



Leg Skin Ulcer With Atypical Features: Vascular Wound or Advanced Melanoma?
© 2024 HMP Global. All Rights Reserved.
Any views and opinions expressed are those of the author(s) and/or participants and do not necessarily reflect the views, policy, or position of Wounds or HMP Global, their employees, and affiliates.
Abstract
Background. Leg ulcers have various etiologies, including malignancy, although vascular issues are the most frequent cause. Malignant wounds present diagnostic challenges, with a reported prevalence rate ranging from 0.4% to 23%. This significant variability in reported prevalence appears to be due to the different settings in which data are collected, which suggests potential influence by medical specialty. Consequently, the misdiagnosis of neoplastic ulcers (eg, ulcerated melanoma) as vascular wounds is relatively common, leading to delayed diagnosis, inadequate treatment, and a dramatic worsening of the patient’s prognosis. Identifying malignancy in nonresponsive wounds involves recognizing signs such as hypertrophic granulation tissue, bleeding, unusual pigmentation, and raised edges. The appearance of the perilesional skin, together with dermoscopic observation, is also crucial to differentiation. Ultimately, a biopsy may provide valuable diagnostic clarification. Case Report. A case is presented of lower limb melanoma that for years was misdiagnosed as a vascular wound by multiple specialists, with delayed referral to a dermatologist and resulting recognition and diagnosis, at which time nodular satellite metastases were found. Dermoscopy and biopsy confirmed the diagnosis. The disease was already advanced, with in-transit and distant site metastases, and the prognosis was regrettably poor. Conclusion. This case underscores the importance of early detection and accurate diagnosis of malignant wounds, emphasizing the need to refer patients with suspicious nonresponsive ulcers to a dermatologist.
Introduction
Chronic leg wounds have several etiologies, and vascular genesis is commonly noted to be the most prevalent.1 Other frequent etiologies of such wounds are diabetes, trauma, and prolonged pressure; together with vascular issues, these etiologies account for approximately 95% of chronic leg wounds. The remaining 5% of etiologies are numerous and different, including but not limited to inflammatory, infectious, neoplastic, and drug-related.2 The reported prevalence of malignant wounds varies considerably, from 0.4% to 23%, based on data collection setting, which suggests that diagnosis may be influenced by the specialty area of the physician conducting the evaluation.3,4 In a previous retrospective study conducted at the Dermatologic Clinic of Spedali Civili in Brescia, Italy, in 2022, which analyzed the etiology of the dermatological case history of lower limb ulcers from 2010 through 2019, the prevalence of malignant wounds was found to be 3.2%.2 This contrasts with a vascular surgery report in which neoplastic wounds were deemed rare, with a prevalence of 0.4%.3
Many skin neoplasms can masquerade as ulcers, especially those located on the lower limbs.4,5 When discussing malignant wounds, it is essential to differentiate between 2 scenarios—1 involving structural damage of the skin and possibly deeper tissues as a result of a primary malignant or metastatic event, and the other involving the secondary transformation of a preexisting wound with a different primary cause (eg, Marjolin ulcer).4-7 Among the most common lower extremity skin malignancies are nodular basal cell carcinoma, squamous cell carcinoma, Kaposi sarcoma, lymphoma, and melanoma.4-6
Melanoma of the leg, a malignant neoplasm characterized by uncontrolled growth of melanocytes, can occasionally masquerade as a benign lesion, leading to misdiagnosis, mistreatment, and late diagnosis with possible metastasis. In the European Union, skin melanoma was the sixth most diagnosed cancer in 2020 and was responsible for 1.3% of all cancer-related deaths.8
Overall survival rates for patients with melanoma is strictly related to depth of tumor invasion, together with lymph node involvement and distant metastasis, constituting precisely the main parameters of the AJCC classification for melanoma staging. The overall 5-year survival rate by stage ranges from a high of 99% for melanoma in situ, to a substantially lower rate of 15% to 20% for stage IV melanoma (the most advanced stage).9
