


In Situ Quantification and 3D Reconstruction of Thrombus in SFA Disease Using Intravascular OCT
© 2026 HMP Global. All Rights Reserved.
Any views and opinions expressed are those of the author(s) and/or participants and do not necessarily reflect the views, policy, or position of Cath Lab Digest or HMP Global, their employees, and affiliates.
Mehmet Cilingiroglu, MD, FSCAI, FACC, FESC, FAHA1,2,3
1University of Hawaii John A. Burns School of Medicine, Honolulu, Hawaii; Hilo Benioff Medical Center, Hilo, Hawaii
2University of Texas Health at San Antonio, Texas
3University of Texas in Houston, MD Anderson Cancer Center, Houston, Texas
Disclosures: Dr. Cilingiroglu reports no conflicts of interest regarding the content herein.
Mehmet Cilingiroglu, MD, can be contacted at mcilingi@hawaii.edu.
 Superficial femoral artery (SFA) disease accounts for approximately 40% of symptomatic peripheral arterial disease (PAD) and remains a common cause of critical limb ischemia (CLI) and lower extremity amputation. Intra-arterial thrombus formation plays a key role in the disease process.1-4 Conventional angiography provides little information about the amount of the thrombus burden. Intravascular optical coherence tomography (OCT), a well-established laser light based imaging modality with a fine axial resolution of 10 micrometer (µm), offers superior sensitivity and specificity for the identification and accurate description of intraluminal thrombus.5 However, to date, quantification of the total clot burden has not been described.
Superficial femoral artery (SFA) disease accounts for approximately 40% of symptomatic peripheral arterial disease (PAD) and remains a common cause of critical limb ischemia (CLI) and lower extremity amputation. Intra-arterial thrombus formation plays a key role in the disease process.1-4 Conventional angiography provides little information about the amount of the thrombus burden. Intravascular optical coherence tomography (OCT), a well-established laser light based imaging modality with a fine axial resolution of 10 micrometer (µm), offers superior sensitivity and specificity for the identification and accurate description of intraluminal thrombus.5 However, to date, quantification of the total clot burden has not been described.
Methods
We hypothesized that three-dimensional (3D) reconstruction of the OCT studies could yield accurate quantification of the intra-arterial thrombus burden. Three patients who underwent a peripheral angiogram and OCT evaluation with the indication of lifestyle-limiting claudication were included in our study.
After invasive angiography, the OCT C7-XR system (Abbott) was used, following power injection of dextran at 8 mL/sec for 5 seconds. Thrombus was defined as a typically jagged protrusion into the luminal space of material with a homogenous texture. In one patient with chronic total occlusion (CTO) of the SFA, low-pressure balloon angioplasty was performed to reestablish blood flow and allow the passage of the OCT catheter (Figure 1).
