Pediatric Granular Cell Tumor of the Digital Nerve: A Case Report and Literature Review
© 2025 HMP Global. All Rights Reserved.
Any views and opinions expressed are those of the author(s) and/or participants and do not necessarily reflect the views, policy, or position of ePlasty or HMP Global, their employees, and affiliates.
Abstract
Introduction. Granular cell tumors (GCTs) are rare soft tissue neoplasms thought to originate from Schwann cells of the peripheral nervous system. These tumors predominantly occur in the head and neck regions. Instances of GCTs affecting peripheral nerves of the upper extremity, particularly in the hand, are exceptionally rare.
Methods. A 9-year-old girl presented with a rapidly growing mass on the left index finger. Ultrasound and magnetic resonance imaging revealed a mass encasing the neurovascular bundle extending to the dermal surface. Biopsy confirmed the presence of a GCT. Intraoperatively, the tumor, which was embedded within the radial nerve and adherent to the tendon sheath, was excised. Nerve reconstruction was performed with a posterior antebrachial cutaneous nerve graft.
Results. Histopathology showed pleomorphic polygonal cells with granular cytoplasm and mild nuclear atypia. Immunohistochemical staining was positive for S100, CD68, SOX10, NKI/C3, inhibin, and TFE3, confirming the diagnosis of a benign GCT. The tumor was successfully excised with clear margins.
Conclusions. Here we present the 5th documented case of GCT originating from the digital nerve and first-ever case treated with excision and posterior antebrachial cutaneous nerve graft reconstruction. The successful use of a nerve graft in this case underscores the value in preserving sensory function after tumor excision. Long-term follow-up is essential to monitor for recurrence and ensure favorable outcomes.
Introduction
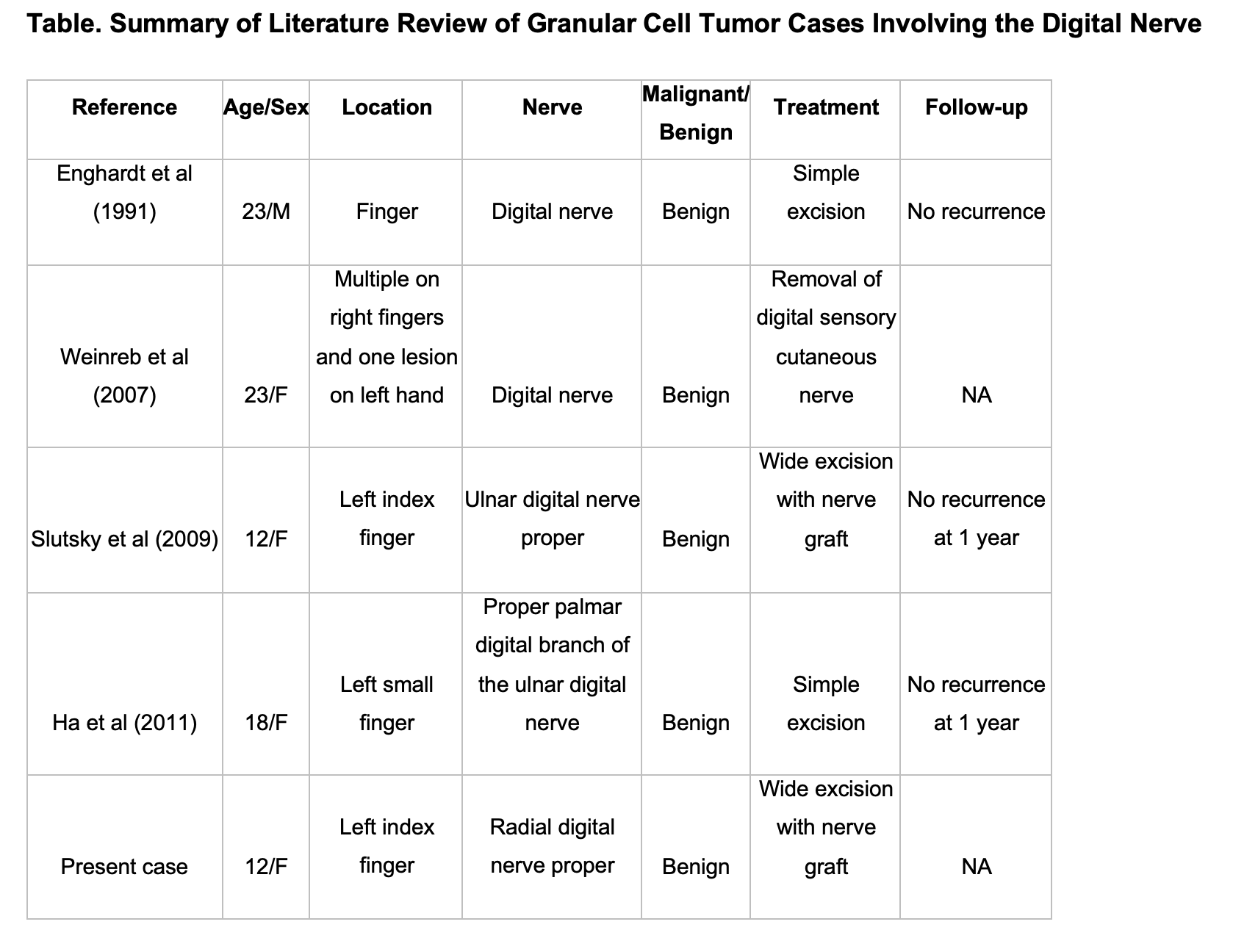
Granular cell tumors (GCTs) are rare soft tissue tumors that arise from myelin-producing Schwann cells in the peripheral nervous system. GCTs are uncommon and only comprise 0.5% of all soft tissue tumors.1 The majority of GCTs are benign, with approximately 2% identified as malignant.2 When these rare tumors do occur, they most often arise within the head and neck regions with preference to tongue and oral mucosa. In review of the literature, there are four reports of GCT involving the digital nerve (Table).3-6 Here we present a case of a GCT originating from an index digital nerve involving the digital artery and flexor tendon, treated with tumor excision and posterior antebrachial cutaneous nerve graft reconstruction.