Nearby skin, subcutaneous tissue, and lymph nodes are the most affected regional metastatic sites, while the most common sites of distant metastases are skin, lung, brain, liver, bone, and intestine.10 In-transit melanoma metastases, also known as satellite or microsatellite metastases, are a type of locoregional recurrence of melanoma that occurs in the skin or subcutaneous tissue between the primary melanoma site and the regional lymph node basin. Hematogenous spreading typically takes place at a later stage, often in stage III disease.11,12
In the patient with an ulcer, it is imperative to establish an accurate diagnosis and initiate the appropriate therapy. During observation of a wound that does not respond to topical therapy, factors that may raise suspicion for malignancy include the presence of hypertrophic granulation tissue that does not heal, unusual pigmentation, and raised edges, as well as the possible coexistence of satellite lesions. Malignant wounds may exhibit different appearances, whether as crater-like ulcers indicative of a destructive process or as raised nodules resembling cauliflower-like growth, or sometimes combining both aspects. Malignant wounds are also characterized by rapid growth, hence the granulation tissue and proliferating vessels often observed in these lesions. Frequent findings are malodor, exudate, edema, necrosis, pain, easy bleeding, pruritus, and susceptibility to infection. Initial local invasion often presents as an inflammatory response characterized by redness, induration, heat, and tenderness. Formation of necrotic tissue typically follows, creating an environment conducive to bacterial proliferation, leading to secondary infections. Swift expansion of the tumor may compress adjacent structures such as soft tissues and nerves, resulting in pain and reduced mobility.4,6,13-15 It is also helpful to observe perilesional skin, which in malignant wounds, unlike venous-based wounds, does not show signs of eczema, lipodermatosclerosis, white atrophy, or superficial varices (or, if present, those signs are not of sufficient magnitude to warrant a therapy-resistant ulcer).3 Moreover, chronic venous ulcers are typically situated in the lower leg, especially in the perimalleolar area, and appear to be associated with an increased disease burden for the patient, whereas malignant wounds have the potential to present in any anatomic site, but seem to arise more frequently in areas both sun-exposed and prone to trauma, such as the anterior shin.4,16
Together with clinical observation, dermoscopy can be helpful in differentiating skin neoplasms from benign lesions. Dermoscopy is especially helpful in aiding diagnosis by identifying typical features of the major skin malignant tumors of the lower limb, for example, the presence of red globules, a gray-to-blue veil, irregular vessels, or irregular pigmentation in patients with melanoma.14
A previous study conducted by Ghasemi et al4 in a tertiary wound clinic identified 726 leg ulcers. Of these, 124 had atypical presentations and were biopsied, revealing a malignancy rate of 16.1% (20 of 124). These findings reaffirm how crucial it is for physicians to suspect a malignant etiology when presented with an ulcer with atypical clinical features. Additionally, the findings underscore the critical importance of performing a skin biopsy for histological confirmation of malignancy in suspicious-appearing lesions. Currently, there is no unanimous agreement regarding a recommended waiting period or frequency for cutaneous biopsy. Recent research indicates that multiple and repeated biopsies are advisable in cases in which there is a strong clinical suspicion of malignancy, especially after lack of response to 3 months or more of appropriate treatment; it is recommended that 2 punch biopsies (4 mm or 5 mm) be performed: 1 on the edge and 1 in the center of the ulcer.4,15,17
Management of atypical ulcers requires a multifaceted treatment approach. Both local and systemic therapies are tailored to the specific underlying causes.
