closest model to human skin in terms of the anatomical and physiological characteristics of skin.32 We therefore examined possible adverse effects of applying the test dressings on wounds by using a porcine partial-thickness wound model. An independent laboratory (Harlan Biotech Israel, Ltd.) performed this experiment using a large, white, Landrace female pig weighing ~50 kg. Test sites comprised a total of 12 evenly bilateral allocated punch biopsy partial-thickness wounds each measuring approximately 12 mm in diameter and 5 mm in depth. Immediately after wounding, six randomly chosen wounds were covered with test dressings and the remaining 6 wounds with control commercial sterile dressing pads (hereafter referred to as control dressings). Comparable assessments of the test dressing and control dressing covered wound sites at day 3 and day 7 post-wounding were conducted by macroscopic examination and scoring of local dermal reactions (erythema, edema, and crust formation), and by microscopic examination following biopsy harvest. In addition to assessing the direct effects at the wound sites, blood samples were collected at the pre-test stage (baseline control) and at the time of the two respective biopsy harvest sessions on study days 3 and 7 post-wounding to resolve any potential treatment effects on clinical pathology parameters.
 Skin sensitization. None of the animals exposed to the internal or exterior fabric of the test dressings showed any dermal reactions throughout the entire 72-hour observation period. There was no evidence of erythema, eschar, or edema formation. The calculated guideline-based Primary Irritation Index (PII) was 0.0 (ie, the test item is classified as a nonskin irritant item under ISO-10993 international standard). Additionally, systemic clinical signs in reaction to treatment were not evident in any of the animals and unusual changes in body weight also were not noted.
Porcine safety study. In the porcine experiment, the weight of the pig remained the same during the 7-day study. No noticeable clinical signs of adverse effects in the pig were evident throughout the entire study period in reaction to treatment. Macroscopic examination of the wound sites revealed no significant differences between the control and test dressings in erythema, edema, and crust formation (Table 2) at 3 and 7 days post-wounding. Microscopic examination and histological analyses of the test site biopsies harvested 3 days post-wounding revealed no difference between the control and test dressings treatments at all test sites. A mild to moderate superficial inflammatory reaction was noted, while deeper layers exhibited normal histological patterns. Seven days post-wounding, the examined biopsies of dermal test sites exposed to both test item dressings (control and test dressings) demonstrated a “wet” eosinophilic phlegmonous dermatitis and granulomatous foreign body cell reaction to the same extent. All clinical pathology values obtained from the pre-treatment and 2 post-treatment collected blood samples were similar and fell well within the normal range (data not shown).
Skin sensitization. None of the animals exposed to the internal or exterior fabric of the test dressings showed any dermal reactions throughout the entire 72-hour observation period. There was no evidence of erythema, eschar, or edema formation. The calculated guideline-based Primary Irritation Index (PII) was 0.0 (ie, the test item is classified as a nonskin irritant item under ISO-10993 international standard). Additionally, systemic clinical signs in reaction to treatment were not evident in any of the animals and unusual changes in body weight also were not noted.
Porcine safety study. In the porcine experiment, the weight of the pig remained the same during the 7-day study. No noticeable clinical signs of adverse effects in the pig were evident throughout the entire study period in reaction to treatment. Macroscopic examination of the wound sites revealed no significant differences between the control and test dressings in erythema, edema, and crust formation (Table 2) at 3 and 7 days post-wounding. Microscopic examination and histological analyses of the test site biopsies harvested 3 days post-wounding revealed no difference between the control and test dressings treatments at all test sites. A mild to moderate superficial inflammatory reaction was noted, while deeper layers exhibited normal histological patterns. Seven days post-wounding, the examined biopsies of dermal test sites exposed to both test item dressings (control and test dressings) demonstrated a “wet” eosinophilic phlegmonous dermatitis and granulomatous foreign body cell reaction to the same extent. All clinical pathology values obtained from the pre-treatment and 2 post-treatment collected blood samples were similar and fell well within the normal range (data not shown).

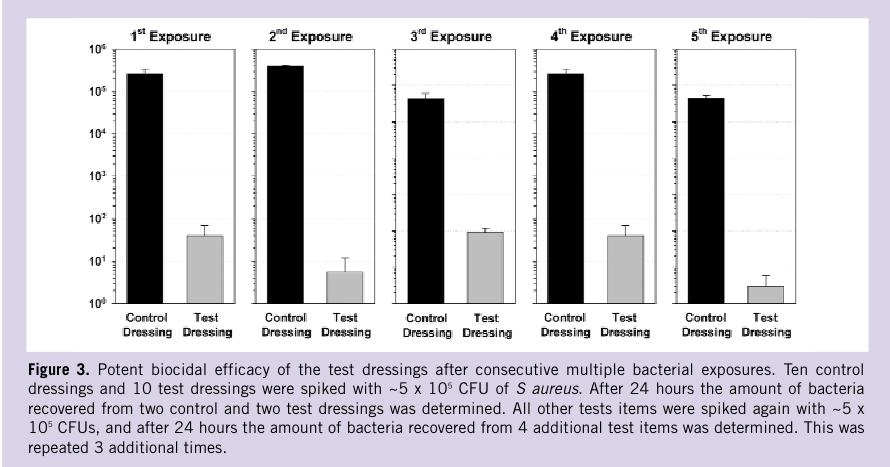
 The wound dressing has two layers: a highly absorbent internal fabric, which effectively absorbs exudate from a “moist” wound, and an external non-stick, non-woven fabric intended to allow simple and atraumatic removal following usage. The internal and external layers contain 2.3%–3% (w/w) copper oxide. This endows the dressing with potent antibacterial and antifungal properties, as summarized in Table 1 and as depicted in Figures 2 and 3, protecting it from contamination. The prolonged efficacy and high biocidal copper reservoir of the dressing is demonstrated by its capacity to reduce the microbial challenge by more than 3 logs even when spiked 5 consecutive times with a high bacterial titer (Figure 3). Notably, the wound dressing antimicrobial properties are exerted within minutes (Figure 2). This is in agreement with other studies, showing for example, that exposure of intact Saccharomyces cerevisiae to Cu2+ causes a loss of the permeability barrier of its plasma membranes within 2 minutes at 25˚C leading to loss of cell viability.35
