Don’t Shock That: Pacemaker Tachycardia During Ground Transport
Abstract
This paper examines two incidents of pacemaker tachycardia (PT) on the same critical care transport (CCT) unit seven months apart. Both cases involved rate-responsive pacemakers causing tachycardia during ground transport. In both cases, tachycardia appeared within two minutes of leaving the sending facility. The heart rate increased and decreased with the speed of the ambulance, and the phenomenon resolved within a minute after stopping at the receiving facility. Neither patient required intervention during the PT event.
One finding from Case 1 stands out when discussing the etiology of PT—high RPM of the ambulance while idling at the receiving facility produced no rate changes. This suggests that the cause is likely vibration rather than electromagnetic interference.
The primary concern with PT is misidentification. PT can cause a wide-complex QRS, which can be mistaken for ventricular tachycardia. Misidentification of PT could lead a provider to treat PT as ventricular tachycardia, potentially causing harm to the patient.
PT has been documented in aeromedical transport since 1989. However, there is no documentation of PT in ground ambulance transport in the literature, although anecdotal accounts have been noted.
Introduction
Pacemakers are common. Any EMT, medic, or CCT provider who has spent time on an ambulance has transported a patient with one. What most of us weren’t taught is that ground or air transport itself may trigger pacemaker dysfunction and cause pacemaker tachycardia (PT).
Rate-responsive pacemakers are designed to increase the patient’s heart rate when the body’s demand is higher, such as walking or exercising. They adjust the heart rate by sensing motion, vibration, or physiological changes and responding accordingly. This becomes a problem when the sensor cannot tell the difference between physical activity and other stimuli, such as air or ground transport with vibration.
PT has been documented in aeromedical transport going back as far as 1989. Studies on helicopter transport identified vibration and electromagnetic interference as the probable culprits. The takeaway from the literature is that the risk of PT exists, the incidence is low, and providers should be aware of it.
