Case Series of Reconstruction Applying NovoSorb Biodegradable Temporising Matrix: Preliminary Practice and Findings in the United Kingdom
© 2025 HMP Global. All Rights Reserved.
Any views and opinions expressed are those of the author(s) and/or participants and do not necessarily reflect the views, policy, or position of ePlasty or HMP Global, their employees, and affiliates.
Abstract
Background: Biodegradable temporizing matrix (BTM) is a novel synthetic dermal matrix for wound reconstruction and an alternative to biological dermal substitutes such as Integra (Integra LifeSciences). It provides a scaffold for dermal regeneration and acts as a temporizing device prior to skin graft application, reducing the need for autologous tissue donor sites such as local or free-flap transfer.
Methods:This retrospective case series involved 12 patients whose surgery was completed with BTM from October 2021 to February 2023. The inpatient stay, subsequent procedures, and any complications were also reviewed.
Results:The median time for inpatient stay was 3.5 days, and patients who required skin grafts after full BTM integration were treated as a day case. Only 1 case had the complication of postoperative infection.
Conclusions:The study supports the application of BTM products to heal wounds with exposed bone or tendon. This is considered a low-risk option to reduce complications and improve reconstructive and cosmetic outcomes, particularly in the head and neck region.
Introduction
Biodegradable temporizing matrix (BTM, also known as BTM NovoSorb) is an artificial synthetic polymer that does not contain any biological materials.
Complex wounds are generally characterized by the exposure of tendon and bone, as well as the failure of reconstructive procedures such as skin grafts. Even patients with multiple comorbidities can undergo skin grafting for complex reconstructions, typically 4 weeks after applying BTM. This approach can lead to sensory function regeneration in the early stage, enhancing its effectiveness and robustness.
Free-tissue transfer is commonly regarded as the gold standard of reconstruction in complex wounds; however, patient comorbidities and other factors may be contraindications for free-tissue transfer surgery. With the application of BTM, the operating time is shortened, and morbidity is lowered compared with pedicled or free flaps, indicative of a reduction in surgical risk and complication.
Methods and Materials
A consecutive case series review of patients who were treated with BTM at the Plastic Surgery Department, Lister Hospital, East and North Hertfordshire NHS Trust, Stevenage, United Kingdom, was performed from October 2021 to February 2023. Patient demographics, comorbidities, defect etiology, size of the defect, the reason for BTM use, operation details, and complications (if any) were documented using information acquired from the medical records. The time spent in initial hospital stay, the time from BTM implantation to integration, and the time spent on hospital stay for post-graft were recorded. The indications for BTM were grouped as follows: (1) covering wounds with exposed bone, (2) covering wounds with exposed tendon, (3) covering surgical wounds, and (4) burn wound temporization. Complications were grouped into the following categories: infection and non-adherence.
Surgical technique
BTM was used as specified by the manufacturer
The first stage involved the inset of BTM to the wound bed and quilting sutures to ensure maximal contact surface area was achieved. Sutures used for inset were varying sizes of Ethilon (J&J MedTech), Prolene (J&J MedTech), and Vicryl Rapide (J&J MedTech). The secondary dressings most commonly used were Jelonet (Smith & Nephew) with a sponge tie-over or Mepitel (Mölnlycke), gauze, and a bandage. Likewise, choices were made according to clinician preference and anatomical location.
Where it could be facilitated, and with patient factors considered, dressings management took place on an outpatient basis. At dressings changes, the BTM was inspected, cleaned, and redressed by specialist nurses.
The second stage involved delamination of the sealing membrane and refreshing the surface of the neo-dermis. A split-thickness skin graft was then harvested and inset to the wound margins. Skin grafts were inset with Vicryl Rapide sutures or tissue glue. Skin grafts were assessed for take between 5 and 7 days postoperatively.