Case Presentation
History and presentation
A 9-year-old right-hand-dominant girl presented with a 2-month history of a rapidly growing mass on the left index finger. Hand examination revealed an isolated tender nodule on the volar aspect of the left index finger tracking along the flexor tendon sheath towards the first webspace. Tenderness was exacerbated by palpation and percussion of the nodule. No notable alteration in flexion or extension function was appreciated on exam. Examination demonstrated the mass extended from the distal palm to the level of the distal proximal phalanx, with the mass felt to be fixed to the flexor tendon sheath.
Imaging
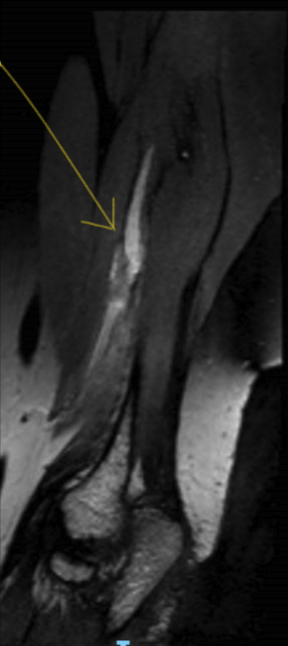
Ultrasound revealed a 0.7 × 1.8 × 3.8-cm hypoechoic mass with no vascularity detected on Doppler. Magnetic resonance imaging with and without contrast of the left hand revealed a 1 × 1.3 × 2-cm lesion located along the surface of the flexor tendon on the index finger. The lesion demonstrated high signal on T2-weighted images and isointense to muscle on T1-weighted images. The lesion encased the neurovascular bundle and extended to the dermal surface through the subcutaneous soft tissues. Borders were found to be well defined with no involvement of the bone or bone marrow. Differential diagnosis at this time included giant cell tumor, neurofibroma, schwannoma, and malignant peripheral nerve sheath tumor.
Surgery
Excisional biopsy of the mass was performed to provide samples to pathology for analysis. Intraoperatively, the subcutaneous fat along the radial aspect of the index finger was abnormal and adherent to the skin. The tumor did not have well-defined margins. The nerve demonstrated a swollen appearance, and the abnormal fat could not be cleared from the radial neurovascular bundle with blunt dissection. Biopsy of the abnormal fatty tumor surrounding the radial digital nerve was performed and sent for frozen section analysis and found to be a benign mass.
