


An Innovative Retrieval Technique for an Entrapped Rotational Atherectomy Device: A Case Discussion From the 2015 SCAI Fellows Course
An entrapped rotational atherectomy burr is uncommon, but one of the nightmare complications in the cardiac cath lab.1 Familiarity with various retrieval techniques and skilled application is the key to successful retrieval.
Case report
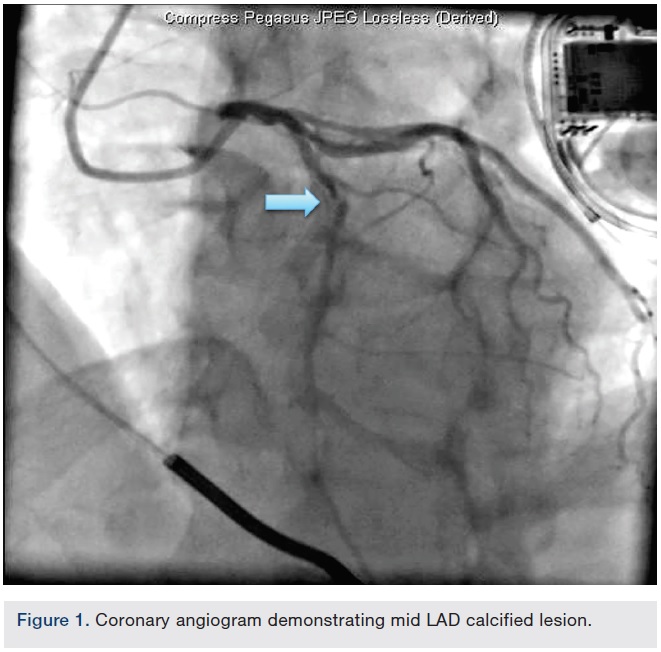 A 69-year-old male with coronary artery disease, prior left anterior descending artery (LAD) stenting, ischemic cardiomyopathy, hypertension, diabetes, and hyperlipidemia underwent coronary angiography for worsening angina and anterior ischemia on stress testing. Coronary vessels were heavily calcified. A prior stent was visualized in the proximal and mid LAD with 50% in-stent stenosis proximally and 95% sub-total occlusion just distal to the stent or within the stent (difficult to delineate due to severe calcification). The LAD lesion was thought to be the culprit. Rotational atherectomy was undertaken due to the calcification distal to the stent.
A 69-year-old male with coronary artery disease, prior left anterior descending artery (LAD) stenting, ischemic cardiomyopathy, hypertension, diabetes, and hyperlipidemia underwent coronary angiography for worsening angina and anterior ischemia on stress testing. Coronary vessels were heavily calcified. A prior stent was visualized in the proximal and mid LAD with 50% in-stent stenosis proximally and 95% sub-total occlusion just distal to the stent or within the stent (difficult to delineate due to severe calcification). The LAD lesion was thought to be the culprit. Rotational atherectomy was undertaken due to the calcification distal to the stent.
 A 6 French Ultimate 2 guide (Merit Medical) through a right radial approach was used to engage the left main. A Balance Middleweight (BMW) wire (Abbott Vascular) was passed distal to the LAD, then exchanged for an Extra Support RotaWire (Boston Scientific) via a Micro 14 catheter (Roxwood Medical). A 1.5 mm RotaLink Plus (Boston Scientific) was used for atherectomy and 2 runs were performed with no deceleration as per staff. The Rota burr popped through the lesion, then stalled.
A 6 French Ultimate 2 guide (Merit Medical) through a right radial approach was used to engage the left main. A Balance Middleweight (BMW) wire (Abbott Vascular) was passed distal to the LAD, then exchanged for an Extra Support RotaWire (Boston Scientific) via a Micro 14 catheter (Roxwood Medical). A 1.5 mm RotaLink Plus (Boston Scientific) was used for atherectomy and 2 runs were performed with no deceleration as per staff. The Rota burr popped through the lesion, then stalled.