Complications management
Infection was defined as the BTM developing a yellow-grey color and purulent exudate accumulating in the matrix underneath the dressing membrane when patients were postoperatively followed up at the dressing clinic. The nursing team reviewed the wound site and examined the presence of purulent exudate when the dressing was changed. Once identified, the nursing team applied manual pressure to release the purulent fluid until drained and washed the wound site with aqueous chlorhexidine. The nursing team flagged any medical concern and the patient was reviewed by the surgical team.
Nonadherence of BTM was defined as any part of the BTM not attached to the wound surface 3 to 4 weeks post-application, when the patient was reviewed at the plastic dressing clinic.
Results
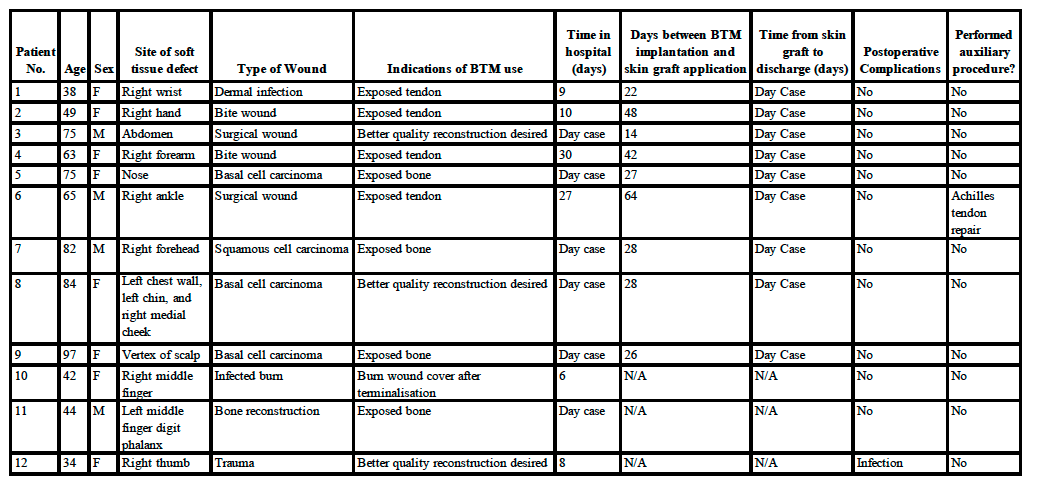
This case series included 12 patients with a median age of 63 years (range, 34-97 years); 75% (9 out of 12) were female. The decision for applying BTM was made by the responsible consultant, who took into consideration the patient’s demographics and defect factors, including covering exposed bone (5 cases), covering exposed tendon (5 cases), covering exposed surgical wound (1 case), and covering burn wound after terminalization (1 case). The sites of defects were the head (3 cases), hand (4 cases), wrist (1 case), abdomen (1 case), forearm (1 case), ankle (1 case), and chest (1 case).
The treated defects resulted from acute burn (1 case); infected animal bite wound (2 cases); dermal infection (1 case); complex surgical wound (2 cases); tumor excision, including basal cell carcinoma and squamous cell carcinoma (4 cases); bone reconstruction (1 case); and traumatic tissue loss (1 case).
Table. Case summary
Patient 5 presented to the Plastic Surgery Department with a confirmed diagnosis of basal cell carcinoma and received advice regarding the application of BTM and Mohs surgery. The indication for the application of BTM was to cover the exposed nasal bone and upper lateral cartilage. Clinical photography in Figure 1 was undertaken subsequent to Mohs surgery, prior to BTM application.

Figure 1. Photo of patient 5 taken post-Mohs excision of basal cell carcinoma and before the application of the biodegradable temporizing matrix (anterior view).