The patient returned 4 weeks after initial excisional biopsy. First, a nerve graft was harvested from the posterior antebrachial cutaneous sensory nerve (Figure 1 A-B). Incisions were placed along the scar on the index finger from the previous excision. The tumor was found to be embedded within the left index radial digital nerve and adherent to the flexor tendon sheath (Figures 2A-2C). Excision was performed along the affected nerve and flexor tendon sheath. The tumor encased the radial and digital artery, requiring sacrifice in order to excise the tumor. The excised tumor measured approximately 3.8 cm in length (Figure 2D). Intraoperative frozen sections were sent to pathology to confirm clear proximal and distal margins. Additional specimens were sent for permanent pathological analysis. A nerve graft was used to reconstruct the digital nerve to preserve sensation to the left index finger (Figure 1C). The remaining distal posterior antebrachial cutaneous nerve was transferred to the medial antebrachial cutaneous nerve in an end-to-side tension-free fashion. Final microscopic pathology examination confirmed infiltration of the granular cell tumor into the perineurium, accompanied by extensive epineural and endoneurial fibrosis in the nerve.
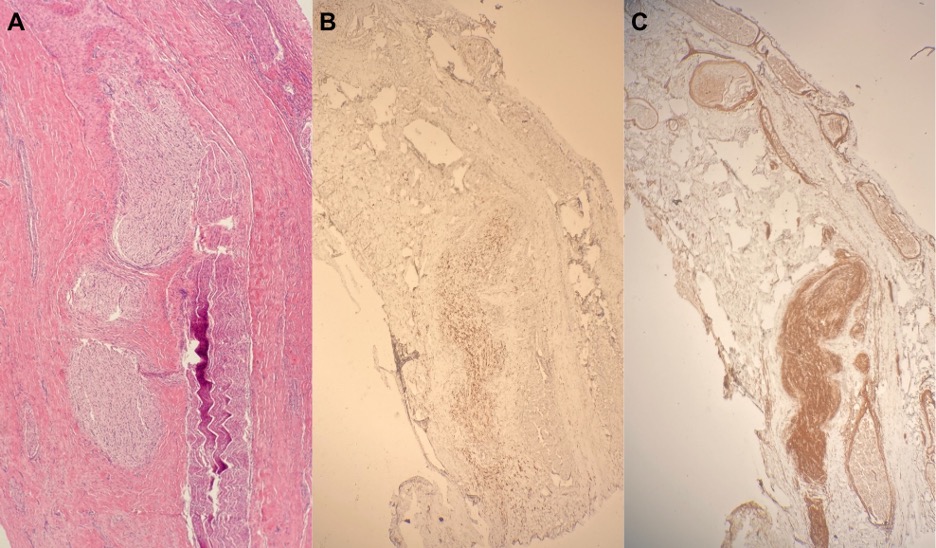
Figure 1. (A) A 10-cm left posterior antebrachial cutaneous nerve graft; (B) left posterior antebrachial cutaneous nerve graft and anatomy exposed; (C) left index finger post-excision and removal of involved structures.
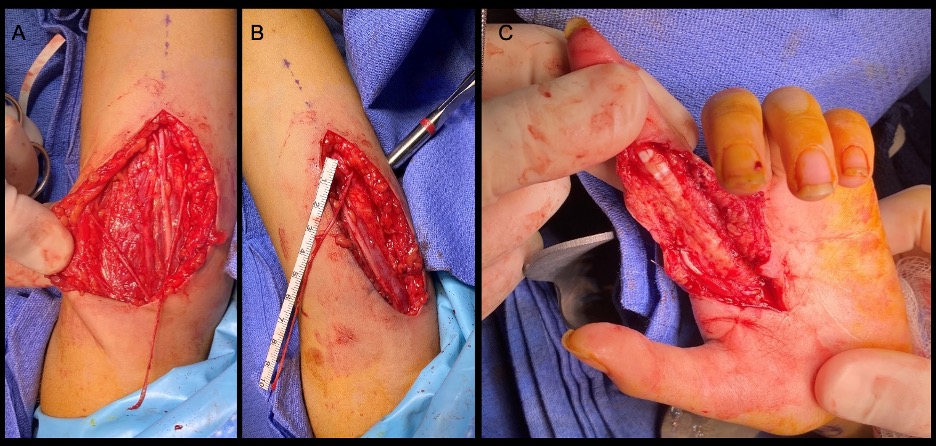
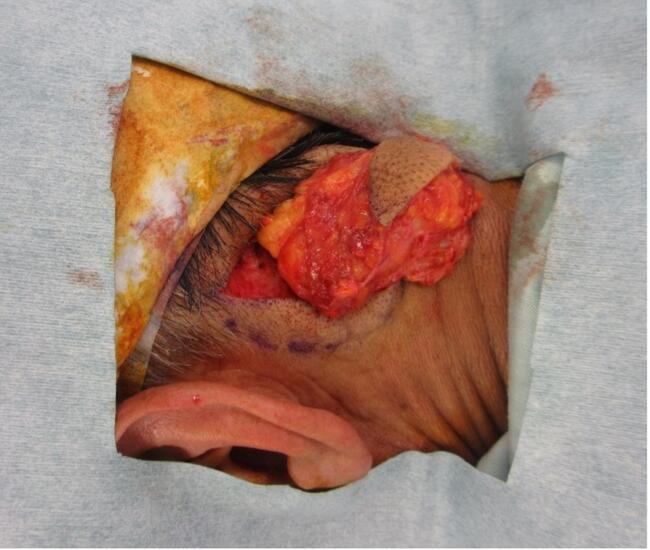
Figure 2. (A) Initial incision and exposure of tumor; (B) base of tumor indicated by yellow tie; (C) tumor grasped demonstrating involvement of surrounding structures; (D) excised tumor measuring approximately 3.8 cm in length.
