Determining the Costs of an EMS System, and Why It Matters—Part 1
This article is the first of a three-part series examining the cost of modern EMS systems and how these systems can be funded.
Emergency medical services (EMS) clinicians in the United States respond to over 40 million calls and transport more than 30 million patients annually. Once a global leader in prehospital care, the U.S. EMS system has declined significantly during the past several decades due to chronic underfunding and a fragmented financing model.
Indicators of systemic dysfunction include:
- Over 2,500 U.S. counties with little to no access to EMS
- A tenfold variation in patient survival rates between EMS agencies
- A 10% disparity in cardiac arrest response times based on jurisdiction
- EMS clinician salaries that lag significantly behind comparable healthcare and public safety professionals
- Annual personnel turnover rates between 25% and 40%
- Occupational injury and fatality rates that far exceed those of similar professions
- A growing number of EMS agencies ceasing operations
Objective
To estimate the cost of implementing a sustainable, high-performance EMS system across the United States.
Evidence Review
This analysis draws on peer-reviewed literature, professional publications, and government reports to assess historical and current approaches to EMS funding.
Findings
A fully tax-funded high-performance EMS system would require an investment of approximately $103 per person annually. Alternatively, a hybrid funding model, in which Medicare, Medicaid, and private insurers contribute a prospective annual fee, could reduce taxpayer burden while ensuring financial sustainability and system resilience.
Conclusions and Relevance
Establishing a sustainable high-performance EMS system in the U.S. is essential to ensuring universal access to lifesaving prehospital care. It also represents a critical step toward achieving a 21st-century EMS infrastructure on par with those in other advanced nations.
Introduction
Clinicians in the EMS system respond to over 40 million calls for assistance, and transport over 30 million patients a year in the United States.1 In addition, they respond to disasters, are on stand-by alert at dangerous scenes such as fires and police actions as well as for mass gatherings, they treat patients who are not transported, they relieve overcrowded hospitals, and they contribute to community health through education and injury prevention interventions such as pediatric drowning prevention.2-7 The clinicians, including EMTs and paramedics, have a nationally recognized curriculum and community colleges often award more credit for paramedic programs than for nursing programs.8
Early patient transport systems existed in Napolean’s time but the modern ambulance system in the U.S. came about during the 1960s and 70s.9 By 1980, some of the systems in the U.S. were admired models for the world.10,11
Since the 1980s, the EMS systems in the U.S. have been struggling with increased demand, limited resources and an aging infrastructure; they have not succeeded in achieving goals set more than a decade ago, and have fallen far behind the performance of systems operating in other developed countries.12,13 The chief reason for this decline is a dysfunctional funding system. The dysfunctional funding system results in many adverse outcomes for Americans. These adverse outcomes include:
- 2,500 counties in the U.S. that have effectively no access to EMS14
- As much as a 10-times difference in patient survival rates between different EMS agencies15-18
- A 10% difference in response time to cardiac arrests depending on the jurisdiction where the patient collapses19,20
- Salaries of EMS clinicians being far below that of their health care and public safety colleagues21
- Personnel turnover rates of 25% to 40% a year22,23
- Occupational injury and fatality rates for EMS clinicians that are far above those of their professional counterparts24-27
- Large variations in payments to ambulance services based on the local mix of insurance providers28
- Numerous EMS agencies going out of business.29,30
Additionally, Americans have largely not had access to the 21st century advances in clinical care and EMS operations that have been implemented in other countries. For example, other countries have some paramedics who have clinical master’s degrees and who work as community paramedics; these clinicians can reduce transports to emergency departments by 50%.31-34 In addition to saving costs associated with having the patient brought to a hospital emergency department, community paramedics treat many patients at home allowing these patients to stay home and follow up with their personal health care provider.
This analysis addresses the question: how much would it cost to fund a high-performance EMS system in the U.S.? Establishing a high-performance EMS system is a necessary precursor to creating a 21st century EMS system in the U.S.
The Obstacle to Funding EMS in the U.S.
