Extraction of a TASER 7 Barb Embedded in the Supraorbital Frontal Bone: A Clinical Case Report
© 2025 HMP Global. All Rights Reserved.
Any views and opinions expressed are those of the author(s) and/or participants and do not necessarily reflect the views, policy, or position of ePlasty or HMP Global, their employees, and affiliates.
Abstract
Hand-held conducted energy devices, such as the TASER 7 (Axon Enterprise, Inc), are commonly used by law enforcement as a method of "non-lethal" force. However, their use may result in serious injuries. The authors report a case where a TASER 7 barb became embedded in the left supraorbital frontal bone during a field incident. Initial removal attempts were unsuccessful when the cylindrical cartridge broke off. Ultimately, the barb was successfully removed at bedside with a Kocher clamp and firm, constant in-line traction under local anesthesia at a tertiary hospital. This case highlights the potential complications associated with conducted energy devices and provides a bedside removal technique that avoids the need for operative intervention.
Introduction
Law enforcement frequently uses handheld conducted energy devices (CEDs), also known as conducted electrical weapons, to subdue individuals. These devices generate a high-voltage arc of 50 000 volts when deployed, followed by the release of probes, which consist of sharp barbs attached to cylindrical metal shafts. Each probe is connected to the CED by thin wires that transmit the electrical charge. Upon impact, the barb penetrates the skin and underlying tissues, delivering the electrical current and anchoring the probe in place, potentially causing minor electrical burns and secondary injuries.1
The TASER 7 (Axon Enterprise, Inc) is a newer model designed with a heavier and faster probe, leading to deeper tissue penetration because of its increased kinetic energy and momentum. This model features a flatter barb, which is part of the probe that embeds into the target. The probe's shaft, connected to a base plate, deploys the attached cable during flight, making it more challenging to remove once embedded.2 This case report focuses on the extraction of a TASER 7 probe that became lodged in the supraorbital frontal bone without requiring surgical intervention.
Case Presentation
A 25-year-old man evaded apprehension by law enforcement, necessitating the user of a TASER 7. This resulted in 1 barb penetrating the left upper leg and another being embedded just above the left eyebrow in line with the lateral canthus (Figure 1). The patient was taken to a community hospital, where the barb from his left thigh was removed. However, upon attempted removal of the barb embedded above the brow, the cylindrical cartridge became detached and the barb remained embedded in his left forehead. Further attempts at extraction of the barb failed, prompting transfer to a tertiary hospital for facial trauma evaluation. Non-contrast head computed tomography (CT) imaging revealed a metallic object lodged in the left supraorbital soft tissues, with a 6-mm linear structure projecting into the supraorbital frontal bone. The scan also showed a small amount of adjacent subcutaneous gas, a left occipital scalp laceration, and no intracranial hemorrhage or ocular trauma (Figure 2).

Figure 1. Image of the patient with a TASER 7 barb (Axon Enterprise, Inc) in his forehead.
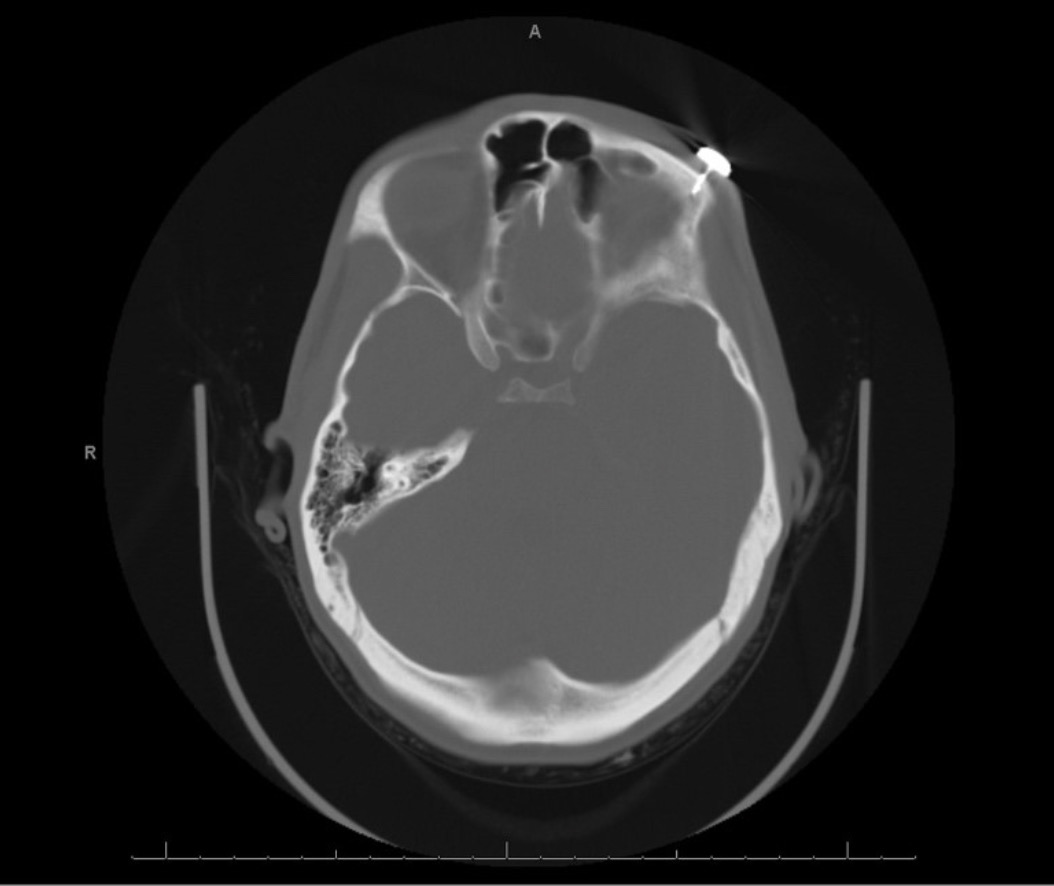
Figure 2. Image of the axial computed tomography scan showing penetration of the supraorbital frontal bone.