The leading approach for managing primitive neoplastic ulcers typically involves initiating surgical intervention as the first-line treatment, followed by consideration of chemotherapy, radiotherapy, electrochemotherapy, or other adjuvant/neoadjuvant systemic therapies, depending mainly on type of neoplasm, mutational profile, clinical features such as size, ulceration (eg, patients with ulcerated primary melanoma appear to experience significant benefit when treated with adjuvant interferon-α), extent of invasion, and patient comorbidities and general performance status.15,18,19
Similarly, treatment of cutaneous metastases depends on various factors, including the number, size, and location of the metastases, as well as the patient's overall comorbidities, performance status, and preferences. Therapeutic options include local therapies, such as surgical excision, intralesional injection (with bacille Calmette-Guérin, interferon, interleukin 2, or oncolytic viruses), local ablation therapy, topical imiquimod, and radiation therapy; regional therapies, such as isolated limb perfusion or infusion with melphalan; and systemic therapies, such as immunotherapies, small molecule inhibitors, and chemotherapies.12
Palliative wound management is important in neoplastic cases, with the aim of controlling disease advancement and enhancing the patient's quality of life. This is achieved by addressing issues such as pain, exudate, bleeding, and odor (the so-called PEBO approach) through the careful selection of suitable dressings.20 Case studies encourage the use of wound care products, including polyurethane foam and nonadhesive gelling foam dressings, activated charcoal dressings, and topical metronidazole gel as a means of controlling infection and odor.15,20,21
The present report discusses the case of a patient who presented with ulcerated melanoma of the lower limb. Although he exhibited all the aforementioned characteristics, including in-transit metastases, his wound was misdiagnosed as a vascular wound and treated accordingly for years.
Case Report
A 64-year-old male was admitted to the neurologic department of the Hospital "Spedali Civili" in Brescia for cerebellar ischemia. During that hospital stay, a dermatologic consultation was requested to guide treatment of a "vegetative ulcerative lesion of lower limb in patient with venous deficiency."
The patient's medical records showed that in the previous 2 years he was evaluated by different specialists, including his general practitioner, internal medicine physicians, and vascular and orthopedic surgeons. The patient had undergone bilateral hip replacement with subsequent rehabilitation, and he also received outpatient care for gout and renal failure. Each of the aforementioned specialists made note of a bleeding ulcer of the right lower extremity in the patient's record, but they merely prescribed a lower extremity venous ecocolordoppler (which the patient had repeated several times over the years), suspecting venous insufficiency of the lower extremities. Observing the same vegetant ulcer, in addition to severe lymphedema of the right leg and some ipsilateral hyperpigmented nodules, the neurologists who admitted him hypothesized local venous thrombosis. Therefore, arterial and venous color Doppler ultrasound was performed again, which identified patent arteries and veins. Nevertheless, the vascular surgeon who performed the examination classified the hyperpigmented lesions as thrombosed varices.
Infectious diseases and dermatological evaluations were also requested. Infective ulceration was suspected, and the infectiologist conducted a skin culture swab, which was positive for multisensitive Enterococcus faecalis and Enterobacter cloacae. However, the culture results were deemed diagnostically nonsignificant.
