Pedicled Vastus Lateralis and Tensor Fascia Lata Flap for Aortic Graft Salvage
© 2025 HMP Global. All Rights Reserved.
Any views and opinions expressed are those of the author(s) and/or participants and do not necessarily reflect the views, policy, or position of ePlasty or HMP Global, their employees, and affiliates.
Questions
- What is the incidence of aortic graft infection? What patient and surgical factors are associated with graft infection? What complications may arise if untreated?
- What factors are associated with successful salvage of vascular grafts?
- What muscle flaps can be considered for aortic graft coverage?
- What is the reach of a pedicled vastus lateralis flap and what maneuvers may be performed to increase its reach?
Case Description
A 70-year-old man with retroperitoneal liposarcoma statis post-neoadjuvant radiation, radical resection, and abdominal aortic reconstruction presented with recurrent retroperitoneal abscess and entero-enteric and entero-cutaneous fistulae consistent with a contaminated abdomen. Following failed conservative management with intravenous antibiotics and percutaneous drainage, he was taken for surgical graft salvage with flap coverage (Figure 1). Various reconstructive options were considered. Local retroperitoneal flaps were in the radiated field. An omental flap was used in index operation and was necrotic. The nephrectomy scar precluded a rectus flap and, given the degree of muscle wasting, a rectus femoris flap was deemed too small. Given the size of the defect, a combined vastus lateralis and tensor fascia lata flap was chosen. The vastus lateralis and tensor fascia lata were identified (Figure 2). The flap was dissected free and the arc of rotation confirmed (Figure 3). Finally, the flap was tunneled through the rectus sheath and inset without tension in the retroperitoneum over the aortic graft (Figure 4). The patient had a prolonged hospital course, but no complications were noted relating to the vastus lateralis flap or aortic graft. He was discharged to a nursing facility 2 months postoperatively and, at his final visit 1 year postoperative, there was no evidence of aortic graft compromise or infection.
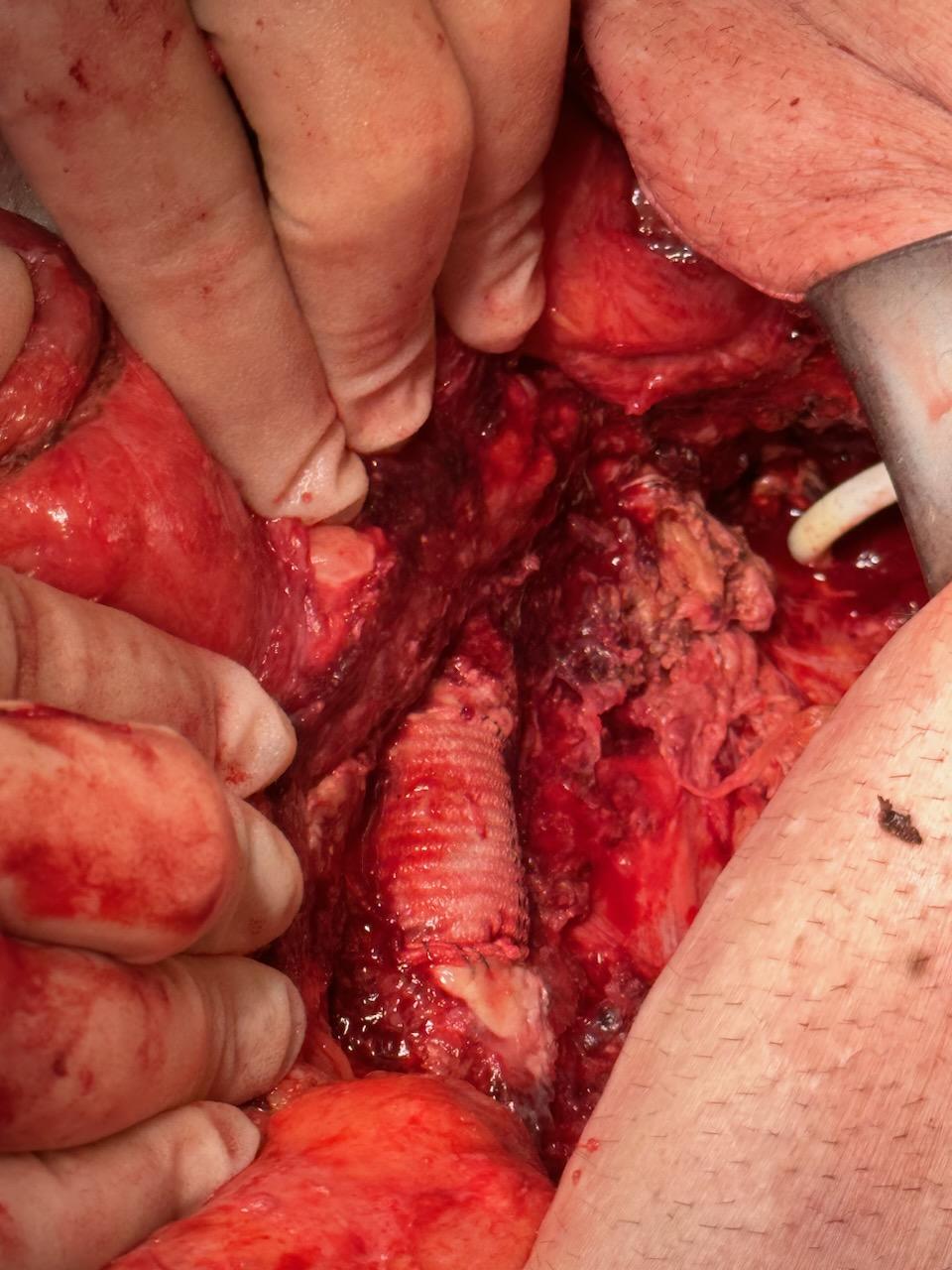
Figure 1. Exposed aortic graft in the retroperitoneum with necrotic omentum.

Figure 2. Suprafascial dissection of vastus lateralis and tensor fascia lata.

Figure 3. Pedicled vastus lateralis/tensor fascia lata flap arc of rotation.
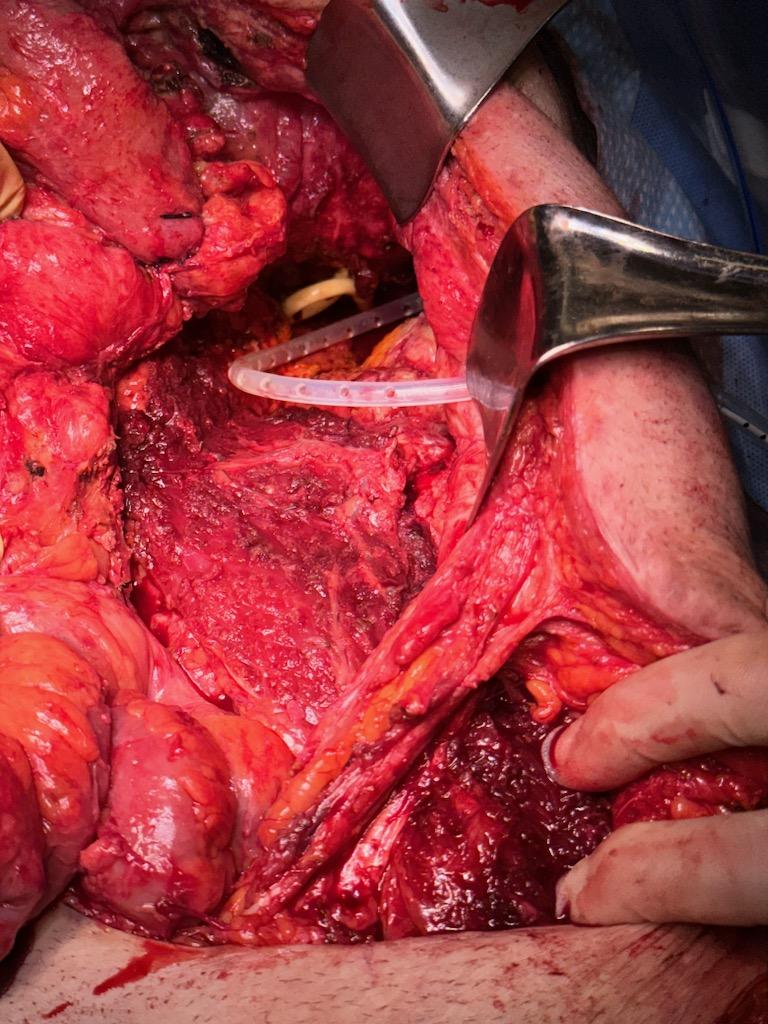
Figure 4. Tension-free flap inset over aortic graft in the retroperitoneum.