A valid concern related to the repeated usage of antimicrobial agents in wound dressings is the development of microbial resistance to the active agents, in view of the rather high resistance developed to antibiotics and other agents by microbes in less than 50 years of their usage (see Introduction). However, in this respect, the use of copper should raise relatively low concern. The targets of many agents, including antibiotics, are very specific cell components, and development of resistance to these agents may thus occur via a particular mutation or a few mutations in that particular cell component. Copper ions, however, cause non-specific simultaneous damage to microorganisms via: A) denaturation of nucleic acids by binding to and/or disordering helical structures and/or by cross-linking between and within nucleic acid strands36,37; B) alteration of proteins and inhibition of their biological assembly and activity38,39; C) plasma membrane permeabilization35,40,41; and D) membrane lipid peroxidation.41–43 Some microorganisms have developed several mechanisms to tolerate excess concentrations of metal, including copper,40 and are thus less sensitive to copper than others.2 However, exposure of microorganisms including viruses, gram-positive and gram-negative bacteria, and fungi to high concentrations of copper ions, like those released by the wound dressings, results in simultaneous damage to many cellular components.1 Accordingly, the present study did not find any reduction in sensitivity by bacteria consecutively exposed to fabrics containing only 1% (w/w) copper oxide. It is not surprising that copper, despite its presence throughout human history and its historical use as an antimicrobial agent, remains a broad-spectrum biocidal/antimicrobial compound to which microbes have not been able to develop resistance.1
To allow the wound dressing to exert its potent biocidal properties not only against bacteria found in the dressing itself, but also against bacteria present within the wound, the copper oxide wound dressing was designed to be flexible with high conformability so as to easily adhere to all wound surfaces. This reduces to a minimum the formation of voids (dead spaces), where bacteria may flourish, thereby impeding successful wound healing.44 The close proximity of the copper oxide containing dressings and the wound surface allows for more efficacious copper ion release from the dressings into the dressing/wound interface. Additionally, the high absorbency and flexibility of the copper oxide dressing assures better sequestration of the bacteria by absorbing the exudates into the internal layers and reducing the bioburden in the wound. Sequestration of bacteria has been shown to be an important feature of wound dressings.45
Another obvious concern when using antimicrobial agents in wound dressings is their safety since antimicrobial agents exposed to open wounds can be systemically absorbed. For example, the concentration of silver, which is widely used as an antimicrobial agent in wound dressings due to its biocidal properties, can increase by more than 130 fold in plasma and urine of silver sulfadiazine cream-treated burn patients within 6 hours of exposure.46 Absorption can lead to toxicity and, indeed, renal toxicity from silver has been reported after topical application.47 Similarly, hepatic dysfunction was reported in patients with burns treated with silver dressings,48 although this was resolved after cessation of the silver treatment. In another recent study, accumulation of silver and delayed re-epithelialization in normal human skin when using different silver containing wound dressings has been reported.49 Furthermore, there is increased concern regarding the safety of silver use, and in particular nanosilver, in wound dressings and in medical devices in general.50 Nevertheless, the use of silver dressings is gaining popularity51 and is generally considered safe.
Copper, as opposed to silver, is an essential trace element needed for the normal function of many tissues, such as the integument, nervous and immune systems, and in general for the normal function of many metalloproteins, gene expression regulatory proteins, and many metabolic processes.11,52 Copper, unlike silver, is readily metabolized and utilized by the body when absorbed either orally or through tissues. Copper is stored bound to metallothionein, ceruloplasmin, amino acids, and in association with copper-dependent enzymes53,54; excess copper is readily secreted via feces (~72%) and urine.55–57 Contrary to the high susceptibility of microorganisms to copper, human skin is not sensitive to copper and the risk of adverse reactions due to dermal exposure to copper is extremely low.7,8 However, in wounds, especially in diabetic ulcers or pressure sores, where there is significant reduced blood supply to the wound, there is a danger of accumulation of the active substance in the wound, including of copper. Possible local toxicity due to copper accumulation and possible complications due to the use of the copper containing wound dressings, especially in patients who suffer from renal or liver malfunction, need to be addressed carefully in future clinical trials. In some cases, such as in severe burn wounds, copper deficiency in the wounds may occur due to systemic trace element imbalance.58,59 Since it has been found that systemic, prolonged high dosage delivery of copper may be deleterious, careful research is required regarding the use of the copper oxide impregnated wound dressing in burn wounds.
The present study investigated the safety of copper oxide containing dressings in animal models and found that the wound dressings did not cause any adverse reactions in closed skin, which is in accordance with previous studies where other fabrics with even higher concentrations of copper oxide were used.25 Importantly, as demonstrated in the porcine experiment, the copper oxide containing wound dressings did not differ from the control dressings in terms of local effects.