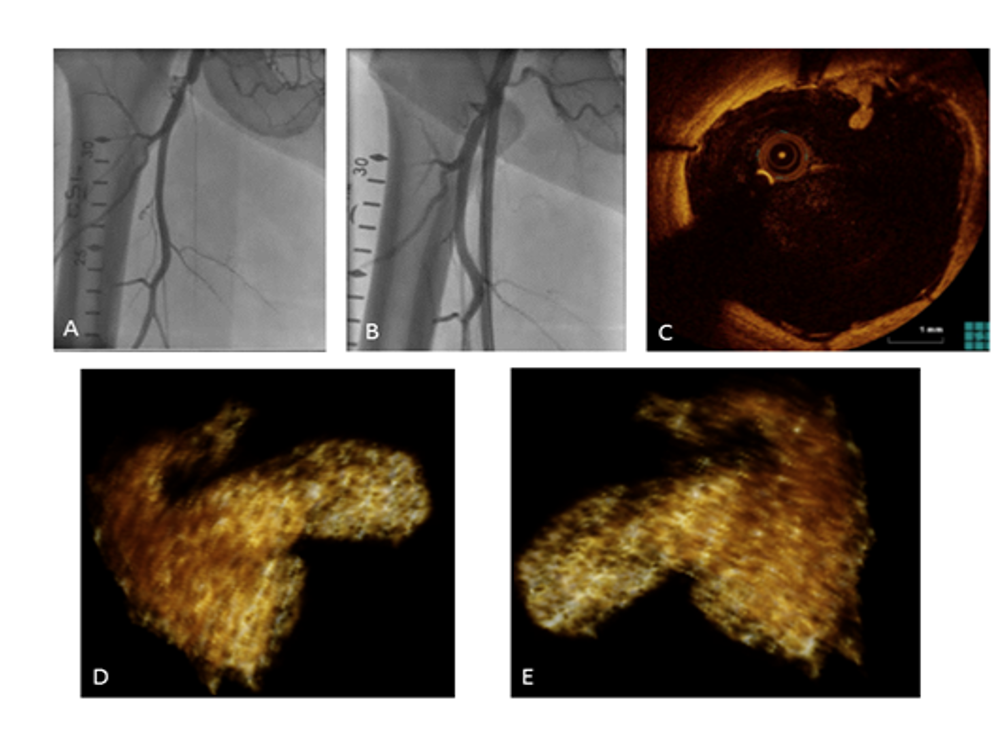
CTO: chronic total occlusion; SFA: superficial femoral artery; OCT: optical coherence tomography.
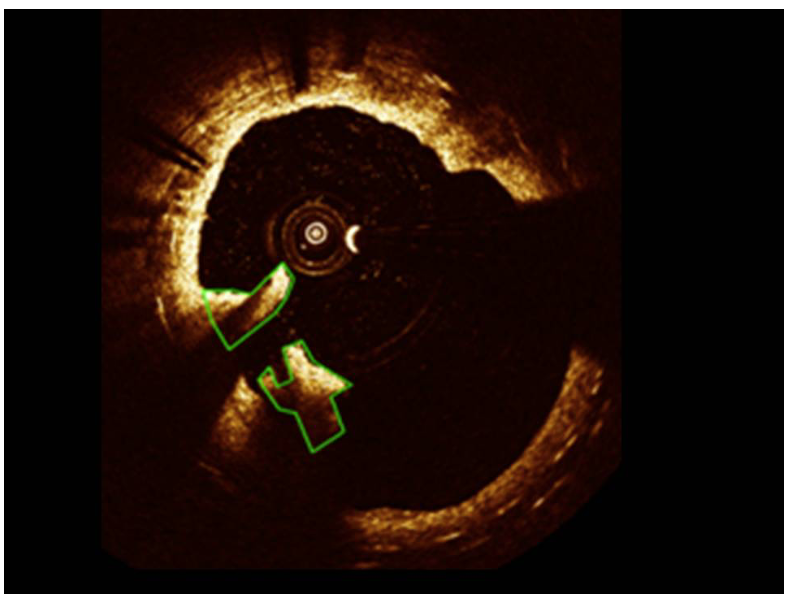
Using LabVIEW (National Instruments) custom-based imaging software, each frame of the OCT pullback was analyzed by manually tracing thrombi boundaries (Figure 2). All the image pixels of the clot were counted and then converted to a volume by calibrating the catheter to a 1 mm diameter. Thrombi boundaries were interpolated to provide a 3D visualization with ImageJ (custom imaging software) and volumetric quantification of the thrombus burden in the region of interest.