Q1. What is the incidence of aortic graft infection? What patient and surgical factors are associated with graft infection? What complications may arise if untreated?
Graft infection complicates 4% of all aortic reconstructions.1 Independent risk factors for graft infection comprise both patient and surgical factors, including diabetes, immunosuppression, malnutrition, groin access, open wound at time of procedure, emergency procedure, and need for early reoperation in the early postoperative period.1 Infection typically arises from direct inoculation of the graft or peri-graft space. The most common causative organism is coagulase-negative Staphylococcus spp.1,2 Aortic graft infection has a high morbidity and may result in sepsis, aneurysm formation, thrombosis, and distal embolization. If untreated, graft infection causes erosion between the graft and the surrounding bowel, urinary tract, or skin, and may lead to potentially catastrophic aortic fistulae in 1% to 2% of patients undergoing aortic reconstruction.
Q2. What factors are associated with successful salvage of vascular grafts?
Standard treatment of exposed grafts involves extended parental antibiotic therapy and resection of the exposed segment with extra-anatomic bypass. The use of muscle flaps for graft salvage has evolved from its origins in the 1980s to become more common today.3 Muscle flaps provide a well-vascularized tissue bed to eliminate dead space, enhance local tissue oxygenation, and deliver intravenous antibiotics and immune cells. Muscle-flap graft salvage has been shown to reduce bacterial counts, increase salvage rates, and accelerate healing time. Recent studies advocate for attempted vascularized tissue salvage without graft excision if no fistula is present.4 Timing is key, with earlier time to coverage associated with increased graft salvage.3,4
Q3. What muscle flaps can be considered for aortic graft coverage?
Several factors are considered when it comes to flap selection including the location, size of the defect, structures involved, and presence of contamination. Pedicled flaps are advantageous in that they require a shorter operating time and decrease the time for tissue resorption.5 First-line local flaps include retroperitoneal flaps with psoas muscle and intra-abdominal omental flaps. Regional flaps such as rectus abdominis or reversed latissimus dorsi may then be considered. Next, more distal pedicled flaps may be considered, including the rectus femoris, vastus lateralis, or tensor fascia lata. Conversion of pedicled flap to free-tissue transfer, or direct free-tissue transfer is always an option in the case of insufficient reach or lack of available pedicled flaps. In this case, a rectus flap was not possible because of the previous nephrectomy scar, which compromised the potential vascularity and reach of a rectus flap. A rectus femoris was deemed too small given the degree of muscle wasting the patient had undergone. A pedicled vastus lateralis-tensor fascia lata graft was chosen to cover the graft and prevent a potentially catastrophic aorto-enteric fistula.
Q4. What is the reach of a pedicled vastus lateralis flap and what maneuvers may be performed to increase its reach?