The wound dressing has two layers: a highly absorbent internal fabric, which effectively absorbs exudate from a “moist” wound, and an external non-stick, non-woven fabric intended to allow simple and atraumatic removal following usage. The internal and external layers contain 2.3%–3% (w/w) copper oxide. This endows the dressing with potent antibacterial and antifungal properties, as summarized in Table 1 and as depicted in Figures 2 and 3, protecting it from contamination. The prolonged efficacy and high biocidal copper reservoir of the dressing is demonstrated by its capacity to reduce the microbial challenge by more than 3 logs even when spiked 5 consecutive times with a high bacterial titer (Figure 3). Notably, the wound dressing antimicrobial properties are exerted within minutes (Figure 2). This is in agreement with other studies, showing for example, that exposure of intact Saccharomyces cerevisiae to Cu2+ causes a loss of the permeability barrier of its plasma membranes within 2 minutes at 25˚C leading to loss of cell viability.35
A valid concern related to the repeated usage of antimicrobial agents in wound dressings is the development of microbial resistance to the active agents, in view of the rather high resistance developed to antibiotics and other agents by microbes in less than 50 years of their usage (see Introduction). However, in this respect, the use of copper should raise relatively low concern. The targets of many agents, including antibiotics, are very specific cell components, and development of resistance to these agents may thus occur via a particular mutation or a few mutations in that particular cell component. Copper ions, however, cause non-specific simultaneous damage to microorganisms via: A) denaturation of nucleic acids by binding to and/or disordering helical structures and/or by cross-linking between and within nucleic acid strands36,37; B) alteration of proteins and inhibition of their biological assembly and activity38,39; C) plasma membrane permeabilization35,40,41; and D) membrane lipid peroxidation.41–43 Some microorganisms have developed several mechanisms to tolerate excess concentrations of metal, including copper,40 and are thus less sensitive to copper than others.2 However, exposure of microorganisms including viruses, gram-positive and gram-negative bacteria, and fungi to high concentrations of copper ions, like those released by the wound dressings, results in simultaneous damage to many cellular components.1 Accordingly, the present study did not find any reduction in sensitivity by bacteria consecutively exposed to fabrics containing only 1% (w/w) copper oxide. It is not surprising that copper, despite its presence throughout human history and its historical use as an antimicrobial agent, remains a broad-spectrum biocidal/antimicrobial compound to which microbes have not been able to develop resistance.1
To allow the wound dressing to exert its potent biocidal properties not only against bacteria found in the dressing itself, but also against bacteria present within the wound, the copper oxide wound dressing was designed to be flexible with high conformability so as to easily adhere to all wound surfaces. This reduces to a minimum the formation of voids (dead spaces), where bacteria may flourish, thereby impeding successful wound healing.44 The close proximity of the copper oxide containing dressings and the wound surface allows for more efficacious copper ion release from the dressings into the dressing/wound interface. Additionally, the high absorbency and flexibility of the copper oxide dressing assures better sequestration of the bacteria by absorbing the exudates into the internal layers and reducing the bioburden in the wound. Sequestration of bacteria has been shown to be an important feature of wound dressings.45
Another obvious concern when using antimicrobial agents in wound dressings is their safety since antimicrobial agents exposed to open wounds can be systemically absorbed. For example, the concentration of silver, which is widely used as an antimicrobial agent in wound dressings due to its biocidal properties, can increase by more than 130 fold in plasma and urine of silver sulfadiazine cream-treated burn patients within 6 hours of exposure.46 Absorption can lead to toxicity and, indeed, renal toxicity from silver has been reported after topical application.47 Similarly, hepatic dysfunction was reported in patients with burns treated with silver dressings,48 although this was resolved after cessation of the silver treatment. In another recent study, accumulation of silver and delayed re-epithelialization in normal human skin when using different silver containing wound dressings has been reported.49 Furthermore, there is increased concern regarding the safety of silver use, and in particular nanosilver, in wound dressings and in medical devices in general.50 Nevertheless, the use of silver dressings is gaining popularity51 and is generally considered safe.
Copper, as opposed to silver, is an essential trace element needed for the normal function of many tissues, such as the integument, nervous and immune systems, and in general for the normal function of many metalloproteins, gene expression regulatory proteins, and many metabolic processes.11,52 Copper, unlike silver, is readily metabolized and utilized by the body when absorbed either orally or through tissues. Copper is stored bound to metallothionein, ceruloplasmin, amino acids, and in association with copper-dependent enzymes53,54; excess copper is readily secreted via feces (~72%) and urine.55–57 Contrary to the high susceptibility of microorganisms to copper, human skin is not sensitive to copper and the risk of adverse reactions due to dermal exposure to copper is extremely low.7,8 However, in wounds, especially in diabetic ulcers or pressure sores, where there is significant reduced blood supply to the wound, there is a danger of accumulation of the active substance in the wound, including of copper. Possible local toxicity due to copper accumulation and possible complications due to the use of the copper containing wound dressings, especially in patients who suffer from renal or liver malfunction, need to be addressed carefully in future clinical trials. In some cases, such as in severe burn wounds, copper deficiency in the wounds may occur due to systemic trace element imbalance.58,59 Since it has been found that systemic, prolonged high dosage delivery of copper may be deleterious, careful research is required regarding the use of the copper oxide impregnated wound dressing in burn wounds.
The present study investigated the safety of copper oxide containing dressings in animal models and found that the wound dressings did not cause any adverse reactions in closed skin, which is in accordance with previous studies where other fabrics with even higher concentrations of copper oxide were used.25 Importantly, as demonstrated in the porcine experiment, the copper oxide containing wound dressings did not differ from the control dressings in terms of local effects.
Materials and Methods
Test dressings. A recently developed technology that introduces copper oxide into fibers30,31 was used to make the copper oxide containing nonstick dressing pads (Figure 1; hereafter referred to as “test dressings”). The test dressings contain an internal, highly absorbent (165 µL/cm2 = 165 µL/10 mg) needle punch fabric made of viscose/rayon (Galaxy®, Kelheim Fibers, GmbH, Germany) fibers of 1.4 denier and 38 mm in length and 3% of cellulose copper oxide plated fibers (Figure 1). The internal layer is enveloped with an external hydrophobic treated spun bond layer made of polypropylene fibers impregnated with 2.3% weight/weight (w/w) copper oxide particles (Figure 1). The fibers were examined by scanning electron microscopy (SEM) and the presence of copper was determined by x-ray photoelectron spectrum analysis, as shown in Figure 1.