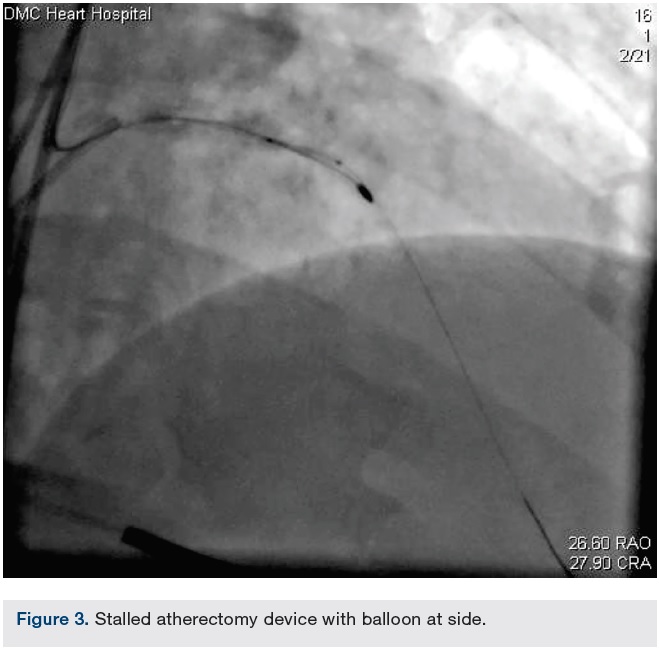 Gentle manual traction on the Rota burr shaft could not retract the burr, but did cause the vessel to accordion and caused the guide to deeply intubate the left main (LM) artery. Multiple attempts at spinning the burr were attempted, but it remained stalled. The patient remained hemodynamically stable.
Gentle manual traction on the Rota burr shaft could not retract the burr, but did cause the vessel to accordion and caused the guide to deeply intubate the left main (LM) artery. Multiple attempts at spinning the burr were attempted, but it remained stalled. The patient remained hemodynamically stable.
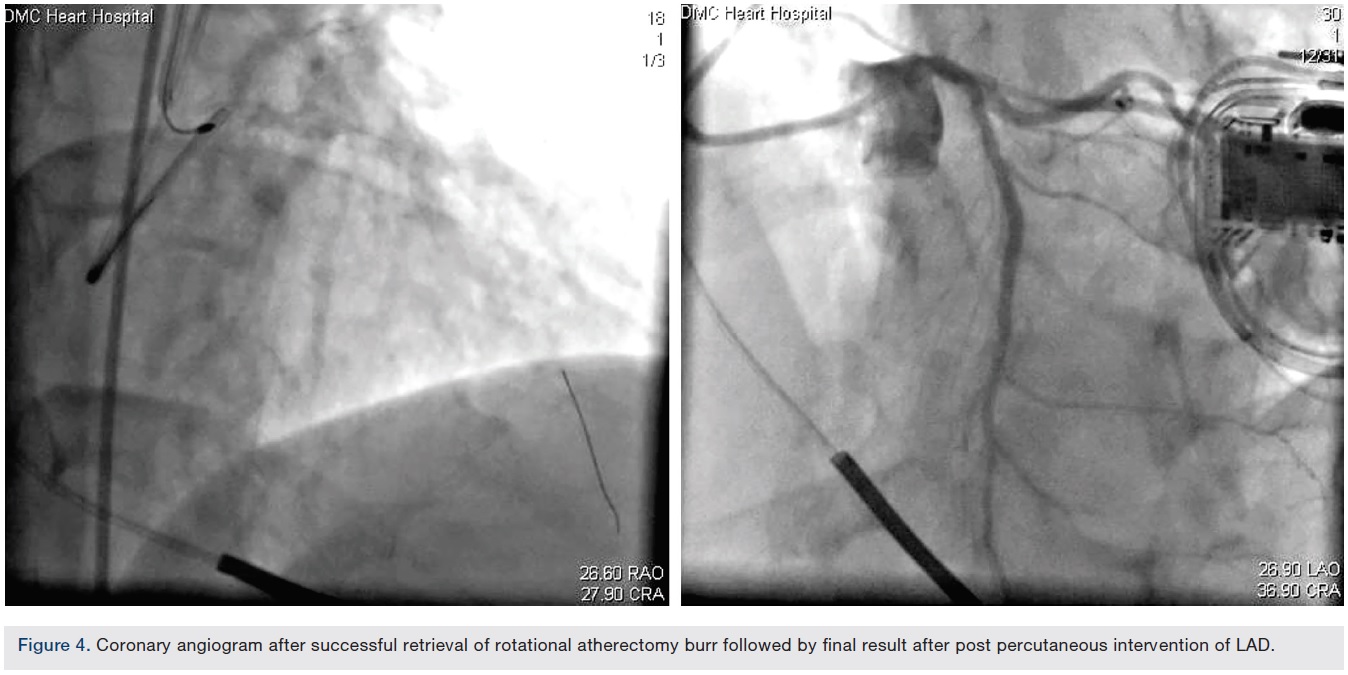
Femoral access was obtained. The LM was engaged with a second guide (Xtra Backup [XB] 3.5 guide). A BMW wire was negotiated to the distal LAD beyond the burr. Multiple inflations of a 1.5 x 12 mm balloon were performed beside, proximal, and distal to the burr. This was followed by serial inflations using a 2.0 x 12 mm balloon. A slight tug on the Rota burr was then successful in retrieving it.
Mechanism of burr entrapment
 The Rotablator device is an olive-shaped, front-cutting, diamond-coated and tipped burr for antegrade ablation. The back side (proximal part) of this burr is smooth and does not allow cutting when pulling back. Spinning displaces friction orthogonally, reducing forward friction and allowing the burr to advance slowly, debulking the lesion as it moves forward.
The Rotablator device is an olive-shaped, front-cutting, diamond-coated and tipped burr for antegrade ablation. The back side (proximal part) of this burr is smooth and does not allow cutting when pulling back. Spinning displaces friction orthogonally, reducing forward friction and allowing the burr to advance slowly, debulking the lesion as it moves forward.