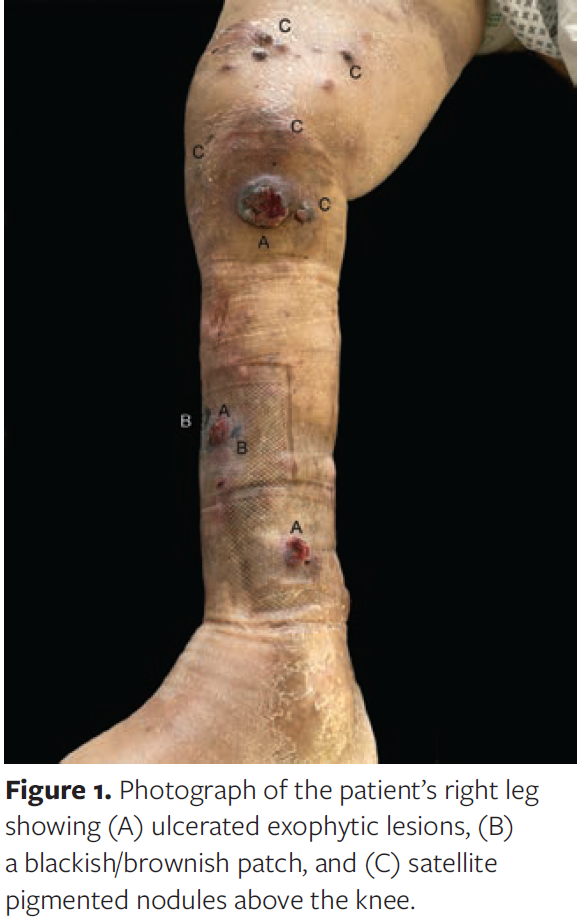
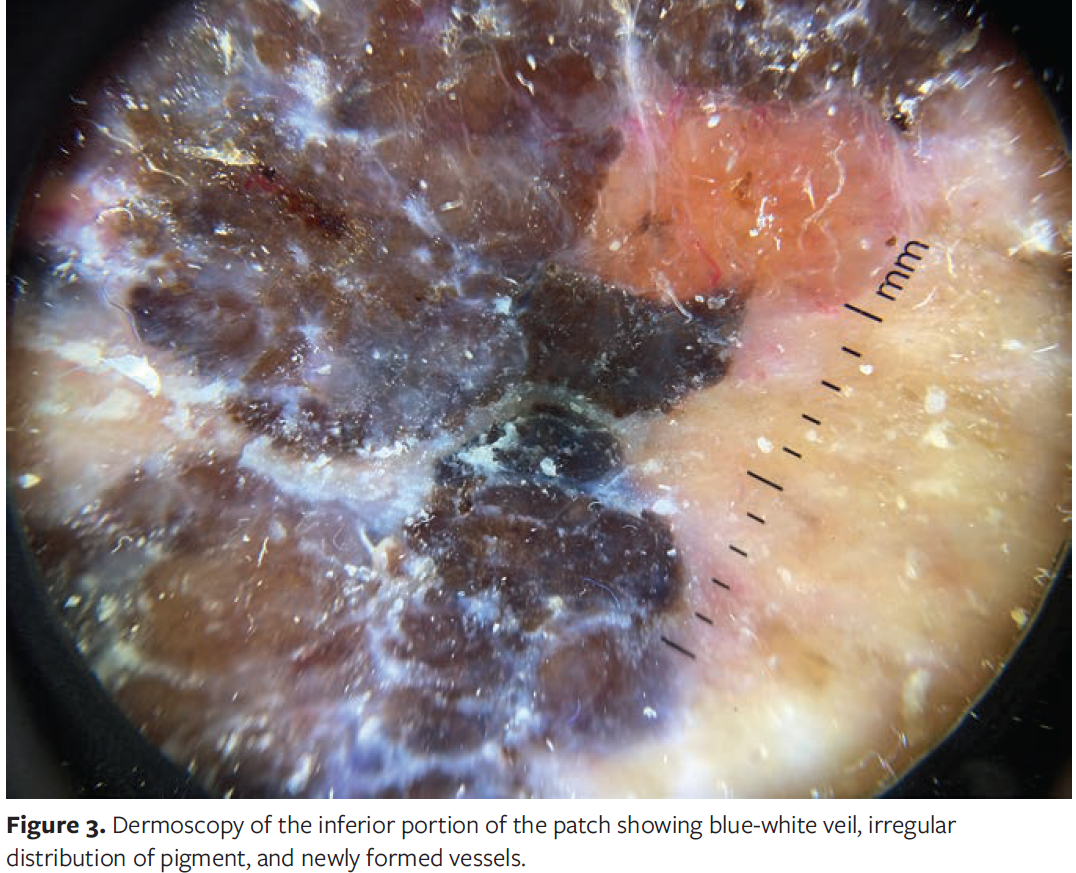
Dermatological evaluation revealed 3 ulcerated nodules on the pretibial area, the largest of which was 4 cm in diameter (the lesion for which the evaluation was requested), as well as 26 black, firm nodules about the knee that were nontender to palpation, and a blackish-brown lateral pretibial patch measuring 5 cm × 5 cm (Figures 1, 2). Dermoscopy of the patch showed atypia with irregular structure, inverted network, blue-white veil, multiple brown and black dots, and scar-like depigmentation coexisting with hyperpigmentation (Figure 3), all of which were strongly suspicious for melanoma. The primary diagnostic hypothesis in this case was invasive melanoma with satellite ulcerated and nodular metastases, because inspection of the entire lower limb with the hyperpigmented satellite nodules (some ulcerated, some flat) showed clear signs of in-transit invasion (Figure 1).