Determination of antibacterial and antifungal properties. The antibacterial and antifungal properties of the internal and envelope layers of the test dressings were determined according to the American Association of Textile Chemists and Colorists (AATCC) Test Method 100-1993. Briefly, sterile swatches weighing 0.50 g ± 0.01 g of the copper containing fabrics and of similar fabrics without copper (control fabrics) were placed in sterile vials and exposed to 0.5 mL saline solution containing 1 x 105 to 4 x 106 colony forming units (CFUs). The spiked samples were then incubated at room temperature for 4 hours unless otherwise specified. After the incubation period, the test samples were transferred aseptically to Stomager bags containing 100 mL of saline solution and 0.1% of Tween 80 (wash buffer). The bags were then shaken vigorously for 2 minutes. Aliquots of 0.1 mL, 1 mL, and 10 mL of the liquid from each bag were then added to the wash buffer to a final volume of 20 mL. The 20-mL samples were then passed through a 0.45-µm membrane using a vacuum pump and a Gelman/Pall filtration device. The membranes containing the bacteria/fungi were washed with 50 mL of wash buffer and then placed in Petri dishes containing selective culture media. The plates were incubated at 35˚C ± 1˚C for 24 hours and the number of bacterial or fungi colonies were counted. Tests in which the incubation time was minutes, 10 mL of sterile standard DE (Dey/Engley) Neutralizing Broth was added to the spiked samples in order to neutralize antimicrobial activity. The log reduction of bacterial or fungal titers was calculated with the following formula: Log A – Log B = Log R to the nearest hundred, where R = reduction; A = population of the challenge organism; B = the number of test organisms recovered from the inoculated test sample. The test organisms studied were: Escherichia coli (ATCC # 8739); Klebsiella pneumoniae (ATCC# 13883); Enterococcus fecalis (ATCC 29212); Pseudomonas aeruginosa (ATCC 9027); Staphylococcus aureus (ATCC 6538); and Candida albicans (ATCC 10231).
The fibers were examined by scanning electron microscopy (SEM) and the presence of copper was determined by x-ray photoelectron spectrum analysis, as shown in Figure 1.
Determination of antibacterial and antifungal properties. The antibacterial and antifungal properties of the internal and envelope layers of the test dressings were determined according to the American Association of Textile Chemists and Colorists (AATCC) Test Method 100-1993. Briefly, sterile swatches weighing 0.50 g ± 0.01 g of the copper containing fabrics and of similar fabrics without copper (control fabrics) were placed in sterile vials and exposed to 0.5 mL saline solution containing 1 x 105 to 4 x 106 colony forming units (CFUs). The spiked samples were then incubated at room temperature for 4 hours unless otherwise specified. After the incubation period, the test samples were transferred aseptically to Stomager bags containing 100 mL of saline solution and 0.1% of Tween 80 (wash buffer). The bags were then shaken vigorously for 2 minutes. Aliquots of 0.1 mL, 1 mL, and 10 mL of the liquid from each bag were then added to the wash buffer to a final volume of 20 mL. The 20-mL samples were then passed through a 0.45-µm membrane using a vacuum pump and a Gelman/Pall filtration device. The membranes containing the bacteria/fungi were washed with 50 mL of wash buffer and then placed in Petri dishes containing selective culture media. The plates were incubated at 35˚C ± 1˚C for 24 hours and the number of bacterial or fungi colonies were counted. Tests in which the incubation time was minutes, 10 mL of sterile standard DE (Dey/Engley) Neutralizing Broth was added to the spiked samples in order to neutralize antimicrobial activity. The log reduction of bacterial or fungal titers was calculated with the following formula: Log A – Log B = Log R to the nearest hundred, where R = reduction; A = population of the challenge organism; B = the number of test organisms recovered from the inoculated test sample. The test organisms studied were: Escherichia coli (ATCC # 8739); Klebsiella pneumoniae (ATCC# 13883); Enterococcus fecalis (ATCC 29212); Pseudomonas aeruginosa (ATCC 9027); Staphylococcus aureus (ATCC 6538); and Candida albicans (ATCC 10231).
 In addition to the viability tests, a highly sensitive CheckLight ToxScreen Kit (CheckLight Ltd, Qiryat-Tivon, Israel) was used to determine the biocidal efficacy of the control and test items. The assay is based on the luminescence emitted by the marine bacterium Photobacterium leiognathi. The reduction of the bacteria luminescence is correlated with the bacteria viability, which can be measured within minutes of the bacterial exposure to the test items or liquid that came into contact with the test items. The assay was performed according to manufacturer’s instructions. Briefly, a 1.5-mL buffer supplied with the kit was added to 1 cm2 of the control or test item. After 1 minute of vigorous mixing, 1 mL of each mix was withdrawn into a fresh tube containing the bacteria. The tubes were incubated at 27˚C for 10–30 minutes, during which aliquots were withdrawn and the luminescence was determined using a luminometer with a spectral sensitivity range of 380 nm–630 nm. Negative (buffer only) and positive controls (1:100 dilution of a copper chloride solution provided in the kit in buffer) were included and the light level emitted by the test items was compared to that emitted by the positive and negative controls.
Rabbit skin sensitization test. The potential dermal irritation and delayed-type hypersensitivity of the spun-bond polypropylene and of the copper plated cellulosic fibers that comprise the test dressings and contain 2.3% and 3% copper oxide (w/w), respectively, were assessed in 6 Hsdlf:NZW rabbits (3 and 3, respectively) according to the International Standard (ISO 10993-10:2002). An independent laboratory (Harlan Biotech Israel, Ltd.) performed the test under GLP procedures. Briefly, two sites in each animal served as test sites and two others as control sites. Approximately 24 hours before the test, fur was removed by closely clipping a sufficient distance on both sides of the spine for application and observations of all sites (approx. 10 cm × 15 cm). Care was taken to avoid abrading the skin, and only animals with healthy, intact skin were used. Following application, each test site or control site was dressed for a total of 4 hours. At the end of the contact time, the dressings were removed and the positions of the patches were re-marked. Dermal reactions for erythema, eschar, and edema formation were scored according to the test guidelines and recorded at the standard time points of 1, 24, 48, and 72 hours after dressing removal.
In addition to the viability tests, a highly sensitive CheckLight ToxScreen Kit (CheckLight Ltd, Qiryat-Tivon, Israel) was used to determine the biocidal efficacy of the control and test items. The assay is based on the luminescence emitted by the marine bacterium Photobacterium leiognathi. The reduction of the bacteria luminescence is correlated with the bacteria viability, which can be measured within minutes of the bacterial exposure to the test items or liquid that came into contact with the test items. The assay was performed according to manufacturer’s instructions. Briefly, a 1.5-mL buffer supplied with the kit was added to 1 cm2 of the control or test item. After 1 minute of vigorous mixing, 1 mL of each mix was withdrawn into a fresh tube containing the bacteria. The tubes were incubated at 27˚C for 10–30 minutes, during which aliquots were withdrawn and the luminescence was determined using a luminometer with a spectral sensitivity range of 380 nm–630 nm. Negative (buffer only) and positive controls (1:100 dilution of a copper chloride solution provided in the kit in buffer) were included and the light level emitted by the test items was compared to that emitted by the positive and negative controls.