The proposed mechanisms of burr entrapments are spasm, advancement of a small burr beyond a calcified lesion, under-deployed stents, or in-stent stenosis without sufficient ablation. Popping the device through unprepared lesions may lead to distal entrapment. The absence of retrograde debulking is a limitation to removal at this point. The device can get stuck at a bend in a calcified vessel due to coronary spasm or incomplete atherectomy of calcium.
Use of a smaller burr, with high speed, minimal forward pressure while advancing the burr, slow advancement of the burr, and avoidance of deceleration helps to prevent this complication.
Retrieval techniques
 Several bailout techniques were discussed after presentation of this case during the 2015 SCAI Fall Fellows Course. Manual traction on the Rota burr is the easiest method with off-on low speed rotation in Dynaglide mode. However, careful monitoring of traction on the vessel and avoiding deep seating of the guide are necessary in order to avoid vessel injury. Excessive traction on the shaft may result in shaft fracture.
Several bailout techniques were discussed after presentation of this case during the 2015 SCAI Fall Fellows Course. Manual traction on the Rota burr is the easiest method with off-on low speed rotation in Dynaglide mode. However, careful monitoring of traction on the vessel and avoiding deep seating of the guide are necessary in order to avoid vessel injury. Excessive traction on the shaft may result in shaft fracture.
Advancing the burr into the distal lumen and retrieving it, all while rotating it, may allow for retrieval.