The primary barrier to establishing a high-performance EMS system in the United States is the federal government’s long-standing failure to reimburse EMS agencies for the full cost of care provided to Medicare and Medicaid beneficiaries.35 Medicare, administered by the Centers for Medicare and Medicaid Services (CMS), is the single largest payer of EMS services.36,37 The CMS payment is based on a base rate with adjustments for geography and mileage.38 However, its reimbursement rates fall significantly short of covering actual service costs, as confirmed by industry experts reviewing the most recent Medicare Ground Ambulance Data Collection project published in December 2024.35,39 On average, CMS reimbursement for an ambulance to transport a patient is $2,344 less than the cost of providing each transport.40
Although EMS agencies depend on CMS funding, there has been little progress in 50 years to modify CMS payment policies and promote the development of a national EMS system that balances quality, sustainability, system development, and cost.39
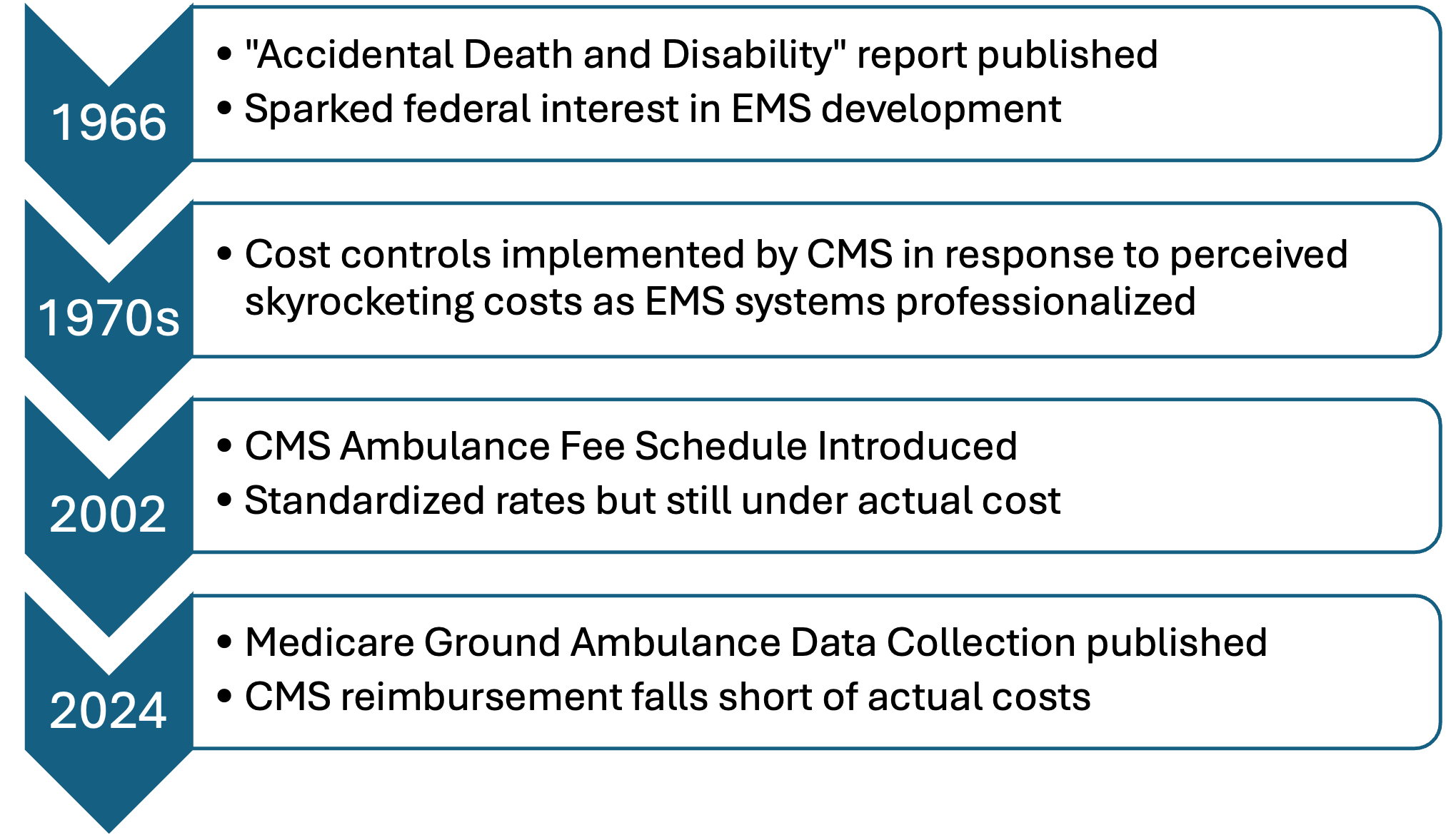
Historically, in the 1960s and 1970s, ambulance services, often operated by mortuaries, began transitioning into regulated, medically equipped EMS providers. These transitions, driven both by federal mandates and community demand, increased operational costs. However, cost increases, sometimes as small as $10 per transport, were perceived as excessive due to the low base price of ambulance services at the time. This perception led CMS, in 1974, to impose strict cost controls just as EMS planning agencies were advocating for improved system development.41
In 2002, CMS replaced its retrospective payment system with a national fee schedule, following a negotiated rulemaking process in accordance with the Federal Advisory Committee Act and the Negotiated Rulemaking Act of 1990.42 The resulting fee schedule still did not cover actual costs of delivering ambulance services.43,44
Over time, many communities adopted a funding model for EMS in which Medicare and Medicaid paid only a portion of the cost of ambulance service provided to their patients, leaving local governments and ambulance providers to cover the remaining costs through other sources of funding such as state grants, local tax subsidies or cost cutting.35 Even with these efforts ambulance agencies struggled to survive. Thus, CMS became an enabler of a poorly functioning EMS system by providing funding to agencies that had no way to make up for funding shortfalls other than by paying very low salaries, allowing unsafe work environments, and keeping ambulances together using duct tape.45,46 Figure 1 illustrates the timeline of EMS funding in the U.S.