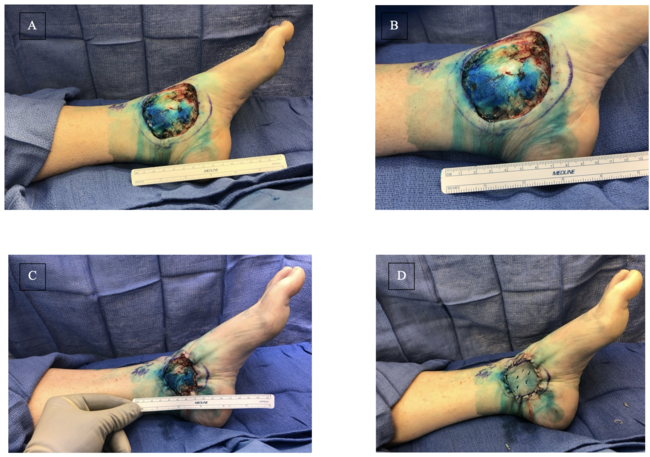
After 4 weeks, patient 5 returned to the theater to address a contour deficiency. No auxillary procedure was performed. Figure 2 depicts the clinical progress. Subsequently, 3 months post-application of the skin graft, the patient exhibited discernible enhancements in contour and aesthetic appearance, as shown in Figure 3. No postoperative complications were noted, and the patient was discharged from the hospital.

Figure 2. Patient 5 with basal cell carcinoma on the nose shown 4 weeks post-application of the biodegradable temporizing matrix to address the contour defect (left: anterior view; right: right lateral view).
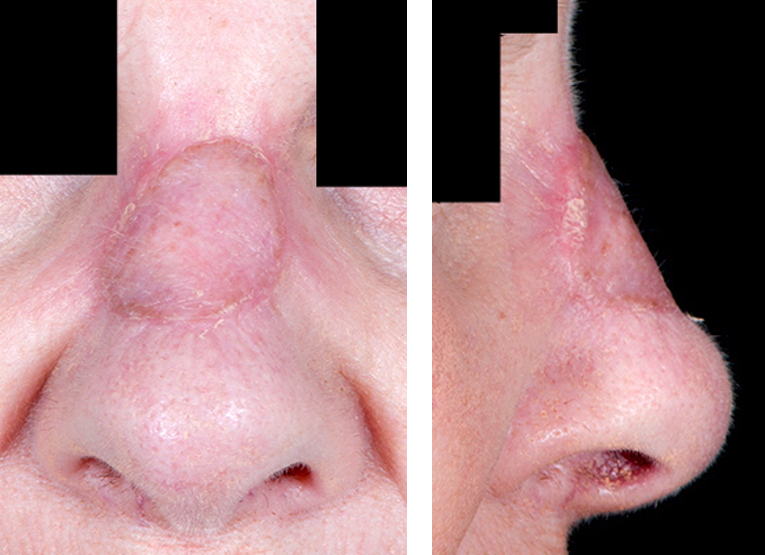
Figure 3. Patient 5 with basal cell carcinoma on the nose shown 3 months post-application of the skin graft (left: anterior view; right: right lateral view).
Patient 9 presented to the Plastic Surgery Department with a confirmed diagnosis of basal cell carcinoma and received advice regarding the utilization of BTM and burring of the outer table of the cranium. The purpose for the application of BTM was to cover the exposed outer table of the skull. The clinical photography in Figure 4 was undertaken subsequent to burring of the outer table of the cranium, prior to BTM application.

Figure 4. Patient 9, who underwent excision of basal cell carcinoma after burring of the outer table of the cranium, shown 4 weeks post-application of the biodegradable temporizing matrix at the vertex of the scalp.
Three months post–skin graft application, patient 9 revisited the clinic, displaying notable enhancements in contour and aesthetic appearance. No additional auxiliary procedures were undertaken. Figure 5 illustrates the clinical progress observed during the outpatient clinic follow-up. Notably, no postoperative complications were recorded, leading to the patient's discharge from the hospital.
