From Tooth to Phalanx: The First Reported Case of Porphyromonas endodontalis Causing Osteomyelitis of the Proximal Phalanx
© 2025 HMP Global. All Rights Reserved.
Any views and opinions expressed are those of the author(s) and/or participants and do not necessarily reflect the views, policy, or position of ePlasty or HMP Global, their employees, and affiliates.
Abstract
Porphyromonas (P.) species, typically associated with oral infections, are known for their role in causing root canal infections and endodontic abscesses. Here, the authors present the first and only reported case of P. endodontalis osteomyelitis in a long bone following a phalanx injury and subsequent dental procedure. In this case, the infection presented in the right fifth proximal phalanx of a 16-year-old boy. Despite initial conservative management and multiple negative bacterial cultures, symptoms persisted, prompting surgical intervention with debridement, biopsy, culture, and polymerase chain reaction analysis. This case underscores the aggressive and elusive nature of P. endodontalis, highlighting challenges in diagnosis and the importance of considering the Porphyromonas species in cases of osteomyelitis, particularly in those with a dental history.
Introduction
Porphyromonas (P.) bacteria, characterized as obligate anaerobic, gram negative, non-sporulating pleomorphic rods, primarily comprise asaccharolytic black pigmenting species such as P. gingivalis, P. endodontalis, P. circumdentaria, and P. salivosa.1,2 These organisms are predominantly found in the oral cavity, particularly in individuals with poor dentition, where they are implicated in root canal infections and endodontic abscesses.3,4
In the literature, there are few cases in which Porphyromonas causes osteomyelitis outside the oral cavity, with even fewer being described in the upper extremity.5 In this case, we present a 16-year-old boy diagnosed with a P. endodontalis osteomyelitis affecting the right fifth proximal phalanx with infiltration of the metacarpal. Following a right fifth finger proximal phalanx fracture, the patient underwent an open reduction and internal fixation with subsequent biopsies and cultures. The tissue culture did not grow any microorganisms, prompting broad-range polymerase chain reaction (PCR) testing that detected 16S ribosomal ribonucleic acid bacterial genes, revealing P. endodontalis as the causative agent of the osteomyelitis infection. To our knowledge and extensive literature search, this is an extremely rare instance of P. endodontalis causing an osteomyelitis affecting the long bones.
Case Presentation
History and presentation
A 16-year-old right-handed boy with a history of KDM5C syndrome, Brown syndrome, and developmental delay presented to Nicklaus Children’s Hospital 2 weeks after a fall on his right hand. He had no history of fever, open wounds, or other signs of infection. Approximately 2 weeks following his injury, he presented to the emergency room with continued pain and was found to have sustained a right fifth proximal phalanx fracture. He was placed in a foam padded aluminum finger splint and prescribed cephalexin after he was found to have broken skin over the fracture site because of dermatillomania. The patient’s primary caretaker disclosed that he had recently undergone dental cleaning before the onset of his symptoms. Following consultation with the hand and peripheral nerve surgery team, the patient’s right fifth finger was immobilized in an ulnar gutter splint, and the patient was instructed to refrain from activities that could impact the affected area. However, despite conservative management, the patient’s finger pain intensified in the ensuing weeks, leading to the placement of a short arm cast. Four months later, the patient was still experiencing continued pain and an edematous right fifth finger, prompting further imaging.
Imaging
The initial X-ray performed 2 weeks after the injury showed ossifications at the medial base of the fifth proximal phalanx, found to be indeterminate of overlapping osseous structures or a minor fracture. Four months after the incident, a repeated X-ray demonstrated increased periosteal reaction and sclerosis along the proximal fifth phalanx with an abnormal appearance of the fifth metacarpal phalangeal joint with soft tissue edema. A chronic nonunion of a previously noted, minimally displaced ulna styloid process fracture was also seen, in addition to an obliquely healed distal right radius fracture (Figure A).