Read part two. It covers the design and estimating costs of EMS systems. Part three will publish on August 8 and will cover the conclusions of the study.
Acknowledgements
The authors extend our appreciation to James T. Kerr (KERR Associates, Inc) for his valuable insights and suggestions.
Disclaimers
There was no funding for this project. The authors have no conflicts of interest.
References
1. The National Association of State EMS Officials (NASEMSO), and the Office of EMS, National Highway Traffic Safety Administration (NHTSA), U.S. Department of Transportation. National Emergency Medical Services (EMS) Assessment. 2020. Available at: https://nasemso.org/wp-content/uploads/2020-National-EMS-Assessment_Reduced-File-Size.pdf. Accessed: February 26, 2023.
2. Harrawood D, Gunderson MR, Fravel S, Cartwright K, Ryan JL. Drowning prevention. A case study in EMS epidemiology. J Emerg Med Serv. 1994; 19(6):34.
3. Dickinson ET, Bogucki S, van Gelder CM. EMS on the fireground. Emergency Medical Services: Clinical Practice and Systems Oversight. 2015:363-372.
4. Walz BJ, Bissell RA, Maguire B, Judge JA, 2nd. Vaccine administration by paramedics: a model for bioterrorism and disaster response preparation. Prehosp Disaster Med. 2003; 18(4):321-326.
5. Milsten AM, Maguire BJ, Bissell RA, Seaman KG. Mass-gathering medical care: a review of the literature. Prehosp Disaster Med. 2002; 17(3):151-162.
6. Maguire BJ, O’Neill BJ, Maniscalco PM, Gerard DR, Handal KA. Will an Ambulance Be Available When You Call? Inside Sources. September 10,, 2020. Available at: https://www.insidesources.com/will-an-ambulance-be-available-when-you-call/. Accessed: September 15, 2020.
7. Ioannides KL, Dekker AM, Shin ME, Schriger DL. Ambulances required to relieve overcapacity hospitals: a novel measure of hospital strain during the COVID-19 pandemic in the United States. Ann Emerg Med. 2022; 80(4):301-313. e303.
8. Phelps S. Credits granted for professional education of paramedics and nurses at at US colleges with paired programmes. International Paramedic Practice. 2016; 6(1):6-12.
9. Shah MN. The formation of the emergency medical services system. Am J Public Health. 2006; 96(3):414-423.
10. Walz BJ. Introduction to EMS Systems. Albany, NY: Delmar Publishing; 2001.
11. Al-Shaqsi Sultan. Models of international emergency medical service (EMS) systems. Oman Med Journal. 2010; 25(4):320-323.
12. Kellermann AL, Hsia RY, Yeh C, Morganti KG. Emergency care: then, now, and next. Health Aff (Millwood). 2013; 32(12):2069-2074.
13. Basnawi A. Addressing challenges in EMS Department operations: a comprehensive analysis of key issues and solution. Emergency Care and Medicine. 2023; 1(1):11-23.
14. Jonk Y, Milkowski C, Croll Z, Pearson K. Ambulance Deserts: Geographic Disparities in the Provision of Ambulance Services [Chartbook]. May, 2023. Maine Rural Health Research Center Available at: https://digitalcommons.usm.maine.edu/cgi/viewcontent.cgi?article=1013&context=ems. Accessed: July 28, 2023.
15. Institute of Medicine. The National Academies Press.Emergency Medical Services: At the Crossroads. 2007. Available at: https://www.nap.edu/download/11629. Accessed: March 21, 2021.