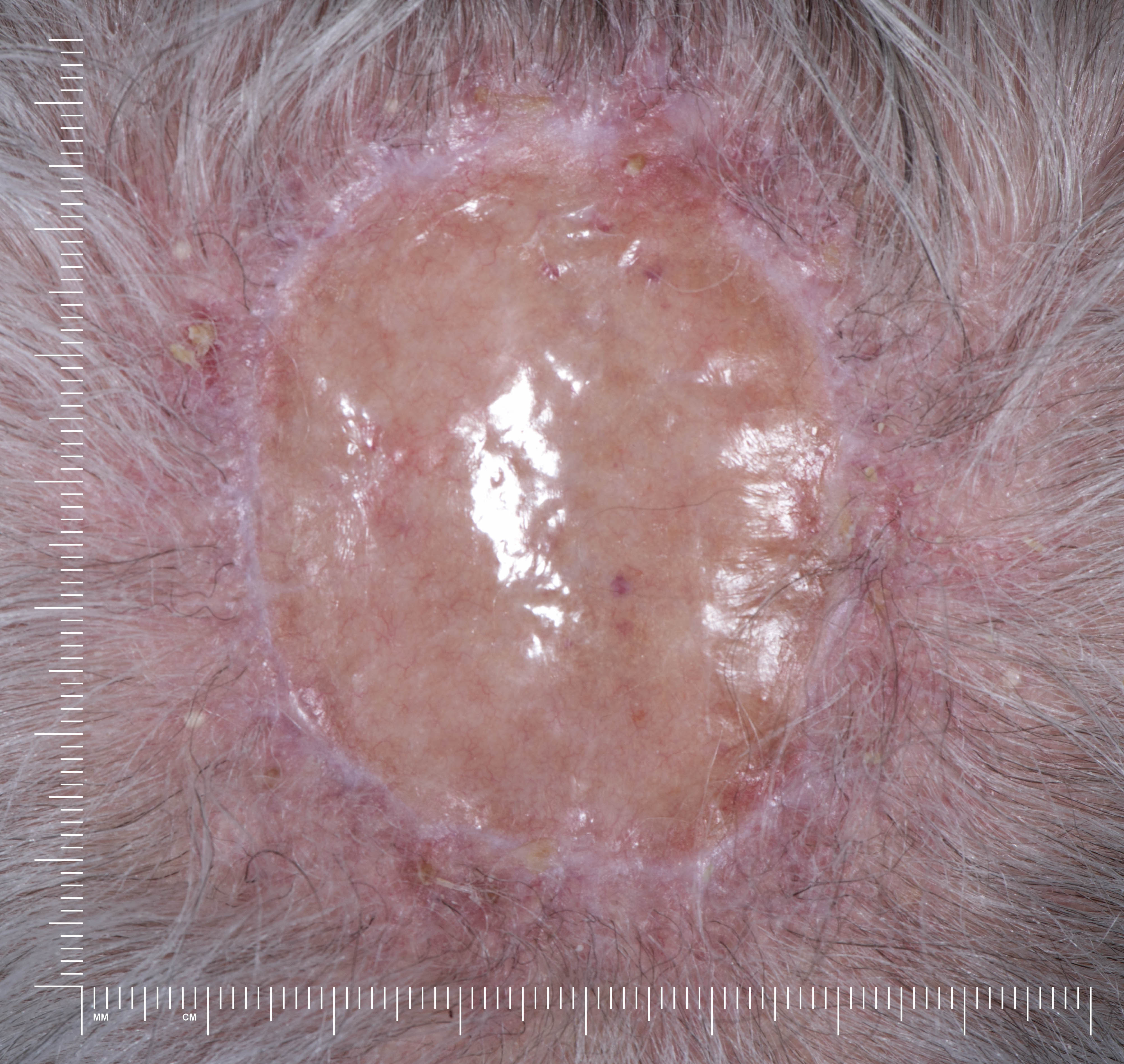
Figure 5. Patient 9, who underwent excision of a basal cell carcinoma after burring of the outer table of the cranium, shown 3 months post-application of the split-thickness skin graft on the biodegradable temporizing matrix at the vertex of scalp.