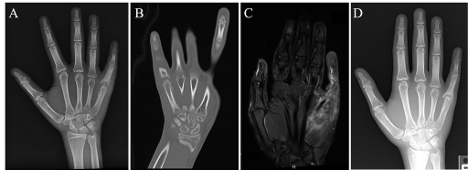
Figure. Imaging of the right hand: (A) preoperative X-ray at 2 months post-injury, (B) computed tomography at 3 months post-injury, (C) magnetic resonance imaging at 3 months post-injury, and (D) X-ray at 5 months postoperative.
Computed tomography of the right hand showed almost complete destruction of the base of the proximal fifth phalanx with mild sparing of the volar aspect with partial destruction of the head of the fifth metacarpal with a pencil-in-cup-like deformity (Figure B).
Magnetic resonance imaging (MRI) showed destruction of the base of the fifth proximal phalanx with bone marrow edema-like signal and hyperenhancement, suggesting osteomyelitis with infiltration of the inflammatory/infectious process of the fifth metacarpal with fifth metacarpal joint septic arthritis. The surrounding soft tissue and muscle edema also suggested cellulitis and myositis (Figure C).
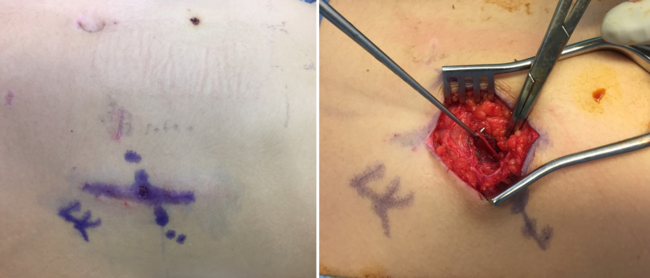
Surgery
Four months after initial presentation, the patient underwent an evaluation of the right hand under fluoroscopy and debridement of the right fifth metacarpal phalangeal joint with cultures and biopsy. The proximal capsule was seen to be replaced by thickened synovial tissue, accompanied by bone resorption. An elliptical incisional biopsy was performed through the dorsal capsule and sent for pathological examination. Hemorrhagic fluid was observed within the underlying joint space, along with apparent pannus or neoplastic changes. Additional tissue was sent for pathological analysis and cultures were obtained. Following copious irrigation of the wound, these abnormal findings suggested neither an obvious infection nor destructive changes. The decision was made to prioritize obtaining a diagnosis before proceeding with wound closure.
Histology
A “small right-finger tumor” was received by pathology; the tissue was light tan to pink in color and of a spongy-to-rubbery texture measuring 1.1 x 0.5 x 0.8 cm and weighing 1.1 g. Histologically, the mass showed mildly hyperplastic synovium with the focal villous configuration composed of acute and chronically inflamed vascularized tissue covered by synovial lining epithelium.
Microbiological testing
Bacterial cultures from the fifth proximal phalanx and metacarpal collected at the time of surgery showed negative growth of aerobic, anaerobic, and fungal colonies. However, bacterial detection by PCR (16 S gene Next Gen Sequencing) showed moderate abundance of P. endodontalis with minor abundance of Odoribacter splanchnicus, Pseudomonas aeruginosa, Alistipes onderdonkii, and Coprobacter species related to Coprobacter fastidiosus.
Outcome
After receiving the PCR results, the patient was prescribed a 30-day course of ciprofloxacin to address concern for Pseudomonas in addition to other concurrent infection etiologies. At the 5-month postoperative follow-up, the patient reported no pain and demonstrated appropriate healing; imaging showed progressive periosteal bone formation (Figure D). The pencil-in-cup deformity of the right fifth metacarpal-phalangeal joint was unchanged, the joint spaces were maintained, and the soft tissues were well preserved, indicative of healing. The patient was advised to continue physical therapy to work on passive and active range of motion (as tolerated) and to use a splint as needed for comfort. Considerations for future treatment include arthroplasty or fusion with or without joint denervation.