16. Girotra S, Dukes KC, Sperling J, et al. Emergency medical service agency practices and cardiac arrest survival. JAMA cardiology. 2024; 9(8):683-691.
17. Byrne JP, Mann NC, Dai M, et al. Association between emergency medical service response time and motor vehicle crash mortality in the United States. JAMA surgery. 2019; 154(4):286-293.
18. Okubo M, Schmicker RH, Wallace DJ, et al. Variation in survival after out-of-hospital cardiac arrest between emergency medical services agencies. JAMA cardiology. 2018; 3(10):989-999.
19. U.S. Centers for Disease Control and Prevention. Emergency Medical Services (EMS): A Look at Disparities in Funding and Outcomes. 2024. Available at: https://www.cdc.gov/ems-community-paramedicine/php/us/disparities.html. Accessed: October 16, 2024.
20. Careless J. CDC Study Reveals Serious EMS Disparities Across U.S. EMS World. November 26, 2024. Available at: https://www.hmpgloballearningnetwork.com/site/emsworld/feature-story/cdc-study-reveals-serious-ems-disparities-across-us. Accessed: March 26, 2024.
21. Maguire BJ, Phelps S, Maniscalco PM, et al. Paramedicine Strategic Planning: Preparing the ‘far forward’ front lines for the second COVID-19 wave. Journal of Emergency Medical Services. May 14, 2020. Available at: https://www.jems.com/2020/05/14/paramedicine-strategic-planning/. Accessed: May 14, 2020.
22. AAA/Avesta. Ambulance Industry Employee Turnover Study. July 2019. Available at: https://ambulance.org/wp-content/uploads/2019/07/AAA-Avesta-2019-EMS-Employee-Turnover-Study-Final.pdf. Accessed: April 19, 2020.
23. Sledge M. New Orleans EMS Has 40% Turnover, Officials Say. J Emergency Medical Services. November 7, 2022. Available at: https://www.jems.com/administration-and-leadership/new-orleans-ems-has-40-turnover-officials-say/. Accessed: April 25, 2023.
24. Maguire BJ, Al Amiry A, O’Neill BJ. Occupational injuries and illnesses among paramedicine clinicians: Analyses of U.S. Department of Labor data (2010 – 2020). Prehosp Disaster Med. 2023; 38(5):581-588.
25. Maguire BJ, O’Neill BJ, Al Amiry A. A cohort study of occupational fatalities among paramedicine clinicians: 2003 through 2020. Prehosp Disaster Med. 2023; 38(2):153-159.
26. Maguire BJ, Maniscalco PM, Gerard DR, et al. Occupational risks for EMS personnel in the United States: Opportunities for OSHA’s proposed Emergency Response Standard to improve EMS safety. EMS1. January 6, 2025. Available at: https://www.ems1.com/ems-advocacy/occupational-risks-for-ems-personnel-in-the-united-states. Accessed: January 7, 2025.
27. Maguire BJ, O’Neill BJ, O’Meara P. Tracking Violence Against EMS: New Research Into an Old Problem. EMS World. 2019; May 28.
28. Zaru B. Regional Variations in Payer Mix and Connecticut's EMS Services. CT Association of Paramedics and EMTs. 2022. Available at: https://www.cga.ct.gov/ph/related/20220721_Sustainability%20and%20Capacity%20of%20EMS%20Services%20in%20CT%20Informational%20Forum/Updated%20EMS%20Regions%20-%20Payer%20Mix%20by%20Hospital%20-%202022%20Atlas%20of%20CT%20EMS_1.pdf. Accessed: April 23, 2025.
29. Hassanein N. What if the ambulance doesn't come? Rural America faces a broken emergency medical system. USA Today. June 26, 2023. Available at: https://www.usatoday.com/story/news/health/2023/06/26/no-ambulances-closing-hospitals-the-crisis-facing-rural-america/70342027007/. Accessed: August 2, 2023.
30. Sheehan A. Greene County's largest provider of EMS services will no longer take 911 calls. CBS/KDKA News. 2024. Available at: https://www.cbsnews.com/pittsburgh/news/greene-county-southwest-ems/. Accessed: March 17, 2025.
31. Wilkinson-Stokes M, Tew M, Yap CY, Crellin D, Gerdtz M. The Economic Impact of Community Paramedics Within Emergency Medical Services: A Systematic Review. Applied Health Economics and Health Policy. 2024; 22(5):665-684.
32. O’Meara P, Stirling C, Ruest M, Martin A. Community paramedicine model of care: an observational, ethnographic case study. BMC Health Serv Res. 2015; 16(1):1-11.