All cases would have otherwise required a more complex reconstructive procedure. The median time for inpatient stay was 3.5 days, where 6 cases were day cases, and the remaining 6 cases were admitted as inpatients. The shortest inpatient stay was 6 days, while the longest was 30 days with a complicated postoperative infection on the right forearm after significant soft tissue damage from a dog bite and open reduction internal fixation surgery.
Nine of 12 cases went on to receive application of a skin graft; the remaining 3 cases proceeded to heal by secondary intention. Of those 9 cases, the average time interval between BTM implantation and skin graft application was 33.2 days. For those patients who had a skin graft after the BTM integration, all patients underwent the procedure as a day case.
Postoperative complications of infection were encountered in 1 case, but there were no cases of non-adhesion concerns among the 12 patients. The infected case was superficial in nature and treated with a bedside washout. There was no delay in skin graft application and no long-term complications. Superficial infections were treated according to the trust’s antibiotics guidelines. Patient 12 did not receive a split-thickness skin graft and, as a result, the infection did not delay the definitive reconstruction procedure. As for other cases presented with complications, patient 6 had Achilles tendon repair surgery completed prior to BTM application; however, he had already developed signs of infections prior to BTM application. Thus, it was not considered as postoperative complication associated with BTM products, although it might have delayed the split-thickness skin graft application and the wound debridement; washout and split-thickness skin graft procedure were performed 64 days after the BTM implantation.
Discussion
This case series of 12 patients includes defects from head to ankle caused by burns, surgical wounds, dermal infections, or traumatic loss. The median time for inpatient stay was 3.5 days, and patients who required skin grafts after full BTM integration were treated as day cases. One case had the postoperative complication of infection.
BTM has been found to be straightforward to apply and does not contribute to an additional critical step in the surgery. The surgical team accumulated experience in treating various defects in different anatomical positions and concluded that the skin graft take was satisfactory on the newly formed dermis. Following the Mohs surgery for patient 5 and the removal of the outer table of the cranium through burring for patient 9, it displayed effectiveness in treating basal cell carcinoma in the facial and head regions, respectively. It also contributes to the consecutive case series published by Solanki et al in New Zealand,
The success of BTM integration with no signs of infection can be predicted by day 14. Infections are commonly characterized by microbial contamination and unfavorable wound healing,
Limitations
Nonetheless, the BTM is restricted to 2-dimensional cutting by surgeons and is unable to fully account for step defects, unlike 3-dimensional (3D) printing technology. Given that complex wounds can present in variable shapes, a 3-layer BTM can be introduced to improve contour and aesthetic outcome,
Conclusions
From a clinical perspective, the low infection rate, enhanced skin contouring, and favorable cosmetic results achieved at a reasonable cost with minimal hospitalization provide compelling reasons to contemplate universal adoption of BTM. This is especially pertinent in the facial and head and neck regions, where contouring and cosmetic outcomes are of paramount importance. Further case series reviews and randomized clinical trials should be carried out to investigate the association between BTM implantation and infection rate.
Acknowledgments
Authors: Simpson Shiu Chung Tam, BA (Hons) (Cantab)1; Kirsten Taylor, BSc (Hons), MBBS, MRCS2; Pankaj Patel, MBBS, MCh(Plast), FRCS(Plast)2; Patrick Goon, MBBCh, MD, FRCSEd(Plast), DipFESSH2; Manaf Khatib, MBBS, MSc, MRCS, FRCS(Plast), FEBOPRAS2
Affiliations: 1School of Clinical Medicine, University of Cambridge, Cambridge, United Kingdom; 2Department of Plastic Surgery, Lister Hospital, East and North Hertfordshire NHS Trust, Stevenage, United Kingdom
Correspondence: Simpson Shiu Chung Tam, School of Clinical Medicine, University of Cambridge, CB2 0SP, United Kingdom. E-mail: sct55@cam.ac.uk
Sources of support: The study has no external funding.