Rabbit skin sensitization test. The potential dermal irritation and delayed-type hypersensitivity of the spun-bond polypropylene and of the copper plated cellulosic fibers that comprise the test dressings and contain 2.3% and 3% copper oxide (w/w), respectively, were assessed in 6 Hsdlf:NZW rabbits (3 and 3, respectively) according to the International Standard (ISO 10993-10:2002). An independent laboratory (Harlan Biotech Israel, Ltd.) performed the test under GLP procedures. Briefly, two sites in each animal served as test sites and two others as control sites. Approximately 24 hours before the test, fur was removed by closely clipping a sufficient distance on both sides of the spine for application and observations of all sites (approx. 10 cm × 15 cm). Care was taken to avoid abrading the skin, and only animals with healthy, intact skin were used. Following application, each test site or control site was dressed for a total of 4 hours. At the end of the contact time, the dressings were removed and the positions of the patches were re-marked. Dermal reactions for erythema, eschar, and edema formation were scored according to the test guidelines and recorded at the standard time points of 1, 24, 48, and 72 hours after dressing removal.
 Porcine partial-thickness wound model. The skin of pigs is considered the closest model to human skin in terms of the anatomical and physiological characteristics of skin.32 We therefore examined possible adverse effects of applying the test dressings on wounds by using a porcine partial-thickness wound model. An independent laboratory (Harlan Biotech Israel, Ltd.) performed this experiment using a large, white, Landrace female pig weighing ~50 kg. Test sites comprised a total of 12 evenly bilateral allocated punch biopsy partial-thickness wounds each measuring approximately 12 mm in diameter and 5 mm in depth. Immediately after wounding, six randomly chosen wounds were covered with test dressings and the remaining 6 wounds with control commercial sterile dressing pads (hereafter referred to as control dressings). Comparable assessments of the test dressing and control dressing covered wound sites at day 3 and day 7 post-wounding were conducted by macroscopic examination and scoring of local dermal reactions (erythema, edema, and crust formation), and by microscopic examination following biopsy harvest. In addition to assessing the direct effects at the wound sites, blood samples were collected at the pre-test stage (baseline control) and at the time of the two respective biopsy harvest sessions on study days 3 and 7 post-wounding to resolve any potential treatment effects on clinical pathology parameters.
Porcine partial-thickness wound model. The skin of pigs is considered the closest model to human skin in terms of the anatomical and physiological characteristics of skin.32 We therefore examined possible adverse effects of applying the test dressings on wounds by using a porcine partial-thickness wound model. An independent laboratory (Harlan Biotech Israel, Ltd.) performed this experiment using a large, white, Landrace female pig weighing ~50 kg. Test sites comprised a total of 12 evenly bilateral allocated punch biopsy partial-thickness wounds each measuring approximately 12 mm in diameter and 5 mm in depth. Immediately after wounding, six randomly chosen wounds were covered with test dressings and the remaining 6 wounds with control commercial sterile dressing pads (hereafter referred to as control dressings). Comparable assessments of the test dressing and control dressing covered wound sites at day 3 and day 7 post-wounding were conducted by macroscopic examination and scoring of local dermal reactions (erythema, edema, and crust formation), and by microscopic examination following biopsy harvest. In addition to assessing the direct effects at the wound sites, blood samples were collected at the pre-test stage (baseline control) and at the time of the two respective biopsy harvest sessions on study days 3 and 7 post-wounding to resolve any potential treatment effects on clinical pathology parameters.
Results
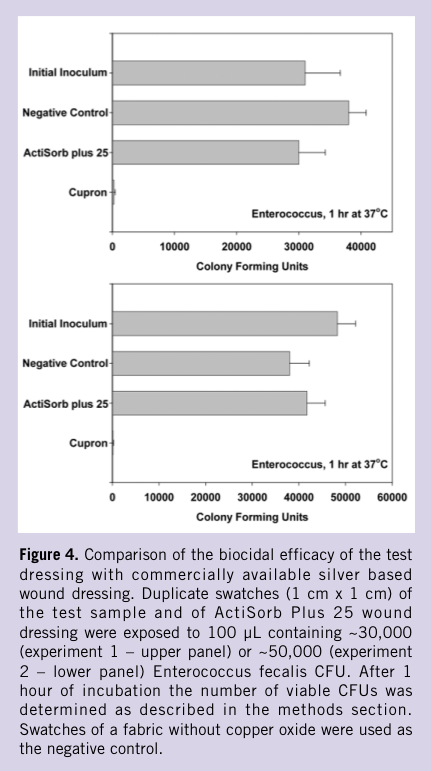
