Peer Reviewed
Rare Benign Tumor: Elastofibroma Dorsi
© 2025 HMP Global. All Rights Reserved.
Any views and opinions expressed are those of the author(s) and/or participants and do not necessarily reflect the views, policy, or position of ePlasty or HMP Global, their employees, and affiliates.
Questions
- What are the main characteristics of elastofibroma dorsi?
- How is elastofibroma dorsi diagnosed?
- How is a patient with elastofibroma dorsi managed?
- What are the possible complications and what is the long-term prognosis?
Case Description
A 74-year-old woman with a history of hypertension and no history of smoking presented with bilateral tumors situated under the scapula; the tumors had been evolving for several years and had begun to cause pain with shoulder movement. Computed tomography scan showed an 86 x 38-mm mass on the right side and a 73 x 22-mm mass on the left side; radiologists suggested the diagnosis of elastofibroma dorsi. The patient underwent surgery with the excision of both tumors, and histopathology confirmed the initial diagnosis.
Q1. What are the main characteristics of elastofibroma dorsi?
Elastofibroma dorsi is a rare, benign tumor that is mostly observed in women 60 years and older in the subscapular region with chronic back pain, which is more intense when moving the shoulders. It is common for this tumor to be bilateral.1 However, in less than 1% of cases, the tumors can be found in different locations, such as near the ischial tuberosity, the olecranon, or within the thoracic wall. In addition to this, even though most of the tumors are bilateral, it has been shown that they have a preference for the right side of the thorax and, in bilateral cases, the right tumor is generally larger.2 This supports the most accepted theory that chronic, repetitive mechanical stress leads to the overproduction of elastic tissue and eventually forms this kind of pathology.3 Our case fits this description because our patient performed manual labor for her entire career, and the right-sided tumor has a larger mass than the tumor on the left side.
Q2. How is elastofibroma dorsi diagnosed?
In order to achieve an accurate diagnosis of elastofibroma, clinical signs, non-specific imaging findings, histopathological examination, and slow progression with benign characteristics are crucial. In this specific area, other tumors—both benign or malignant—can be found and mistaken for an elastofibroma dorsi, such as chondromas, lipomas, low-grade liposarcomas, and fibrolipomas.4
Two tumors could be palpated in our case: the right-sided tumor with a 7-cm diameter, and the left-sided tumor with a 5-cm diameter. Both tumors were relatively well-defined, firm, with submuscular localization, non-adherent to the skin, variable with the movement of the arm, and painful when being mobilized.
Computed tomography findings may be highly suggestive of this pathology, most commonly showing a poorly defined soft-tissue mass with attenuation similar to the adjacent skeletal muscle and having internal striations or scattered areas of fat. Studies show that the smaller the tumor, the more homogenous attenuation will show on a computed tomography scan.5
Similar characteristics have been shown on our patient’s computed tomography scan; the tumors were situated posterior to the serratus muscles and anterior to the latissimus dorsi and scapular plane (Figures 1 and 2).

Figure 1. Computed tomography scan of the patient showing the 2 tumors situated anterior to the scapular plane.