Disclosures: All authors declared that they have no relevant financial or nonfinancial interests to disclose.
References
- PolyNovo. A Biodegradable Temporizing Matrix designed to help surgeons treat traumatic wounds. 2021. Accessed May 15, 2025. https://polynovo.com/novosorb-btm-int-en/
- Greenwood JE. The evolution of acute burn care – retiring the split skin graft. The Annals of The Royal College of Surgeons of England. 2017;99(6):432-438. doi:10.1308/rcsann.2017.0110
- Kuang B, Pena G, Cowled P, et al. Use of Biodegradable Temporising Matrix (BTM) in the reconstruction of diabetic foot wounds: A pilot study. Scars Burn Heal. 2022;8:205951312211222. doi:10.1177/20595131221122272
- Med-Tech Innovation. PolyNovo to launch its NovoSorb BTM tech in European market at MEDICA. Rapid Medtech Communications Ltd. https://www.htworld.co.uk/news/polynovo-to-launch-pioneering-synthetic-wound-matrix-technology/#:~:text=A%20UK%20medical%20devices%20company,technology%20into%20the%20European%20market. October 20, 2021. Accessed May 15, 2025.
- Li H, Lim P, Stanley E, et al. Experience with <scp>NovoSorb</scp> ® Biodegradable Temporising Matrix in reconstruction of complex wounds. ANZ J Surg. 2021;91(9):1744-1750. doi:10.1111/ans.16936
- Wagstaff MJD, Salna IM, Caplash Y, Greenwood JE. Biodegradable Temporising Matrix (BTM) for the reconstruction of defects following serial debridement for necrotising fasciitis: A case series. Burns Open. 2019;3(1):12-30. doi:10.1016/j.burnso.2018.10.002
- Solanki NS, York B, Gao Y, Baker P, Wong She RB. A consecutive case series of defects reconstructed using NovoSorbⓇ Biodegradable Temporising Matrix: Initial experience and early results. Journal of Plastic, Reconstructive & Aesthetic Surgery. 2020;73(10):1845-1853. doi:10.1016/j.bjps.2020.05.067
- Holmes I, Albana MZ. Skin Tissue Engineering and Regenerative Medicine. (Holmes I, Albana MZ, eds.). Elsevier Science; 2016.
- Greenwood JE, Schmitt BJ, Wagstaff MJD. Experience with a synthetic bilayer Biodegradable Temporising Matrix in significant burn injury. Burns Open. 2018;2(1):17-34. doi:10.1016/j.burnso.2017.08.001
- Shah R, Kiely A, McKirdy S. Double-layer biodegradable temporising matrix reconstruction for abdominal skin and soft-tissue reconstruction. BMJ Case Rep. 2022;15(11):e251848. doi:10.1136/bcr-2022-251848
- Lo CH, Brown JN, Dantzer EJG, et al. Wound healing and dermal regeneration in severe burn patients treated with NovoSorb® Biodegradable Temporising Matrix: A prospective clinical study. Burns. 2022;48(3):529-538. doi:10.1016/j.burns.2021.07.014
- Hotchkiss RS, Moldawer LL, Opal SM, Reinhart K, Turnbull IR, Vincent JL. Sepsis and septic shock. Nat Rev Dis Primers. 2016;2(1):16045. doi:10.1038/nrdp.2016.45
- Cheshire PA, Herson MR, Cleland H, Akbarzadeh S. Artificial dermal templates: A comparative study of NovoSorbTM Biodegradable Temporising Matrix (BTM) and Integra ® Dermal Regeneration Template (DRT). Burns. 2016;42(5):1088-1096. doi:10.1016/j.burns.2016.01.028