Antibacterial and antifungal efficacies of test dressings. Both the envelope fabric (2.3% copper oxide impregnated polypropylene nonwoven fabric) and the internal fabric (containing 3% copper oxide plated fibers) of the test dressings have potent antibacterial (gram-positive and gram-negative bacteria) and antifungal properties (Table 1). The damage to microorganisms is exerted within minutes of their exposure to the copper oxide containing fabrics (Figure 2). The test dressings exerted similar potent biocidal efficacy when repeatedly spiked for 5 consecutive days with high titers of bacteria (Figure 3). When the biocidal efficacy against Enterococcus faecalis of the test dressing was compared in two separate experiments with a popular silver containing wound dressing (ActiSorb Plus 25®, Johnson & Johnson Medical, Gargrave, Skipton, UK), it performed significantly better (Figure 4). Importantly, in separate experiments, in which E coli, S aureus, or K pneumoniae were exposed to fabrics containing only 1% copper oxide (one third of the amount found in the test dressings) for 24 hours with 2 log of the bacteria killed, the surviving bacteria that were propagated and re-exposed again for 5 consecutive times to the 1% copper oxide containing fabrics, were as sensitive to the fabrics as their “parent” bacteria. At least 2 log of the bacteria were killed in each of the consecutive exposures, without development of tolerance.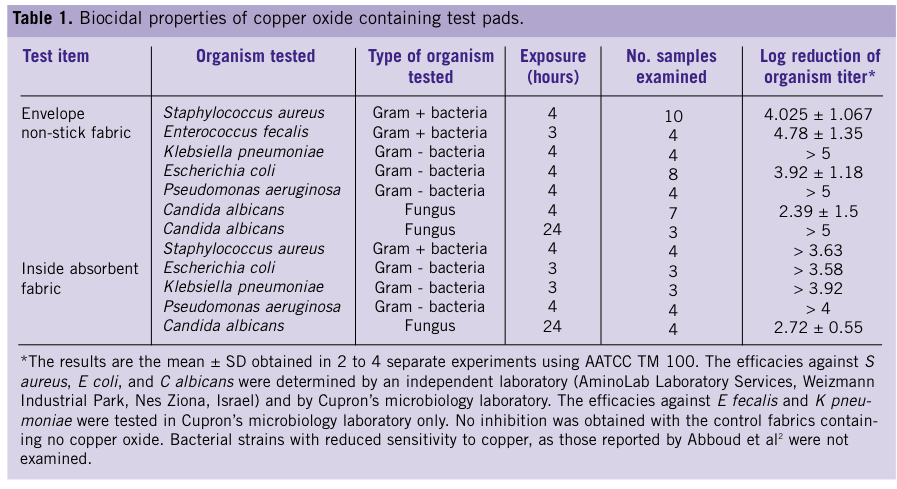 Skin sensitization. None of the animals exposed to the internal or exterior fabric of the test dressings showed any dermal reactions throughout the entire 72-hour observation period. There was no evidence of erythema, eschar, or edema formation. The calculated guideline-based Primary Irritation Index (PII) was 0.0 (ie, the test item is classified as a nonskin irritant item under ISO-10993 international standard). Additionally, systemic clinical signs in reaction to treatment were not evident in any of the animals and unusual changes in body weight also were not noted.
Porcine safety study. In the porcine experiment, the weight of the pig remained the same during the 7-day study. No noticeable clinical signs of adverse effects in the pig were evident throughout the entire study period in reaction to treatment. Macroscopic examination of the wound sites revealed no significant differences between the control and test dressings in erythema, edema, and crust formation (Table 2) at 3 and 7 days post-wounding. Microscopic examination and histological analyses of the test site biopsies harvested 3 days post-wounding revealed no difference between the control and test dressings treatments at all test sites. A mild to moderate superficial inflammatory reaction was noted, while deeper layers exhibited normal histological patterns. Seven days post-wounding, the examined biopsies of dermal test sites exposed to both test item dressings (control and test dressings) demonstrated a “wet” eosinophilic phlegmonous dermatitis and granulomatous foreign body cell reaction to the same extent. All clinical pathology values obtained from the pre-treatment and 2 post-treatment collected blood samples were similar and fell well within the normal range (data not shown).
Skin sensitization. None of the animals exposed to the internal or exterior fabric of the test dressings showed any dermal reactions throughout the entire 72-hour observation period. There was no evidence of erythema, eschar, or edema formation. The calculated guideline-based Primary Irritation Index (PII) was 0.0 (ie, the test item is classified as a nonskin irritant item under ISO-10993 international standard). Additionally, systemic clinical signs in reaction to treatment were not evident in any of the animals and unusual changes in body weight also were not noted.
Porcine safety study. In the porcine experiment, the weight of the pig remained the same during the 7-day study. No noticeable clinical signs of adverse effects in the pig were evident throughout the entire study period in reaction to treatment. Macroscopic examination of the wound sites revealed no significant differences between the control and test dressings in erythema, edema, and crust formation (Table 2) at 3 and 7 days post-wounding. Microscopic examination and histological analyses of the test site biopsies harvested 3 days post-wounding revealed no difference between the control and test dressings treatments at all test sites. A mild to moderate superficial inflammatory reaction was noted, while deeper layers exhibited normal histological patterns. Seven days post-wounding, the examined biopsies of dermal test sites exposed to both test item dressings (control and test dressings) demonstrated a “wet” eosinophilic phlegmonous dermatitis and granulomatous foreign body cell reaction to the same extent. All clinical pathology values obtained from the pre-treatment and 2 post-treatment collected blood samples were similar and fell well within the normal range (data not shown).