Upon examination, the patient exhibited normal facial symmetry and functional strength. Neurological assessment confirmed he was alert and oriented, and an ophthalmology consultation found no ocular pathology. With the patient's consent, bedside removal of the barb was attempted. The area was prepped with half-strength betadine, and 2g of cefazolin were administered intravenously (IV) preprocedure. Analgesia was obtained with local anesthetic (lidocaine 1%, 3 mL), and initial attempts at removal were performed utilizing the fulcrum method3; however, these attempts were unsuccessful because of unfavorable facial anatomy. The barb was then gripped with a Kocher clamp and removed with firm, constant traction. After extraction, the specimen was photographed (Figure 3). The wound was dressed with bacitracin, Xeroform, and Tegaderm. The patient was prescribed a 7-day course of Augmentin given bony involvement.

Figure 3. Image of the TASER 7 barb (Axon Enterprise, Inc) alongside the Kocher clamps used for removal.
Informed consent for the use of photographs and clinical details for publication was obtained from the patient.
Discussion
Willoughby et al described a technique for removing TASER barbs from bone.3 In their procedure, a barb lodged in the clavicle was extracted using vise-grip pliers and a 10-mL syringe as a fulcrum. After administering IV ketorolac and local anesthesia (1% lidocaine and 0.5% bupivacaine), the pliers grasped the barb, and the syringe provided leverage for removal. The method was effective with minimal trauma, though a small barb fragment remained.3 This technique was suited to earlier TASER models like the X26 and X2, which had a more advantageous probe design for removal.
In contrast, the newer TASER 7 model presents unique challenges because of its flatter probe design, which reduces grip and complicates extraction, especially given its increased kinetic energy and faster dart velocity. The design of the TASER 7 probe necessitates different strategies for removal, as traditional methods used for earlier models may be less effective.
Other previous cases documented in the literature highlight more severe injuries. Delavar et al reported a case where part of the dart remained embedded in the frontal lobe, requiring surgical removal.4 Another case involved a dart penetrating the skull and injuring the meninges and brain tissue, necessitating neurosurgical consultation.5 Chandler et al described a situation where neurosurgery successfully removed the probe in the emergency department despite no intracranial abnormalities, underscoring the importance of imaging and specialized consultation.6
In our case, a CT scan confirmed that the barb was embedded in the supraorbital frontal bone but had narrowly missed the frontal sinus. Had the barb penetrated the frontal sinus, the extraction would have required additional precautions to avoid complications such as infection or cerebrospinal fluid (CSF) leakage, potentially necessitating surgical intervention.
Our case differs in that, because the critical structures were missed, the TASER barb was able to be successfully removed at bedside using Kocher clamps, avoiding the need for surgical intervention. This success was facilitated by the absence of intracranial injury and the specific positioning of the barb, which was confined to the supraorbital frontal bone and had narrowly missed critical structures such as the frontal sinus. The use of Kocher clamps allowed for controlled and effective extraction with firm, constant traction, overcoming the challenges posed by the barb's deeper penetration and the intricate anatomy of the facial region. This case underscores the importance of understanding the TASER 7's design features, particularly its flatter probe, and considering the patient’s anatomy to ensure safe and effective removal. The approach highlights how tailored extraction techniques and meticulous planning, including the use of local anesthesia and prophylactic antibiotics, can lead to successful outcomes even in complex cases.
Acknowledgments
Authors: Benjamin B. Scott, MD1; José Antonio Arellano, MD1; Hilary Y. Liu, BS1; Francesco M. Egro, MD, MSc, MRCS1,2
Affiliations: 1Department of Plastic Surgery, University of Pittsburgh Medical Center, Pittsburgh, Pennsylvania; 2Department of Surgery, University of Pittsburgh Medical Center, Pittsburgh, Pennsylvania
Correspondence: Francesco M. Egro, MD, MSc, MRCS, Department of Plastic Surgery, University of Pittsburgh Medical Center, 1350 Locust St, Suite G103, Pittsburgh, PA 15219, USA. Email: francescoegro@gmail.com
Ethics: Informed consent for the use of photographs and clinical details for publication was obtained from the patient.
Disclosures: The authors disclose no relevant financial or nonfinancial interests.
References
- Kroll MW. Physiology and pathology of TASER electronic control devices. J Forensic Leg Med. 2009;16(4):173-177. doi:10.1016/j.jflm.2008.12.012
- Bleetman A, Hepper AE, Sheridan RD. The use of TASER devices in UK policing: an update for clinicians following the recent introduction of the TASER 7. Emerg Med J. 2023;40(2):147-150. doi:10.1136/emermed-2022-212521
- Willoughby L, Peyton K, Gorgas D, Li-Sauerwine S. Leveraging resources to remove a taser barb embedded in bone: case report. Clin Pract Cases Emerg Med. 2022;6(1):29-31. doi:10.5811/cpcem.2021.10.54196
- Delavar B, Thompson MA. Penetrating intracranial taser injury. J Emerg Med. 2021;61(5):590-591. doi:10.1016/j.jemermed.2021.07.071
- Rehman TU, Yonas H, Marinaro J. Intracranial penetration of a TASER dart. Am J Emerg Med. 2007;25(6):733.e3-e4. doi:10.1016/j.ajem.2006.12.017
- Chandler J, Martin BP, Graham DD Jr. TASER(®) injury to the forehead. J Emerg Med. 2013;44(1):e67-e68. doi:10.1016/j.jemermed.2011.06.009