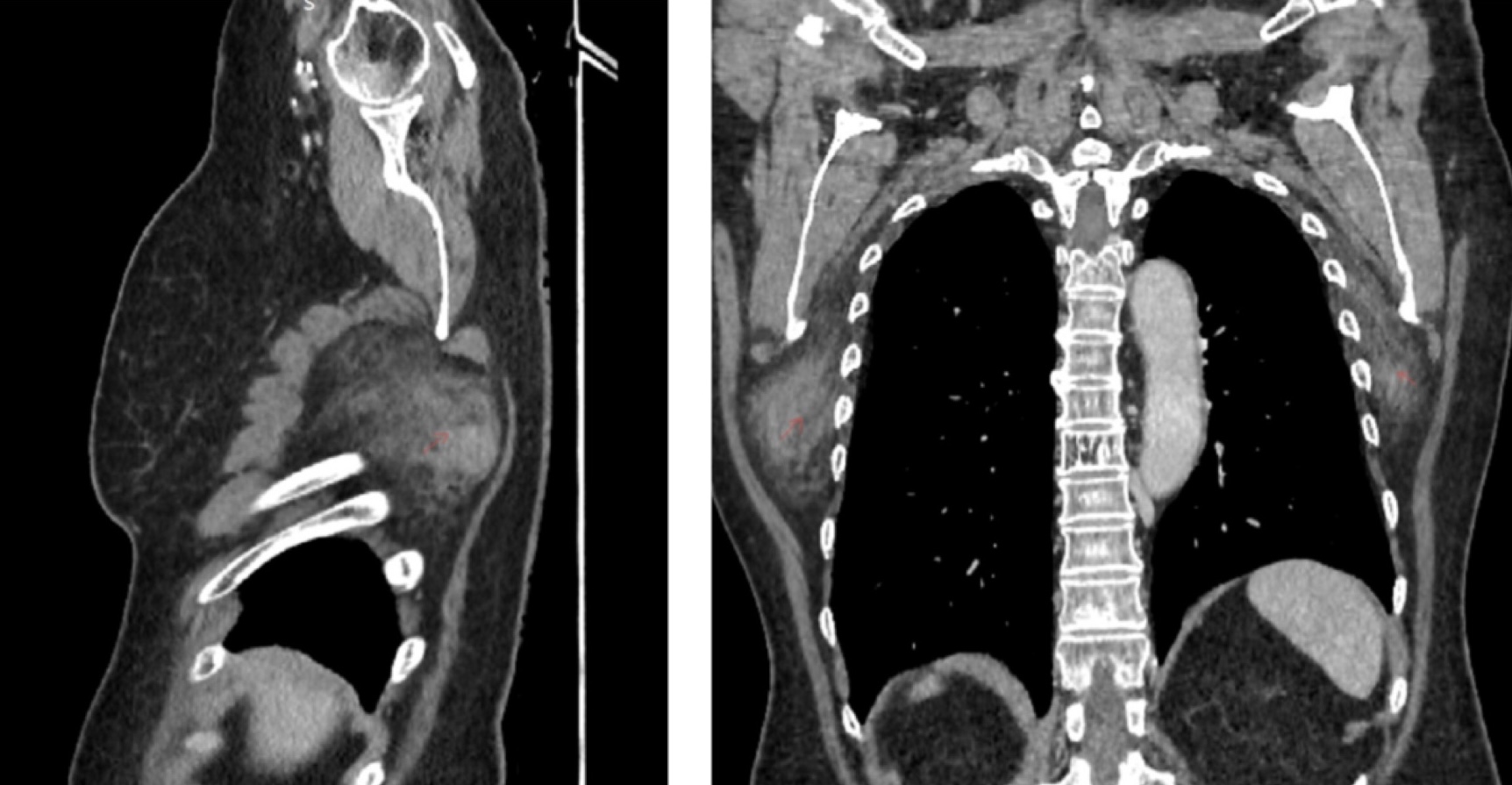
Figure 2. Computed tomography scan from an anterior and lateral perspective.
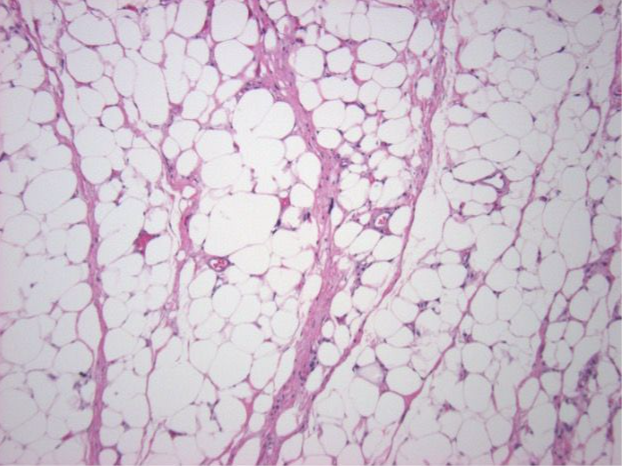
The final evaluation that confirmed the elastofibroma was the histopathologic examination, which analyzed fragments from both tumors that consisted of thick, fibrous bands between layers of adipous tissue.
Q3. How is a patient with elastofibroma dorsi managed?