On physical examination, ipsilateral inguinal lymph nodes appeared enlarged and were hard on palpation, suggesting likely involvement of the region.
After obtaining the patient's informed consent, clinical photographs were taken, and a biopsy of 1 of the black nodules was immediately performed. The biopsy results confirmed the clinical suspicion of localized melanoma.
Total-body computed tomography returned no evidence of encephalic metastasis. However, according to the neurologist, the patient's cerebellar ischemia was believed to be due to neoplastic embolization. Multiple pulmonary nodules were found that were suspected to be metastatic in origin, with bilateral pleural effusion. As expected, involvement of the right inguinal lymph nodes was confirmed. Because of the patient's poor general condition and comorbidities, the oncologist determined that there was no indication for active oncologic treatment and proposed palliative care instead. In the weeks following this evaluation, the patient's condition rapidly deteriorated, with sepsis, a high fever unresponsive to treatment, and persistent impairment of his state of consciousness. He was transferred to hospice care, where he continued to receive palliative care. Unfortunately, the patient died in the same facility 6 weeks later.
Discussion
The report of this particularly unsettling case is shared to emphasize the importance of early detection and accurate diagnosis of malignant wounds. In numerous instances, attributing such diagnostic delays to a patient's denial of seeking medical attention could be a fair assessment. In this particular case, however, over the 2-year period preceding the conclusive diagnosis, the patient was evaluated by various specialists who observed the lesion and documented its presence. Nevertheless, the patient was never referred to a dermatologist. Plausibly, in the early stages, a mere chromatic change labeled as venous stasis hyperpigmentation may have concealed a superficial melanoma. This nonrecognition subsequently allowed progression to a nodular form that was then mistakenly assumed to be a continuation of venous insufficiency. The dermatologist was consulted only when the nodules ulcerated, at which time guidance was sought on wound medication rather than clarification of the cause. The dermatologist should have been the first specialist consulted for evaluation of the pigmented lesion.
This case raises substantial concerns about potential deficiencies in the referral system and various barriers to accessing dermatological care, including social, economic, and geographical factors. Most significantly, it underscores the urgent need for enhanced physician training in recognizing so-called red flags indicative of potential malignancy and in discerning when specialist evaluation is required for optimal patient care. Efforts have been made to train nonspecialist health professionals to recognize suspicious skin lesions, and thus far, these initiatives have yielded positive results.22
The authors of the current report strongly recommend that when encountering nonhealing wounds (ie, ulcers unresponsive to 4 weeks of appropriate wound dressing), atypical wounds, or any hyperpigmented lesion—especially those that exhibit characteristics such as exophytic growth, bleeding, ulceration, being surrounded by satellite nodules, or presenting with healthy perilesional skin—the general practitioner (typically the first health care professional in contact with the patient), or any other specialist who is unable to classify the lesion within their field of expertise, promptly refer the patient to a dermatologist. This proactive referral is crucial, given the heightened prevalence of melanomas and the increased mortality rate associated with cases that are not recognized early.