The vastus lateralis and its overlying anterolateral thigh skin island has been a workhorse pedicled flap for defects from the upper third of the thigh to the epigastrum.6 The pedicled vastus lateralis flap may comfortably cover defects below the umbilicus; however, for defects above, additional maneuvers must be used.6 Maneuvers that may increase reach of the flap to the maximum cranial reachable distance include dissecting the descending lateral circumflex pedicle to its origin, raising the vastus lateralis and tensor fascia lata as a composite unit to incorporate the horizontal branch of the descending lateral circumflex, passing the flap deep to the rectus femoris and sartorius, ligating the branch to the rectus femoris if originating from the descending lateral circumflex artery (type 2 pattern), and, if raised as a myocutaneous flap, shifting the skin.6 Finally, the hip may be flexed up 30° to 60° to reach up to the epigastrium; however, the patient must maintain this flexed position for several days to reduce tension on the pedicle and allow for healing before the hip is extended.7
Acknowledgments
Authors: Dieter Brummund, MD1; Angela Chang, MD2; Vanitha Vasudevan, MD3; Tony Shao, MD4; Christopher Salgado, MD5
Affiliations: 1Larkin Community Hospital, Miami, Florida; 2HCA Florida – Mercy Hospital, Miami, Florida; 3Palmetto General Hospital, Miami, Florida; 4University of Miami, Miami, Florida; 5Constructive Surgery Associates, Miami, Florida
Correspondence: Dieter Brummund, MD, Larkin Community Hospital, Miami, FL 33143, USA. E-mail: dbrummund@larkinhospital.com
Ethics: This review of 1 case and publicly available published literature was exempt institutional review board approval.
Disclosures: Dr Salgado is a speaker for Sanara MedTech, the manufacturer of CellerateRX Surgical Powder. The remaining authors disclosed no financial or other conflicts of interest.
References
- Tsapralis D, Charalampopoulos A, Lazaris AM. Abdominal aortic graft infection. In: Grundmann RT, ed. Diagnosis, Screening, and Treatment of ABdominal, Thoracoabdominal and Thoracic Aortic Aneurysms. IntechOpen; 2011. doi: 10.5772/18514
- Wilson WR, Bower TC, Creager MA, et al; American Heart Association Committee on Rheumatic Fever, Endocarditis, and Kawasaki Disease of the Council on Cardiovascular Disease in the Young; Council on Cardiovascular and Stroke Nursing; Council on Cardiovascular Radiology and Intervention; Council on Cardiovascular Surgery and Anesthesia; Council on Peripheral Vascular Disease; and Stroke Council. Vascular graft infections, mycotic aneurysms, and endovascular infections: a scientific statement from the American Heart Association. Circulation. 2016;134(20):e412-e460. doi:10.1161/CIR.0000000000000457
- May BL, Zelenski NA, Daluvoy SV, Blanton MW, Shortell CK, Erdmann D. Salvage of exposed groin vascular grafts with early intervention using local muscle flaps. Plast Reconstr Surg Glob Open. 2015;3(9):e514. doi:10.1097/GOX.0000000000000480
- Shijo T, Matsuda H, Yokawa K, et al. The impact of vascularized tissue flap coverage on aortic graft infection with and without infected graft excision. Eur J Cardiothorac Surg. 2021;60(5):1043-1050. doi:10.1093/ejcts/ezab179
- Di Summa PG, Watfa W, Campisi C, et al. Free versus pedicled anterolateral thigh flap for abdominal wall reconstruction. Anticancer Res. 2019;39(12):6759-6768. doi:10.21873/anticanres.13891
- Tamai M, Nagasao T, Miki T, Hamamoto Y, Kogure T, Tanaka Y. Rotation arc of pedicled anterolateral thigh flap for abdominal wall reconstruction: how far can it reach? J Plast Reconstr Aesthet Surg. 2015;68(10):1417-1424. doi:10.1016/j.bjps.2015.06.010
- Ting J, Trotter D, Grinsell D. A pedicled anterolateral thigh (ALT) flap for reconstruction of the epigastrium: case report. J Plast Reconstr Aesthet Surg. 2010;63(1):e65-e67. doi:10.1016/j.bjps.2009.05.025