Histopathologic findings
The tumor exhibited a soft-to-firm consistency and presented as pink-white-tan tissue. Further investigation revealed a proliferation of pleomorphic polygonal to slightly spindled cells with indistinct cell borders with mild to moderate nuclear atypia and granular cytoplasm (Figure 3). The cells infiltrated the soft tissue margins. Mitoses were inconspicuous. Immunohistochemical analysis demonstrated positive reactivity for S100, CD68, SOX10, NKI/C3, inhibin, and TFE3. Despite indications of potential infiltration in the biopsy, the proliferative index KI67 was less than 3%. Collectively, these findings were suggestive of a granular cell tumor.
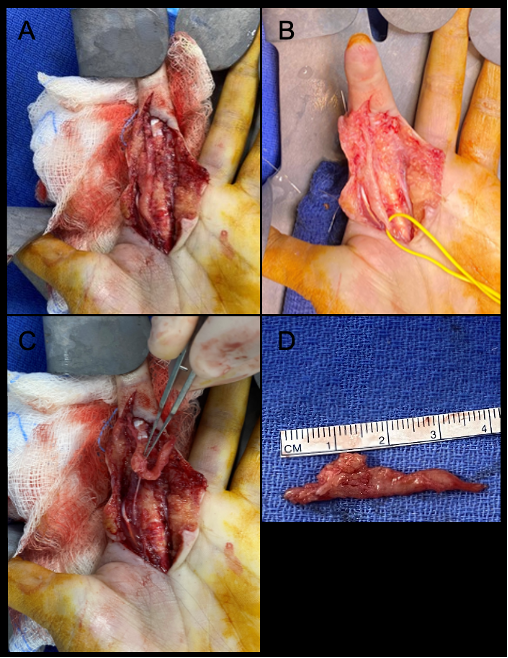
Figure 3. (A) H&E stain (40×) shows a mass arising from the peripheral nerve; (B) tumor cells (40×) diffusely positive for CD68; (C) collagen type IV stain (40×) displaying tumor perineural and intraneural growth.
Discussion
Granular cell tumors were first described by Abrikossoff in 1926. These tumors most often occur in women in their 4th to 6th decades of life; however, all age groups and sexes can be affected.1 These rare tumors are generally benign, and diagnosis is confirmed with imaging and biopsy. Histopathology with immunohistochemistry analysis, including S100 positivity, indicates the neural origin of the tumor. Distinction between benign, atypical, and malignant GCTs remains a controversial issue due to lack of histological and phenotypic criteria that predict behavior.7
Most GCTs are benign, and local invasion of structures is common.7 A previous study by Lack et al showed a recurrence rate of approximately 20% for GCTs that were incompletely excised.8 The potential for malignant transformation in GCTs remain a subject of debate, yet documented cases support its occurrence. One such case by Gallego et al describes a GCT of the hand diagnosed by biopsy with the refusal of excision by the patient.9 After 15 years, the patient returned due to symptomatic growth and was found to have a malignant transformation of the GCT. Within 8 months of malignant transformation, the patient expired with metastases to the lungs and axial skeleton. The risk for recurrence and the chance of malignancy support management by wide surgical excision, histopathology analysis, and long-term follow-up.
In our review of the literature available on PubMed and Web of Science, when searching for granular cell tumor and digital nerve we identified a total of 4 cases (Table). Our presented case and the Slutsky et al case share the most similarities of GCTs involving the digital nerves.3 Both cases involved young female patients with isolated nodules on the volar aspect of the digit. Slutsky et al detail a 12-year-old girl who presented with a long-standing nodule on the left index finger, while the current case involves a 9-year-old girl with a rapidly growing mass on the left index finger affecting the flexor tendon sheath. Notably, both cases opted for surgical approaches involving wide tumor excision and nerve reconstruction. Histopathology confirmed GCTs in both cases with positive S100 protein reactivity. Both cases demonstrated successful tumor removal.