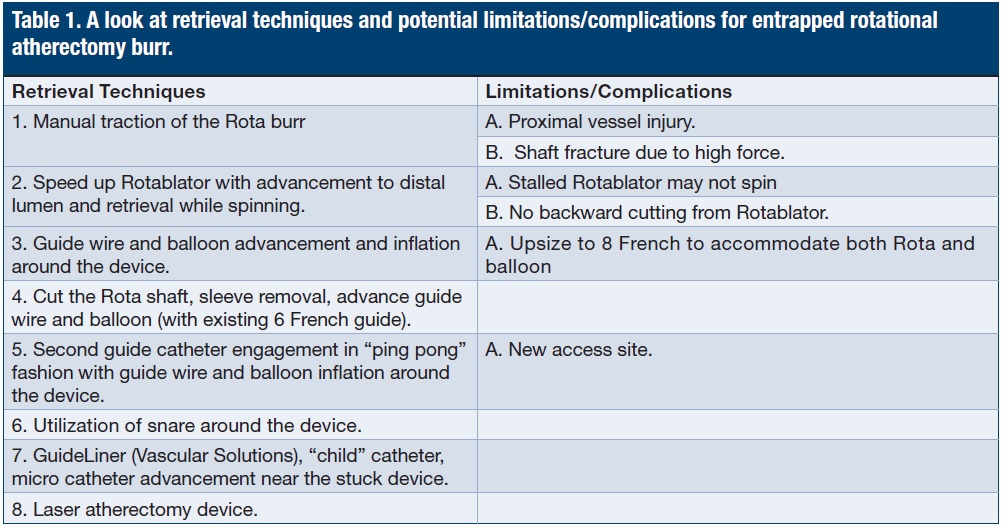 Passing a guide wire distal to the lesion and passing a small balloon alongside the stuck device with serial balloon inflations may allow successful removal. However, guide size is a limitation for this technique. The shaft of the Rotablator is 4.3 French and most balloon catheters are 3 French, so utilization of an 8 French guide may be necessary. Upsizing of the guide can be done after cutting off the advancer sheath (but will not allow any further spinning of the burr). Alternatively, a separate access and guide catheter may be needed to pass the wire and balloon, as reported in this case.
Passing a guide wire distal to the lesion and passing a small balloon alongside the stuck device with serial balloon inflations may allow successful removal. However, guide size is a limitation for this technique. The shaft of the Rotablator is 4.3 French and most balloon catheters are 3 French, so utilization of an 8 French guide may be necessary. Upsizing of the guide can be done after cutting off the advancer sheath (but will not allow any further spinning of the burr). Alternatively, a separate access and guide catheter may be needed to pass the wire and balloon, as reported in this case.
Drive shaft sheath removal after cutting off near the advancer and insertion of a second guide wire/balloon through the 6 French guide is another innovative method.2
As another way to remove the device, passing the snare over the shaft, after cutting the shaft as described above, and snaring the shaft just proximal to the burr may allow retraction of the burr and guide catheter in a controlled fashion.
Advancement of a daughter-through-mother catheter after cutting the shaft as above and applying traction on the burr and anti-traction to the daughter catheter can provide a large, local force to retrieve the burr.3 The daughter catheter will prevent proximal vessel damage and can be helpful if dissection/perforation at the stuck site occurs.
Laser coronary atherectomy can be used for successful retrieval by modifying and softening the calcified lesion/plaque behind the entrapped device.
Acknowledgments. We wish to acknowledge and thank the SCAI Fellows Course Directors, James C. Blankenship, MD, MHCM, FSCAI, SCAI President, and Morton Kern, MD, MSCAI.
References
- Grise MA, Yeager MJ, Teirstein PS. A case of an entrapped rotational atherectomy burr. Catheter Cardiovasc Interv. 2002; 57: 31-33.
- Sakakura K, Ako J, Momomura S. Successful removal of an entrapped rotablation burr by extracting drive shaft sheath followed by balloon dilatation. Catheter Cardiovasc Interv. 2011 Oct 1; 78(4): 567-570.
- Cunnington M, Egred M. GuideLiner, a child-in-a-mother catheter for successful retrieval of an entrapped rotablator burr. Catheter Cardiovasc Interv. 2012 Feb 1; 79(2): 271-273.
- Kadohira T, Schwarcz AI, De Gregorio J. Successful retrieval of an entrapped guide wire between a deployed coronary stent and severely calcified vessel wall using excimer laser coronary atherectomy. Catheter Cardiovasc Interv. 2015 Feb 1; 85(2): E39-E42.
Disclosure: Dr. Kusum Lata and Dr. Cindy Grines report no conflicts of interest regarding the content herein.
The authors can be contacted via Dr. Kusum Lata at lata.drkusum@gmail.com.