The contribution of a dermatologist is crucial, because these specialists are the best trained in using 2 essential diagnostic tools: dermoscopic observation of lesional and perilesional skin, and histopathological analysis by biopsy. Dermatologists are well trained in recognizing various skin diseases and often use dermoscopy to enhance diagnostic accuracy, not only for melanocytic lesions but also for nonmelanoma skin cancers, inflammatory conditions, and almost any other cutaneous neoformation.23,24 Furthermore, dermatologists are adept at performing skin biopsies to assess the etiology of skin dermatoses.
LImitations
This report is limited by its focus on a single case. Furthermore, there were limitations related to the absence of prior images of the patient's lesion and the suboptimal quality of the images captured, mainly due to the circumstances of the evaluation. The patient was assessed while lying in bed, with mobility constraints and significant pain.
Conclusion
Neoplastic ulcers are relatively uncommon, but they warrant consideration in the assessment of a nonhealing wound, particularly one that exhibits atypical features in terms of morphology, growth, inadequate response to therapy, and the appearance of perilesional skin. The suspicion of this diagnosis is vitally important for the timely identification of neoplastic conditions, especially in instances of rapidly progressing malignancies such as melanoma. Considering the significance of the topic and the proven effectiveness of training, it is essential for the physician to skillfully determine when additional investigations are needed to rule out the possibility of malignancy. Consequently, physicians in Italy should not hesitate to refer patients with nonresponsive ulcers for a dermatological consultation for specialized evaluation as well as confirmation or exclusion of clinical suspicions, with the potential for using tools such as dermoscopy and biopsy in the evaluation. This step is vital to achieve earlier diagnosis and a more favorable prognosis.
Acknowledgments
Authors: Paola Monari, MD; Benedetta Galli, MD; and Piergiacomo Calzavara Pinton, MD
Affiliation: University of Brescia, Brescia, Italy
ORCID: Calzavara Pinton, 0000-0002-0935-7204; Galli, 0009-0003-9587-9571; Monari, 0000-0002-6693-0732
Disclosure: The authors disclose no financial or other conflicts of interest.
Correspondence: Benedetta Galli, MD; University of Brescia, Dermatology and Venereology, P.le Spedali Civili, 1, Brescia, Italy 25123; b.galli003@unibs.it
Manuscript Accepted: February 2, 2024
References
1. Dissemond J, Körber A, Grabbe S. [Differential diagnoses in leg ulcers.] Article in German. J Dtsch Dermatol Ges. 2006;4(8):627-634. doi:10.1111/j.1610-0387.2006.06052.x
2. Monari P, Gualdi G, Rovaris S, Venturuzzo A, Rovati C, Pinton PC. Etiology of chronic leg ulcers in a dermatologic wound clinic: a retrospective observational study. Wound Manag Prev. 2022;68(8):12-15.
3. Adam DJ, Naik J, Hartshorne T, Bello M, London NJ. The diagnosis and management of 689 chronic leg ulcers in a single-visit assessment clinic. Eur J Vasc Endovasc Surg. 2003;25(5):462-8. doi:10.1053/ejvs.2002.1906
4. Ghasemi F, Anooshirvani N, Sibbald RG, Alavi A. The point prevalence of malignancy in a wound clinic. Int J Low Extrem Wounds. 2016;15(1):58-62. doi:10.1177/1534734615627721
5. Perrotto J, Glick B. Lower extremity malignancies masquerading as ulcers. Ostomy Wound Manage. 2006;52(10):46-52.
6. Kirchberger MC, Erfurt-Berge C. Management of malignant wounds [Management ma-ligner wunden]. Article in German. Z Gerontol Geriat. 2020;53(6):572–576. doi:10.1007/s00391-019-01629-w
7. Gualdi G, Monari P, Calzavara-Pinton P, Farisoglio C, Ginani A, Catrani S. Early cutaneous metastasis of adenoid cystic carcinoma of the salivary gland. Cutis. 2014;93(6):E16-E18.