Because this tumor can be diagnosed with a computed tomography scan or magnetic resonance imaging, the excision of asymptomatic, small elastofibroma is not needed because malignant characteristics or transformation have never been reported. Radiotherapy could be an option for cases that are unresectable because of their localization.6
Our patient started to develop pain both during shoulder movement and during rest, so resection was the only choice. A parallel incision was made 2 cm under the scapula on both sides, and dissection through the latissimus dorsi was performed showing 2 tumors; both were round-shaped, adherent to the serratus muscle, and followed by marginal excision of the tumoral mass (Figure 3). Even if good hemostasis was achieved, 1 drain was placed on each side to mitigate the high risk of seromas and hematomas caused by the dead space and extensive dissection area. The drains were removed after 5 days when less than 50 mL per 24 hours were collected (Figure 4). During the 5 days of drainage, the patient received antibiotics and daily dressing changes.
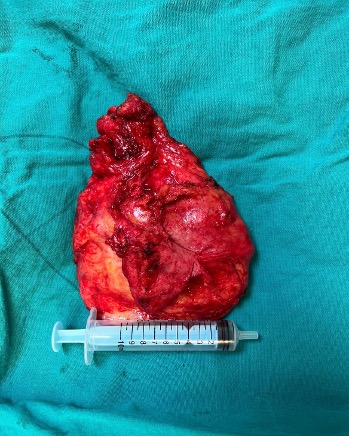
Figure 3. Right-sided tumor measuring 7 x 8 cm (5-cm syringe for scale).

Figure 4. The empty space left after resection of the right-side tumor. Some of the serratus muscle and ribcage can be observed.
Q4. What are the possible complications and what is the long-term prognosis?
The incidence of hematomas or seromas is high after this kind of resection, and excision is discouraged if the case is not symptomatic. Hematomas prolong the hospital stay and involve more invasive maneuvers such as puncture, immobilization, or even surgical evacuation. In order to reduce the incidence of this complication, good hemostasis must be achieved during surgery and negative pressure through the drainage tube should be applied.7 Other possible complications that the surgeon may encounter are infections, wound dehiscence, or prolonged wound drainage.
In the case presented here, the wound drainage ceased after 5 days and no hematomas or seromas were encountered. The patient stated that pain with shoulder movement stopped 1 month after surgery. Because of the benign characteristics of this tumor, no other treatment is necessary after marginal excision.
Acknowledgments
Authors: Adrian Frunza, MD, PhD; Luca Avram, MD
Affiliation: Bucharest Emergency Clinical Hospital, Bucharest University School of Medicine, Romania.
Correspondence: Luca Avram MD; luca_avr@yahoo.com / luca.avram@rez.umfcd.ro
Disclosures: The authors disclose no financial or other conflicts of interest.
References
- Battaglia M, Vanel D, Pollastri P, et al. Imaging patterns in elastofibroma dorsi. Eur J Radiol. 2009;72(1):16-21. doi:10.1016/j.ejrad.2009.05.024
- Ochsner JE, Sewall SA, Brooks GN, Agni R. Best cases from the AFIP: elastofibroma dorsi. RadioGraphics. 2006;26(2):1873-1876. doi:10.1148/rg.266055184
- Karrakchou B, Yaikoubi Y, Chairi MS, Jalil A. Elastofibroma dorsi: case report and review of the literature. Pan Afr Med J. 2017;28:34. doi:10.11604/pamj.2017.28.34.13675
- Neagoe O, Faur CI, Ionică M, Baderca F, et al. Elastofibroma dorsi, a rare condition, with challenging diagnosis. Case report and literature review. Medicina. 2021;57(4):370. doi:10.3390/medicina57040370
- Naylor MF, Nascimento AG, Sherrick AD, McLeod RA. Elastofibroma dorsi: radiologic findings in 12 patients. AJR Am J Roentgenol. 1996;167(3):683-687. doi:10.2214/ajr.167.3.8751681
- Sarici IS, Basbay E, Mustu M, et al. Bilateral elastofibroma dorsi: a case report. Int J Surg Case Rep. 2014;5(12):1139-1141. doi:10.1016/j.ijscr.2014.10.032
- Nagano S, Yokouchi M, Setoyama T, et al. Elastofibroma dorsi: surgical indications and complications of a rare soft tissue tumor. Mol Clin Oncol. 2014;2(3):421-424. doi:10.3892/mco.2014.257