Ground transport is a different story. There are no published studies and no case reports. Anecdotal accounts of PT exist among CCT providers, but nothing is in print.
This paper looks at two cases of PT during CCT transport. Both cases involve rate-responsive pacemakers and each resolved upon arrival at the receiving facility. The goal of this article is to educate EMS providers about PT, and more importantly, what not to do when they see it.
CASE 1: Loma Linda University Medical Center to St. Bernardine’s Medical Center
The patient was a 76-year-old female being transferred from Loma Linda University Medical Center to St. Bernardine’s Medical Center. The patient had a history of a recent witnessed cardiac arrest, myocardial infarction, coronary artery disease, diabetes mellitus, and a permanent pacemaker. She was intubated and sedated on a propofol drip and SIMV on the ventilator. The patient responded to sternal rub only.
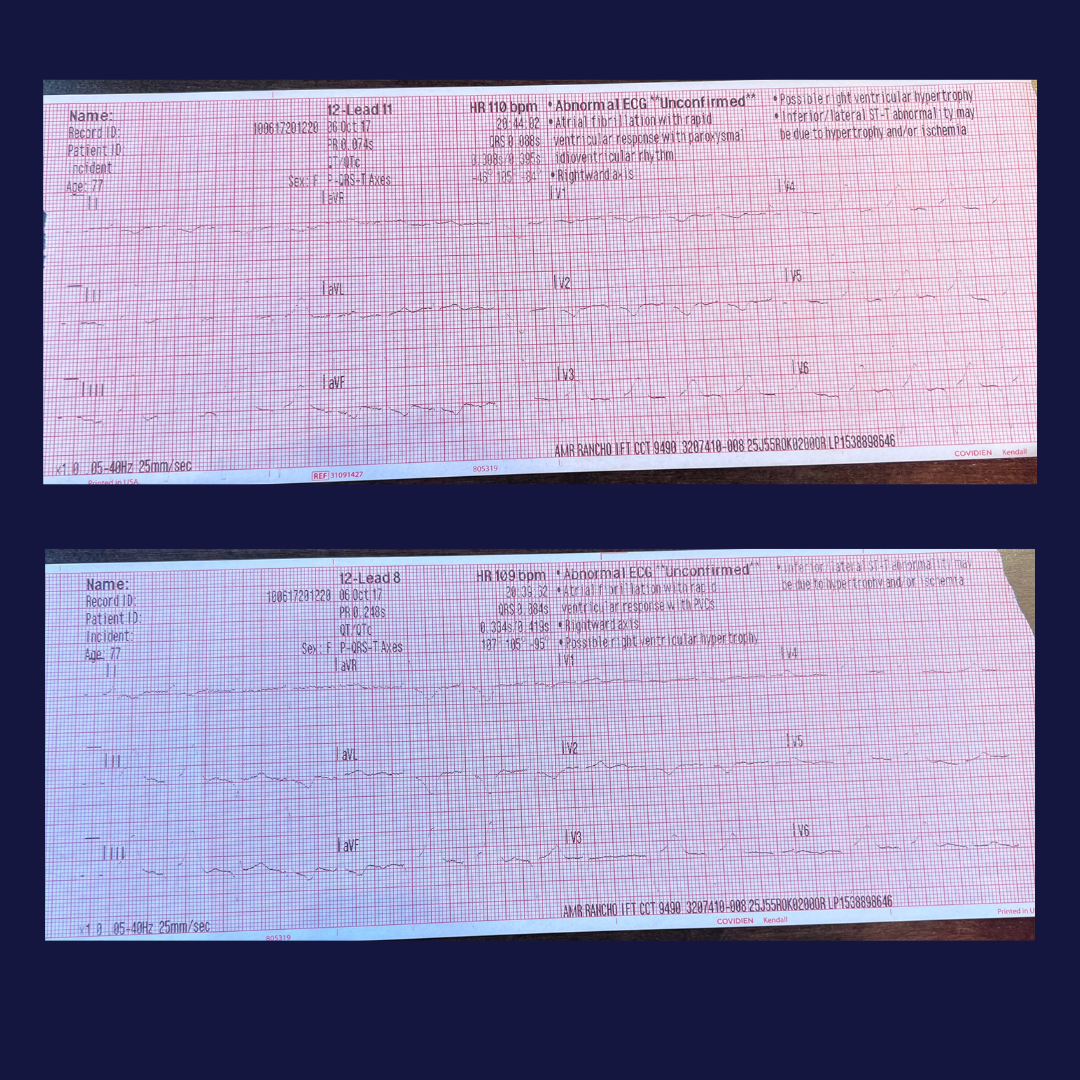
The baseline EKG showed normal sinus rhythm with a heart rate of 70, with no variability. All other vital signs were within normal limits.
Within two minutes of leaving the sending facility, the EKG changed. The QRS widened, and the pacemaker started firing faster than the 70 beats per minute seen at baseline. The heart rate was variable, ranging from the 80s to 110s. Interestingly, the heart rate tracked with the speed of the ambulance—it climbed as the ambulance accelerated and dropped as the ambulance decelerated. The blood pressure, pulse oximetry, respirations, and level of consciousness showed no changes during the tachycardia; therefore, no treatment was initiated.
Once the CCT unit arrived at the destination, the patient’s heart rate went back to baseline within a minute. One important thing to note is that while the ambulance was idling at higher RPMs, there was no rate change.
CASE 2: Redlands Community Hospital to Kaiser Permanente Ontario
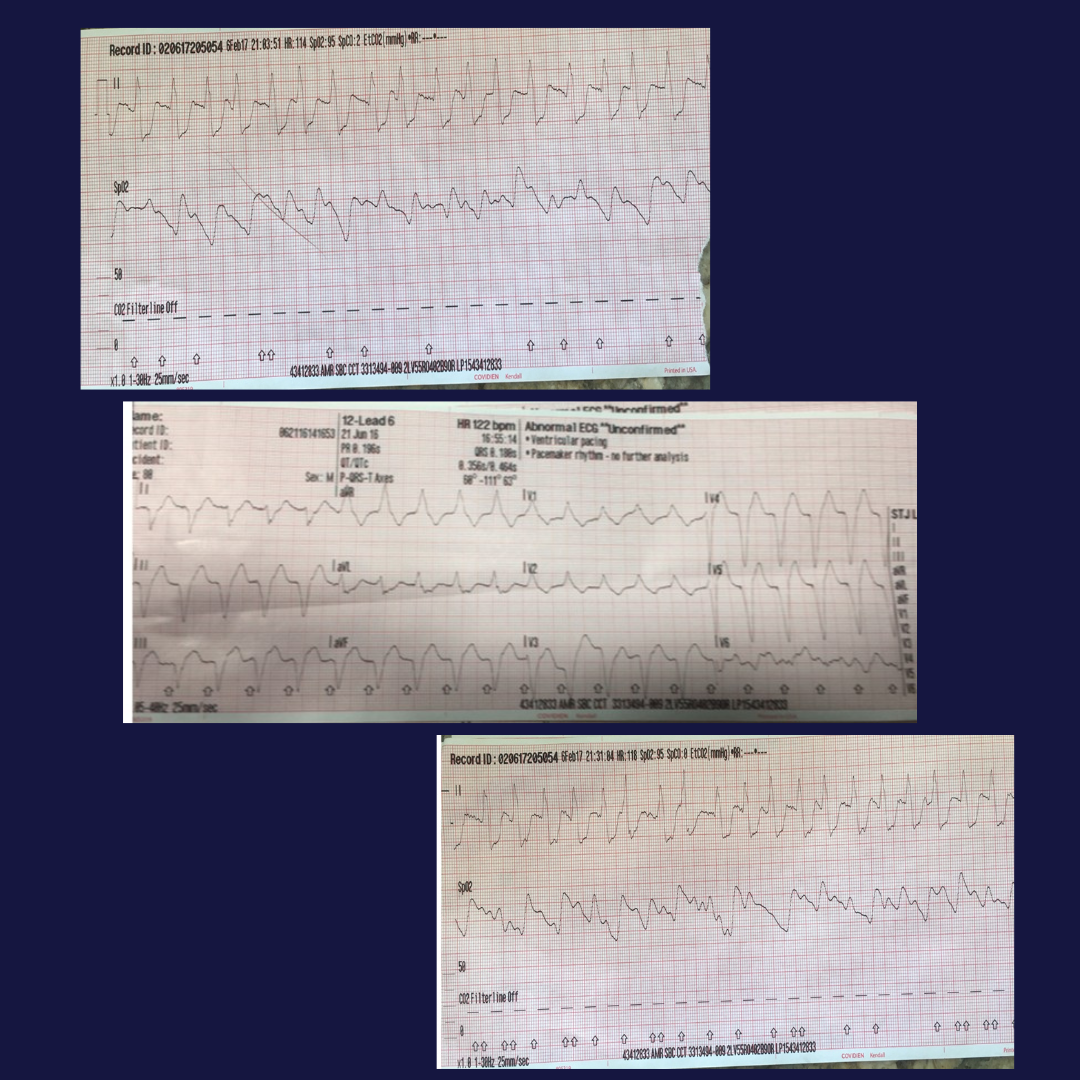
Seven months later, the same CCT unit transported an 87-year-old female for repatriation due to insurance. The patient had a history of pneumonia and was Bi-PAP dependent. Her medical history included congestive heart failure, coronary artery disease, and a rate-responsive pacemaker. The day prior, an ALS unit had attempted to transport the patient, but she developed a wide-complex tachycardia and they diverted back to Redlands Community Hospital for stabilization.