Discussion
Wounds with compromised circulation to the wound site, such as venous leg ulcers, diabetic foot ulcers, and decubitus wounds, can often be effectively treated by basic approaches such as controlling infection, maintaining a clean wound, and keeping pressure offloaded.33 However, roughly a third of these wounds fail to heal, dictating the need for a more active approach. Copper plays a key role in many of the processes that together comprise wound healing, including induction of endothelial growth factor, angiogenesis, and expression and stabilization of extracellular skin proteins. Thus, we recently hypothesized that part of the incapacity to heal chronic wounds, which might have compromised circulation to the wound site, may be attributed to low local copper levels.28 Importantly, copper has potent broad biocidal properties1 and contamination of wounds is an important contributing factor to impaired wound healing.27,33 The authors hypothesized that introducing copper into wound dressings would not only reduce the risk of wound and dressing contamination, but more importantly, would directly stimulate faster wound repair.28 This would be done by the release of copper from the wound dressings directly into the wound site inducing angiogenesis and skin regeneration. The present study analyzed the copper dressing’s in-vitro biocidal properties and safety in animal models. Their capacity to enhance wound closure, increase gene and in-situ upregulation of proangiogenic factors (eg, placental growth factor and VEGF), and increase blood vessel formation when compared to control dressings (without copper) or commercial wound dressings containing silver in wounds inflicted in genetically engineered diabetic mice, is reported elsewhere.29 Copper oxide was incorporated into the dressings since it is the most common naturally occurring form of copper and copper oxide is both non-soluble and a very powerful biocide. These properties allow a very slow and steady release of copper ions,34 which permit an increased shelf life of the wound dressings, and more significantly, increased capacity of the wound dressing for prolonged and stable biocidal and wound healing properties.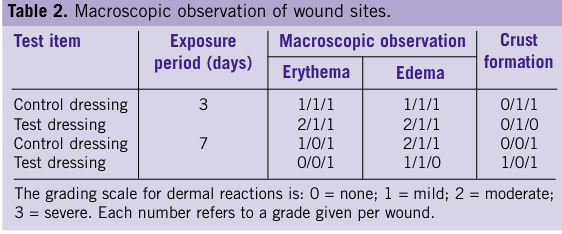 The wound dressing has two layers: a highly absorbent internal fabric, which effectively absorbs exudate from a “moist” wound, and an external non-stick, non-woven fabric intended to allow simple and atraumatic removal following usage. The internal and external layers contain 2.3%–3% (w/w) copper oxide. This endows the dressing with potent antibacterial and antifungal properties, as summarized in Table 1 and as depicted in Figures 2 and 3, protecting it from contamination. The prolonged efficacy and high biocidal copper reservoir of the dressing is demonstrated by its capacity to reduce the microbial challenge by more than 3 logs even when spiked 5 consecutive times with a high bacterial titer (Figure 3). Notably, the wound dressing antimicrobial properties are exerted within minutes (Figure 2). This is in agreement with other studies, showing for example, that exposure of intact Saccharomyces cerevisiae to Cu2+ causes a loss of the permeability barrier of its plasma membranes within 2 minutes at 25˚C leading to loss of cell viability.35
A valid concern related to the repeated usage of antimicrobial agents in wound dressings is the development of microbial resistance to the active agents, in view of the rather high resistance developed to antibiotics and other agents by microbes in less than 50 years of their usage (see Introduction). However, in this respect, the use of copper should raise relatively low concern. The targets of many agents, including antibiotics, are very specific cell components, and development of resistance to these agents may thus occur via a particular mutation or a few mutations in that particular cell component. Copper ions, however, cause non-specific simultaneous damage to microorganisms via: A) denaturation of nucleic acids by binding to and/or disordering helical structures and/or by cross-linking between and within nucleic acid strands36,37; B) alteration of proteins and inhibition of their biological assembly and activity38,39; C) plasma membrane permeabilization35,40,41; and D) membrane lipid peroxidation.41–43 Some microorganisms have developed several mechanisms to tolerate excess concentrations of metal, including copper,40 and are thus less sensitive to copper than others.2 However, exposure of microorganisms including viruses, gram-positive and gram-negative bacteria, and fungi to high concentrations of copper ions, like those released by the wound dressings, results in simultaneous damage to many cellular components.1 Accordingly, the present study did not find any reduction in sensitivity by bacteria consecutively exposed to fabrics containing only 1% (w/w) copper oxide. It is not surprising that copper, despite its presence throughout human history and its historical use as an antimicrobial agent, remains a broad-spectrum biocidal/antimicrobial compound to which microbes have not been able to develop resistance.1
To allow the wound dressing to exert its potent biocidal properties not only against bacteria found in the dressing itself, but also against bacteria present within the wound, the copper oxide wound dressing was designed to be flexible with high conformability so as to easily adhere to all wound surfaces. This reduces to a minimum the formation of voids (dead spaces), where bacteria may flourish, thereby impeding successful wound healing.44 The close proximity of the copper oxide containing dressings and the wound surface allows for more efficacious copper ion release from the dressings into the dressing/wound interface. Additionally, the high absorbency and flexibility of the copper oxide dressing assures better sequestration of the bacteria by absorbing the exudates into the internal layers and reducing the bioburden in the wound. Sequestration of bacteria has been shown to be an important feature of wound dressings.45
Another obvious concern when using antimicrobial agents in wound dressings is their safety since antimicrobial agents exposed to open wounds can be systemically absorbed. For example, the concentration of silver, which is widely used as an antimicrobial agent in wound dressings due to its biocidal properties, can increase by more than 130 fold in plasma and urine of silver sulfadiazine cream-treated burn patients within 6 hours of exposure.46 Absorption can lead to toxicity and, indeed, renal toxicity from silver has been reported after topical application.47 Similarly, hepatic dysfunction was reported in patients with burns treated with silver dressings,48 although this was resolved after cessation of the silver treatment. In another recent study, accumulation of silver and delayed re-epithelialization in normal human skin when using different silver containing wound dressings has been reported.49 Furthermore, there is increased concern regarding the safety of silver use, and in particular nanosilver, in wound dressings and in medical devices in general.50 Nevertheless, the use of silver dressings is gaining popularity51 and is generally considered safe.
Copper, as opposed to silver, is an essential trace element needed for the normal function of many tissues, such as the integument, nervous and immune systems, and in general for the normal function of many metalloproteins, gene expression regulatory proteins, and many metabolic processes.11,52 Copper, unlike silver, is readily metabolized and utilized by the body when absorbed either orally or through tissues. Copper is stored bound to metallothionein, ceruloplasmin, amino acids, and in association with copper-dependent enzymes53,54; excess copper is readily secreted via feces (~72%) and urine.55–57 Contrary to the high susceptibility of microorganisms to copper, human skin is not sensitive to copper and the risk of adverse reactions due to dermal exposure to copper is extremely low.7,8 However, in wounds, especially in diabetic ulcers or pressure sores, where there is significant reduced blood supply to the wound, there is a danger of accumulation of the active substance in the wound, including of copper. Possible local toxicity due to copper accumulation and possible complications due to the use of the copper containing wound dressings, especially in patients who suffer from renal or liver malfunction, need to be addressed carefully in future clinical trials. In some cases, such as in severe burn wounds, copper deficiency in the wounds may occur due to systemic trace element imbalance.58,59 Since it has been found that systemic, prolonged high dosage delivery of copper may be deleterious, careful research is required regarding the use of the copper oxide impregnated wound dressing in burn wounds.