Discussion
This case of P. endodontalis osteomyelitis in the phalanges represents the first reported case of its kind, as P. endodontalis is an uncommon cause of osteomyelitis, especially in the long bones. It is, however, unsurprising that P. endodontalis is able to achieve such bone destruction as seen on the MRI of this patient because of the aggressive and resilient nature of the bacteria. This bacteria, unlike its Porphyromonas counterparts, is strictly anaerobic and does not need carbohydrates to survive.6 The Porphyromonas species utilize the lipopolysaccharide embedded in their cell membrane as a potent stimulator of inflammatory cytokines that participate in the formation of acute abscesses and, usually, alveolar bone destruction.6 Lipopolysaccharides also inhibit osteoblast differentiation and bone mineralization, further amplifying the destruction of bone.6,7 Its lipopolysaccharide induction of bone destruction allows for the perfect environment for the bacteria to settle, which ultimately causes a cascade effect of further bone damage. In the case of this patient with a KDM5C mutation, KDM5C is crucial for T-cell function, and mutations have been implicated in altering the immune response, thereby increasing the risk of infection.8
P. endodontalis also exhibits a remarkable capacity for tissue invasion beyond the oral cavity. Dorn et al demonstrated that P. endodontalis has the capability to invade the smooth muscle cells and endothelial cells of the coronary artery, underscoring its aggressive nature and potential for systemic dissemination.9 Given these findings, it is reasonable to speculate that hematogenous spread of the bacterium from the oral cavity to the fifth proximal phalanx likely contributed to the osteomyelitis in our patient. This hypothesis is supported by the patient’s recent dental cleaning that preceded the onset of his symptoms. A similar case was described in a 41-year-old man who developed P. gingivalis osteomyelitis in the ulna following a root-end resection of a molar and subsequent placement of a jacket crown.5 Of note, the P. gingivalis was also recovered by PCR only in this case. Likewise, a case of P. endodontalis osteomyelitis of the maxilla with orbital cellulitis was found in a 13-year-old boy after a tooth extraction.10 In this instance, the authors utilized metagenomics of an aspiration biopsy to identify the presence of the bacterium.
As demonstrated in these cases, P. endodontalis poses a challenge for conventional culture methods. In a study conducted by Gomes et al, the authors attempted to culture 50 samples of Porphyromonas bacteria. While 44 samples yielded Porphyromonas species, P. endodontalis proved elusive and could not be cultivated.3 Instead, PCR emerged as a more reliable method for its identification; even with PCR, however, the recovery rate remains relatively low, estimated at around 25%.3,6
Interestingly, during the surgical procedure, minimal inflammation or damage was visualized. Although P. endodontalis is typically associated with the signs and symptoms of rotting and necrotic teeth, studies have demonstrated its presence in asymptomatic individuals as well.11 Machado de Oliveira et al conducted a study revealing that while P. endodontalis was commonly detected in symptomatic cases of endodontic infections, it was also found in root canal infections without evident tenderness or radiating pain. This suggests that although P. endodontalis is known for its aggressive nature, it may occasionally elicit a relatively chronic or mild inflammatory response.
While unique, this case of P. endodontalis osteomyelitis is not surprising given the usual aggressive nature of the bacteria leading to bone damage and joint involvement, as seen in our patient. Because of the patient’s excoriation disorder, there is a possibility that the osteomyelitis may have been caused by direct inoculation rather than by hematogenous spread. However, considering the absence of overt infectious symptoms overlying the wound, multiple negative bacterial cultures, the temporal relationship with the patient’s recent dental cleaning, and P. endodontalis’ preference for anaerobic conditions, we believe direct inoculation is less likely. Instead, we favor hematogenous spread, which aligns with findings from the aforementioned cases.
Conclusions
This case highlights the challenges in diagnosing P. endodontalis infections, as traditional culture methods often fail to detect it, necessitating molecular techniques like PCR or metagenomics for accurate identification. While this case represents a rare manifestation of P. endodontalis infection, similar instances have been reported, suggesting the need for heightened awareness among clinicians, particularly in individuals with dental histories or predisposing conditions. Further research is warranted to better understand the epidemiology, pathogenesis, and optimal management strategies for Porphyromonas-associated osteomyelitis, ultimately improving diagnosis and outcomes for affected patients.