8. ECIS - European Cancer Information System. European Union. 2023. Accessed October 20, 2023. https://ecis.jrc.ec.europa.eu/pdf/factsheets/Melanoma_cancer_en.pdf
9. O'Neill CH, Scoggins CR. Melanoma. J Surg Oncol. 2019;120(5):873-881. doi:10.1002/jso.25604
10. Damsky WE Jr., Rosenbaum LE, Bosenberg M. Decoding melanoma metastasis. Cancers. 2011;3(1):126-163. doi:10.3390/cancers3010126
11. Marghoob AA, Changchien L, DeFazio J, et al. The most common challenges in melanoma diagnosis and how to avoid them. Australas J Dermatol. 2009;50(1):1-13. doi:10.1111/j.1440-0960.2008.00496_1.x
12. Gabriel E, Skitzki J. The role of regional therapies for in-transit melanoma in the era of improved systemic options. Cancers (Basel). 2015;7(3):1154-1177. doi:10.3390/cancers7030830
13. Starace M, Carpanese MA, Pampaloni F, et al. Management of malignant cutaneous wounds in oncologic patients. Support Care Cancer. 2022;30(9):7615-7623. doi:10.1007/s00520-022-07194-0
14. Janowska A, Davini G, Fidanzi C, et al. Atypical ulcer arising on stasis dermatitis: achromic melanoma. Wounds. 2022;34(2):E10-E12. doi:10.25270/wnds/2022.e1012
15. Janowska A, Dini V, Oranges T, Iannone M, Loggini B, Romanelli M. Atypical ulcers: diagnosis and management. Clin Interv Aging. 2019;14:2137-2143. doi:10.2147/CIA.S231896
16. Monari P, Pelizzari L, Crotti S, Damiani G, Calzavara-Pinton P, Gualdi G. The use of PRISM (pictorial representation of illness and self measure) in patients affected by chronic cutaneous ulcers. Adv Skin Wound Care. 2015;28(11):489-494. doi:10.1097/01.ASW.0000471977.92623.65
17. Senet P, Combemale P, Debure C, et al. Malignancy and chronic leg ulcers: the value of systematic wound biopsies: a prospective, multicenter, cross-sectional study. Arch Dermatol. 2012;148(6):704-708. doi:10.1001/archdermatol.2011.3362.
18. Barricklow Z, DiVincenzo MJ, Angell CD, Carson WE. Ulcerated cutaneous melanoma: a review of the clinical, histologic, and molecular features associated with a clinically aggressive histologic phenotype. Clin Cosmet Investig Dermatol. 2022;15:1743-1757. doi:10.2147/CCID.S372287
19. Terheyden P, Krackhardt A, Eigentler T. The systemic treatment of melanoma. Dtsch Arztebl Int. 2019;116(29-30):497-504. doi:10.3238/arztebl.2019.0497
20. Janowska A, Davini G, Dini V, Iannone M, Morganti R, Romanelli M. Local management of malignant and unresectable fungating wounds: PEBO assessment. Int J Low Extrem Wounds. 2021:15347346211053478. doi:10.1177/15347346211053478
21. Chrisman CA. Care of chronic wounds in palliative care and end-of-life patients. Int Wound J. 2010;7(4):214-235. doi:10.1111/j.1742-481X.2010.00682.x
22. Harkemanne E, Goublomme N, Sawadogo K, Tromme I. Early melanoma detection in primary care: clinical recognition of melanoma is not enough, one must also learn the basics. J Cancer Educ. 2022;37(4):898-904. doi:10.1007/s13187-020-01897-w
23. Caresana G, Giardini R. Dermoscopy-guided surgery in basal cell carcinoma. J Eur Acad Dermatol Venereol. 2010; 24(12):1395-1399. doi:10.1111/j.1468-3083.2010.03652.x
24. Guida S, Longhitano S, Ardigò M, et al. Dermoscopy, confocal microscopy and optical coherence tomography features of main inflammatory and autoimmune skin diseases: a systematic review. Australas J Dermatol. 2022;63(1):15-26. doi:10.1111/ajd.13695