On assessment, the patient was alert and oriented x 1 with a Glasgow Coma Scale of 14. The EKG showed normal sinus rhythm at a rate in the 90s. All other vital signs were within normal limits.
Just as the ALS unit saw, the CCT witnessed a wide-complex QRS tachycardia, which was variable with the speed of the ambulance. The patient remained hemodynamically stable, with no complaints and no changes in mentation. Transport continued, and upon arrival, the heart rate returned to baseline without any issues.
Discussion
Both cases share the same pattern. PT appeared within two minutes of leaving the sending facility, the heart rate tracked directly with the speed of the ambulance, and the PT resolved within a minute at the receiving facility. Two separate cases, seven months apart, with the same CCT are not a coincidence.
Case 1 offers a critical clue about the cause of PT. While the ambulance idled in the bay of the receiving facility with higher RPMs, there was no rate change. The engine was running, the radios were active, and the AC inverter was producing 60Hz electrical noise; however, the pacemaker did not respond. Only when the ambulance was moving and road vibration was transmitted to the patient did the heart rate increase. This observation is important: if electromagnetic interference (EMI), electrical disruption from the inverter, radios, and monitors. or 60Hz noise were the primary cause, one would expect to see changes during idling. Vibration is the more likely culprit.
Two distinct mechanisms are worth understanding, even if one is more probable than the other. EMI covers any disruption caused by an external electromagnetic field; on an ambulance, that includes 60Hz inverter noise, radio signals, and monitor output. Vibration reaches the patient through mechanical means: road surface irregularities, the suspension of the ambulance, the drivetrain, and the stretcher legs and locking mechanism. In either case, the rate-responsive pacemaker interprets the stimulus as physical activity and causes an increased heart rate as if the patient were walking or exercising. It cannot distinguish between the two.
The clinical concern of PT in the field is misidentification. PT is easily mistaken for ventricular tachycardia on the monitor due to its wide QRS and rapid rate. This is where the real danger lies. Cardioverting or pushing antiarrhythmics on a ventricular paced rhythm could seriously harm the patient. If the patient is stable with normal vital signs, assess whether the heart rate varies with vehicle speed before reaching for the drug box or pads.
Management options are limited. Placing a magnet over the pacemaker disables the rate-response function; however, this requires having the magnet and an MD’s order to do so. Basic life support providers are not likely to identify PT, as EKG interpretation is not within that scope of practice. ALS and CCT providers are more likely to identify PT, and continuing transport is indicated unless decompensation occurs.
PT likely happens more than we know. CCT providers have anecdotally noted PT, but it hasn’t been documented in print until now. Further research is needed to better understand pacemaker response to vibration frequencies and EMI levels in ground ambulances.
Limitations
This paper is limited by its small sample size. Two cases from a single CCT unit cannot establish incidence rates or confirm mechanism. The value here is documentation. These cases establish that PT during ground transport occurs and warrants further investigation.
Conclusion
Pacemaker tachycardia during ground transport is real. Two cases, same CCT unit, seven months apart. It's been documented in helicopter transport since 1989.
The clinical takeaway is simple. For wide-complex tachycardia in a pacemaker patient, assess whether heart rate tracks with vehicle speed before intervening. If vital signs are stable, monitoring is all that is warranted.
As for why it happens, vibration is the likely culprit. The idling observation from Case 1 makes a strong case for that. But more research is needed, specifically looking at ground transport EMI levels and vibration frequencies.
PT is rare, but misidentify it, and you'll treat the wrong arrhythmia in a patient who didn't need treatment.