Results
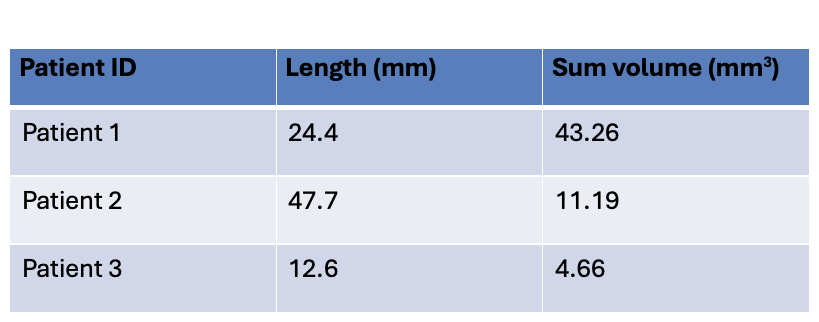
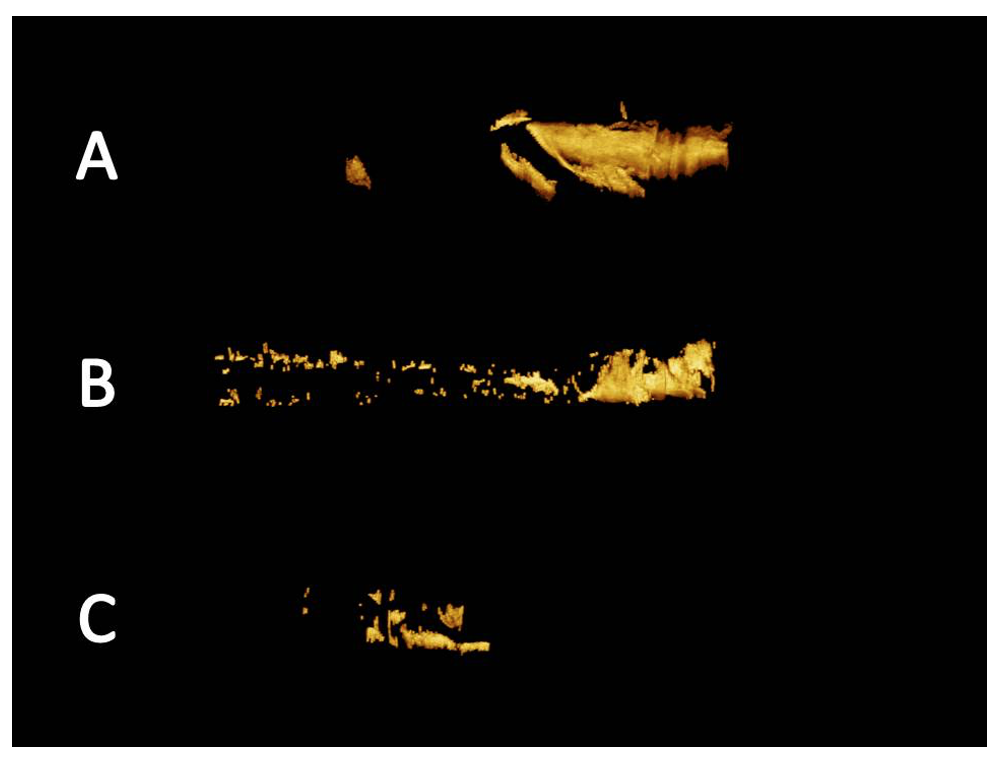
OCT was successfully performed in all three patients. We identified thrombus formation in all three patients despite absence of evident thrombosis with invasive angiography. In the first patient, the clot was of a moderate length (24.4 mm) but large in volume (43.26 mm3). In the second, the clot involved a longer arterial segment (47.7 mm) but the overall volume was smaller (11.19 mm3). The third patient had a smaller identifiable clot of 12.6 mm in length and 4.66 mm3 in volume. The results of our analysis (thrombus length, volume and 3D reconstruction) are shown in the Table and Figure 3.