Acknowledgments
Authors: Hannah Korah, PhD1; Meagan Popp2; Caleb Bercu, MD3; Aaron Berger, MD, PhD3
Affiliations: 1University of Arizona College of Medicine, Tucson, Arizona; 2Herbert Wertheim College of Medicine, Florida International University, Miami, Florida; 3Division of Plastic Surgery, Department of Surgery, Nicklaus Children’s Hospital, Miami, Florida.
Correspondence: Caleb Bercu, MD, Division of Plastic Surgery, Nicklaus Children’s Hospital, 3100 SW 62 Avenue ACB #2230, Miami, FL 33155, USA. E-mail: caleb.bercu@nicklaushealth.org
Ethics: Institutional review board approval was obtained for this study per the institutional protocol and in accordance with a departmental umbrella protocol, with a waiver of informed consent per the institutional protocol. The authors state that this research was conducted in accordance with the Helsinki Declaration as revised in 2008.
Statement of Funding: The author(s) received no financial support for the research, authorship, and/or publication of this article
Disclosures: The authors declare no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
References
1. Paster BJ, Dewhirst FE, Olsen I, Fraser GJ. Phylogeny of Bacteroides, Prevotella, and Porphyromonas spp. and related bacteria. J Bacteriol. 1994;176(3):725-732. doi:10.1128/jb.176.3.725-732.1994
2. Mysak J, Podzimek S, Sommerova P, et al. Porphyromonas gingivalis: major periodontopathic pathogen overview. J Immunol Res. 2014;2014:476068. doi:10.1155/2014/476068
3. Gomes BP, Jacinto RC, Pinheiro ET, et al. Porphyromonas gingivalis, Porphyromonas endodontalis, Prevotella intermedia and Prevotella nigrescens in endodontic lesions detected by culture and by PCR. Oral Microbiol Immunol. 2005;20(4):211-215. doi:10.1111/j.1399-302X.2005.00214.x
4. Lombardo Bedran TB, Marcantonio RA, Spin Neto R, et al. Porphyromonas endodontalis in chronic periodontitis: a clinical and microbiological cross-sectional study. J Oral Microbiol. 2012;4. doi:10.3402/jom.v4i0.10123
5. Diaz ADB, Rodriguez LEQ, Garza NE, et al. Porphyromonas endodontalis, its virulence factor, nutrition, detection, epidemiology and treatment. Int J Appl Dent Sci. 2019;5(3):366-369.
6. Mirucki CS, Abedi M, Jiang J, et al. Biologic activity of porphyromonas endodontalis complex lipids. J Endod. 2014;40(9):1342-1348. doi:10.1016/j.joen.2014.02.017
7. Krawczyk C, Zhai L, Guak H, et al. The sexually dimorphic histone demethylase promotes optimal T cell responses during infection. J Immunol. 2022;208 (1_Supplement):55.22. doi:10.4049/jimmunol.208.Supp.55.22
8. Welkerling H, Geissdörfer W, Aigner T, Forst R. Osteomyelitis of the ulna caused by Porphyromonas gingivalis. J Clin Microbiol. 2006;44(10):3835-3837. doi:10.1128/JCM.00793-06
9. Yao Q, Hu X. Osteomyelitis of maxilla with orbital cellulitis after tooth extraction. Radiol Infect Dis. 2022;9(4):152-154. doi:10.4103/RID.RID_16_22
10. Machado de Oliveira JC, Siqueira JF Jr, Alves GB, Hirata R Jr, Andrade AF. Detection of Porphyromonas endodontalis in infected root canals by 16S rRNA gene-directed polymerase chain reaction. J Endod. 2000;26(12):729-732. doi:10.1097/00004770-200012000-00016