Slutsky et al utilized a graft from the lateral antebrachial cutaneous nerve and the current case used a graft from the posterior antebrachial cutaneous nerve. The lateral antebrachial cutaneous nerve used by Slutsky et al typically arises from the lateral cord of the brachial plexus and supplies sensory innervation to the skin over the lateral forearm. The posterior antebrachial cutaneous sensory nerve, also known as the posterior cutaneous nerve, is a branch of the radial nerve and provides sensory innervation to the posterior aspect of the forearm. In the context of nerve grafting, either nerve may be chosen as donors and harvest for graft may depend on the surgeon's preference based on location, length, and diameter.
Management of GCTs involving the digital nerve require a comprehensive approach, including wide excision for tumor removal and nerve grafting for reconstruction. Given the tendency of recurrence in incompletely resected tumors and risk of malignant transformation, wide excision and long-term follow-up are both important factors in management. Furthermore, this case highlights the utilization of nerve grafts as a valuable strategy for preserving sensory function following GCT excision of the digital nerve.
Acknowledgments
Authors: Caleb H. Bercu, BA1; Raghavee Neupane, BS, MPH2; Ashley Ramirez, MD3; Carole Brathwaite, MD4; Aaron J. Berger, MD, PhD1
Affiliations: 1Division of Plastic Surgery, Department of Surgery, Nicklaus Children’s Hospital, Miami, Florida; 2Nova Southeastern University College of Osteopathic Medicine, Fort Lauderdale, Florida; 3 Herbert Wertheim College of Medicine, Florida International University, Miami, Florida; 4Department of Pathology, Nicklaus Children’s Hospital, Miami, Florida
Correspondence: Aaron J Berger, MD, PhD; aaron.berger@nicklaushealth.org
Ethics: Institutional review board approval was obtained for this study in accordance with a departmental umbrella protocol, with a waiver of informed consent per the institutional protocol. The author(s) state(s) that this research was conducted in accordance with the Helsinki Declaration as revised in 2008.
Statement of Funding: The author(s) received no financial support for the research, authorship, and/or publication of this article.
Disclosures: The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
References
1. Fisher ER, Wechsler H. Granular cell myoblastoma--a misnomer. Electron microscopic and histochemical evidence concerning its Schwann cell derivation and nature (granular cell schwannoma). Cancer. 1962;15:936-954. doi:10.1002/1097-0142(196209/10)15:5<936::aid-cncr2820150509>3.0.co;2-f
2. Fanburg-Smith JC, Meis-Kindblom JM, Fante R, Kindblom LG. Malignant granular cell tumor of soft tissue: diagnostic criteria and clinicopathologic correlation. Am J Surg Pathol. 1998;22(7):779-794. doi:10.1097/00000478-199807000-00001
3. Slutsky DJ. Granular cell nerve tumor in the hand: case report. J Hand Surg. 2009;34(8):1512-1514. doi:10.1016/j.jhsa.2009.05.011
4. Ha SY, Suh YL, Sung CO. Granular cell tumour arising in a digital nerve. J Hand Surg Eur Vol. 2011 Mar;36(3):249-250. doi:10.1177/1753193410392647
5. Enghardt M, Jordan S. Granular cell tumor of a digital nerve. Cancer. 1991;68(8):1764-1769. doi:10.1002/1097-0142(19911015)68:8<1764::AID-CNCR2820680820>3.0.CO;2-#
6. Weinreb I, Bray P, Ghazarian D. Plexiform intraneural granular cell tumour of a digital cutaneous sensory nerve. J Clin Pathol. 2007;60(6):725-726. doi:10.1136/jcp.2005.035972
7. Machado I, Cruz J, Lavernia J, Llombart-Bosch A. Solitary, multiple, benign, atypical, or malignant: the “Granular Cell Tumor” puzzle. Virchows Arch. 2016 May;468(5):527-538. doi:10.1007/s00428-015-1877-6
8. Lack EE, Worsham RGF, Callihan MD, et al. Granular cell tumor: A clinicopathologic study of 110 patients. J Surg Oncol. 1980;13(4):301-316. doi:10.1002/jso.2930130405
9. Dauder Gallego C, Ruiz Zafra J, Stanescu RI, et al. Granular cell tumor of the hand: unusual malignancy of a previous benign lesion: a case report. JBJS Case Connect. 2021 Aug 4;11(3). doi:10.2106/JBJS.CC.20.00503