Discussion
Early autopsy and surgical studies in the 1950s and 1960s demonstrated that atherosclerosis and thrombosis coexist in the progression of the “arterial occlusion”.1,2,6 In the TRA2P-TIMI 50 trial, the study of fresh arterial samples obtained at the time of peripheral bypass surgery showed thrombus occlusion that had undergone organization and recanalization.7
To our knowledge, this is the first report of OCT use for the quantification of thrombus. We have demonstrated that OCT can in vivo visualize and quantify thrombus in patients with PAD. The role, type, strength and duration of antiplatelet and anticoagulation after percutaneous interventions are currently unclear.8-12 Information about the total clot burden may influence the type of endovascular strategy, the use of antiplatelet, anticoagulation or thrombolytic agents, and the use of embolic protection devices. Atherosclerosis and thrombosis both contribute to the progression of PAD. OCT can accurately quantify the length and the volume of the clot burden. Larger studies are needed to assess their clinical importance in the prevention and management of PAD.

References
1. Dunlop GR, Santos R. Adductor-canal thrombosis. N Engl J Med. 1957 Mar 28; 256(13): 577-80. doi:10.1056/NEJM195703282561301
2. Lindbom A. Arteriosclerosis and arterial thrombosis in the lower limb; a roentgenological study. Acta Radiol Suppl. 1950; 80: 1-80.
3. Tai Z. Transcollateral approach for percutaneous revascularization of complex superficial femoral artery chronic total occlusion. J Invasive Cardiol. 2013 May;25(5):E96-100.
4. Mavor GE. The pattern of occlusion in atheroma of the lower limb arteries; the correlation of clinical and arteriographic findings. Br J Surg. 1956 Jan; 43(180): 352-364. doi:10.1002/bjs.18004318003
5. Marmagkiolis K, Lendel V, Leesar MA, Feldman MD, Cilingiroglu M. Use of optical coherence tomography during superficial femoral artery interventions. J Invasive Cardiol. 2014 May; 26(5): 220-223.
6. Watt JK. Origin of femoro-popliteal occlusions. Br Med J. 1965 Dec 18;2(5476):1455-1459. doi:10.1136/bmj.2.5476.1455
7. Bonaca MP, Scirica BM, Creager MA, et al. Vorapaxar in patients with peripheral artery disease: results from TRA2{degrees}P-TIMI 50. Circulation. 2013 Apr 9; 127(14): 1522-1529, 1529e1-6. doi:10.1161/CIRCULATIONAHA.112.000679
8. Efficacy of oral anticoagulants compared with aspirin after infrainguinal bypass surgery (The Dutch Bypass Oral Anticoagulants or Aspirin Study): a randomised trial. Lancet. 2000 Jan 29; 355(9201): 346-351.
9. Poredos P, Jezovnik MK. Is aspirin still the drug of choice for management of patients with peripheral arterial disease? VASA. Zeitschrift fur Gefasskrankheiten. Mar 2013; 42(2): 88-95. doi:10.1024/0301-1526/a000251.
10. Johnson WC, Williford WO; Department of Veterans Affairs Cooperative Study #362. Benefits, morbidity, and mortality associated with long-term administration of oral anticoagulant therapy to patients with peripheral arterial bypass procedures: a prospective randomized study. J Vasc Surg. 2002 Mar; 35(3): 413-421. doi:10.1067/mva.2002.121847
11. Ishihara T, Iida O, Awata M, et al. Angioscopically apparent large thrombus and uncovered stent struts 6 months after late stent thrombosis of a paclitaxel-coated nitinol drug-eluting stent implanted in the superficial femoral artery. Cardiovasc Interv Ther. 2014 Jan; 29(1): 82-85. doi:10.1007/s12928-013-0197-5
12. Hanna EB. Dual antiplatelet therapy in peripheral arterial disease and after peripheral percutaneous revascularization. J Invasive Cardiol. 2012 Dec; 24(12): 679-684.
13. GBD 2015 Disease and Injury Incidence and Prevalence Collaborators. Global, regional, and national incidence, prevalence, and years lived with disability for 310 diseases and injuries, 1990-2015: a systematic analysis for the Global Burden of Disease Study 2015. Lancet. 2016 Oct 8; 388(10053): 1545-1602. doi:10.1016/S0140-6736(16)31678-6