The present study investigated the safety of copper oxide containing dressings in animal models and found that the wound dressings did not cause any adverse reactions in closed skin, which is in accordance with previous studies where other fabrics with even higher concentrations of copper oxide were used.25 Importantly, as demonstrated in the porcine experiment, the copper oxide containing wound dressings did not differ from the control dressings in terms of local effects.
The wound dressing has two layers: a highly absorbent internal fabric, which effectively absorbs exudate from a “moist” wound, and an external non-stick, non-woven fabric intended to allow simple and atraumatic removal following usage. The internal and external layers contain 2.3%–3% (w/w) copper oxide. This endows the dressing with potent antibacterial and antifungal properties, as summarized in Table 1 and as depicted in Figures 2 and 3, protecting it from contamination. The prolonged efficacy and high biocidal copper reservoir of the dressing is demonstrated by its capacity to reduce the microbial challenge by more than 3 logs even when spiked 5 consecutive times with a high bacterial titer (Figure 3). Notably, the wound dressing antimicrobial properties are exerted within minutes (Figure 2). This is in agreement with other studies, showing for example, that exposure of intact Saccharomyces cerevisiae to Cu2+ causes a loss of the permeability barrier of its plasma membranes within 2 minutes at 25˚C leading to loss of cell viability.35
A valid concern related to the repeated usage of antimicrobial agents in wound dressings is the development of microbial resistance to the active agents, in view of the rather high resistance developed to antibiotics and other agents by microbes in less than 50 years of their usage (see Introduction). However, in this respect, the use of copper should raise relatively low concern. The targets of many agents, including antibiotics, are very specific cell components, and development of resistance to these agents may thus occur via a particular mutation or a few mutations in that particular cell component. Copper ions, however, cause non-specific simultaneous damage to microorganisms via: A) denaturation of nucleic acids by binding to and/or disordering helical structures and/or by cross-linking between and within nucleic acid strands36,37; B) alteration of proteins and inhibition of their biological assembly and activity38,39; C) plasma membrane permeabilization35,40,41; and D) membrane lipid peroxidation.41–43 Some microorganisms have developed several mechanisms to tolerate excess concentrations of metal, including copper,40 and are thus less sensitive to copper than others.2 However, exposure of microorganisms including viruses, gram-positive and gram-negative bacteria, and fungi to high concentrations of copper ions, like those released by the wound dressings, results in simultaneous damage to many cellular components.1 Accordingly, the present study did not find any reduction in sensitivity by bacteria consecutively exposed to fabrics containing only 1% (w/w) copper oxide. It is not surprising that copper, despite its presence throughout human history and its historical use as an antimicrobial agent, remains a broad-spectrum biocidal/antimicrobial compound to which microbes have not been able to develop resistance.1
To allow the wound dressing to exert its potent biocidal properties not only against bacteria found in the dressing itself, but also against bacteria present within the wound, the copper oxide wound dressing was designed to be flexible with high conformability so as to easily adhere to all wound surfaces. This reduces to a minimum the formation of voids (dead spaces), where bacteria may flourish, thereby impeding successful wound healing.44 The close proximity of the copper oxide containing dressings and the wound surface allows for more efficacious copper ion release from the dressings into the dressing/wound interface. Additionally, the high absorbency and flexibility of the copper oxide dressing assures better sequestration of the bacteria by absorbing the exudates into the internal layers and reducing the bioburden in the wound. Sequestration of bacteria has been shown to be an important feature of wound dressings.45
Another obvious concern when using antimicrobial agents in wound dressings is their safety since antimicrobial agents exposed to open wounds can be systemically absorbed. For example, the concentration of silver, which is widely used as an antimicrobial agent in wound dressings due to its biocidal properties, can increase by more than 130 fold in plasma and urine of silver sulfadiazine cream-treated burn patients within 6 hours of exposure.46 Absorption can lead to toxicity and, indeed, renal toxicity from silver has been reported after topical application.47 Similarly, hepatic dysfunction was reported in patients with burns treated with silver dressings,48 although this was resolved after cessation of the silver treatment. In another recent study, accumulation of silver and delayed re-epithelialization in normal human skin when using different silver containing wound dressings has been reported.49 Furthermore, there is increased concern regarding the safety of silver use, and in particular nanosilver, in wound dressings and in medical devices in general.50 Nevertheless, the use of silver dressings is gaining popularity51 and is generally considered safe.
Copper, as opposed to silver, is an essential trace element needed for the normal function of many tissues, such as the integument, nervous and immune systems, and in general for the normal function of many metalloproteins, gene expression regulatory proteins, and many metabolic processes.11,52 Copper, unlike silver, is readily metabolized and utilized by the body when absorbed either orally or through tissues. Copper is stored bound to metallothionein, ceruloplasmin, amino acids, and in association with copper-dependent enzymes53,54; excess copper is readily secreted via feces (~72%) and urine.55–57 Contrary to the high susceptibility of microorganisms to copper, human skin is not sensitive to copper and the risk of adverse reactions due to dermal exposure to copper is extremely low.7,8 However, in wounds, especially in diabetic ulcers or pressure sores, where there is significant reduced blood supply to the wound, there is a danger of accumulation of the active substance in the wound, including of copper. Possible local toxicity due to copper accumulation and possible complications due to the use of the copper containing wound dressings, especially in patients who suffer from renal or liver malfunction, need to be addressed carefully in future clinical trials. In some cases, such as in severe burn wounds, copper deficiency in the wounds may occur due to systemic trace element imbalance.58,59 Since it has been found that systemic, prolonged high dosage delivery of copper may be deleterious, careful research is required regarding the use of the copper oxide impregnated wound dressing in burn wounds.
The present study investigated the safety of copper oxide containing dressings in animal models and found that the wound dressings did not cause any adverse reactions in closed skin, which is in accordance with previous studies where other fabrics with even higher concentrations of copper oxide were used.25 Importantly, as demonstrated in the porcine experiment, the copper oxide containing wound dressings did not differ from the control dressings in terms of local effects.