33. Bennhold K. A German Exception? Why the Country’s Coronavirus Death Rate Is Low. New York Times. April 4, 2020. Available at: https://www.nytimes.com/2020/04/04/world/europe/germany-coronavirus-death-rate.html. Accessed: April 14, 2020.
34. O'Meara P, Duthie S. Paramedicine in Australia and New Zealand: A comparative overview. Aust J Rural Health. 2018; 26(5):363-368.
35. Zavadsky M, Wolfberg D. Quantifying the gap between expenses and revenue for EMS services: Takeaways from the First CMS Data Collection Report on Ambulance Services to enhance service levels and reduce costs of service delivery. EMS1. 2025. Available at: https://www.ems1.com/ems-trend-report/quantifying-the-gap-between-expenses-and-revenue-for-ems-services. Accessed: March 15, 2023.
36. U.S. National Highway Traffic Safety Administration, National EMS Advisory Council. EMS Funding and Reimbursement. 2016. Available at: https://www.ems.gov/NEMSAC-advisories-and-recommendations/2016/NEMSAC_Final_Advisory_EMS_System_Funding_Reimbursement.pdf. Accessed: August 14, 2021.
37. Munjal KG, Margolis GS, Kellermann AL. Realignment of EMS reimbursement policy: new Hope for patient-centered out-of-hospital care. JAMA. 2019; 322(4):303-304.
38. Medpac. Ambulance Services Payment System. October 2024. Available at: https://www.medpac.gov/wp-content/uploads/2024/10/MedPAC_Payment_Basics_24_ambulance_FINAL_SEC.pdf. Accessed: April 23, 2025.
39. Mulcahy AW, Heins SE, Rasmussen PW, et al. Medicare Ground Ambulance Data Collection System (GADCS); Report Year 1 and Year 2 Cohort Analysis. RAND Health Care. 2024. Available at: https://www.cms.gov/files/document/medicare-ground-ambulance-data-collection-system-gadcs-report-year-1-and-year-2-cohort-analysis.pdf. Accessed: March 15, 2025.
40. Zavadsky M, Wolfberg D. Takeaways from the First CMS Data Collection Report on Ambulance Services – And What we Need to Do About It. EMS|MC. 2025. Available at: https://emsmc.com/in-the-news/takeaways-from-the-first-cms-data-collection-report-on-ambulance-services-and-what-we-need-to-do-about-it/. Accessed: April 23, 2025.
41. Walz BJ, Krumperman KM, Zigmont JJ, Walz BJ. Foundations of EMS systems. 2nd ed. Clifton Park, NY: Delmar Cengage Learning; 2011.
42. Medicare Program; Fee Schedule for Payment of Ambulance Services and Revisions to the Physician Certification Requirements for Coverage of Nonemergency Ambulance Services. 2002. Available at: https://www.federalregister.gov/documents/2002/02/27/02-4548/medicare-program-fee-schedule-for-payment-of-ambulance-services-and-revisions-to-the-physician#:~:text=SUMMARY:,coverage%20of%20nonemergency%20ambulance%20services. Accessed: April 14, 2025.
43. Digitech. CMS Cost Reporting in 2023 and the Impact on EMS & Ambulance Medicare Reimbursement: Where Are We Now? 2023. Available at: https://digitechcomputer.com/cms-cost-reporting-2023-and-ems-ambulance-medicare-reimbursement/#:~:text=In%202002%2C%20Medicare%20implemented%20a,ambulance%20costs%20versus%20other%20costs. Accessed: April 22, 2025.
44. U.S. General Accounting Office. Ambulance Services: Medicare Payments Can Be Better Targeted to Trips in Less Densely Populated Rural Areas. 2003. Available at: https://www.gao.gov/assets/a239813.html#:~:text=In%202002%2C%20CMS%20implemented%20a%20new%20Medicare,have%20reported%20greater%20difficulty%20maintaining%20adequate%20staff. Accessed: April 22, 2025.
45. Staff. Duct tape mended ambulance fleet under investigation. EMS1. Oct. 15, 2014. Available at: https://www.ems1.com/ambulance-service/videos/duct-tape-mended-ambulance-fleet-under-investigation-48SZvJKlvsbsO9f1/. Accessed: August 20, 2021.
46. Frau L. State EMS system 'close to collapsing' without funding, ambulance chief warns. North Jersey. 2024. Available at: https://www.northjersey.com/story/news/new-jersey/2024/05/13/ems-chief-warns-ambulance-system-close-to-collapsing/73592723007/. Accessed: March 17, 2025.