Clinical Profile and Outcome of Acute Burn Care in a Tertiary Care Center of Western Nepal
© 2025 HMP Global. All Rights Reserved.
Any views and opinions expressed are those of the author(s) and/or participants and do not necessarily reflect the views, policy, or position of ePlasty or HMP Global, their employees, and affiliates.
Abstract
Background. Burns are a global public health problem that enormously impact Nepal’s health system. The treatment of burns is a challenging job for developing and underdeveloped countries. Major burn injuries are associated with high mortality in Nepal. However, extensive service is being provided, along with the gradual establishment of dedicated burn care units. This study aimed to determine the demographics of burn patients presented to the authors’ center and the outcomes of acute burn care.
Methods. This was a retrospective, descriptive, cross-sectional study of burn patients admitted from September 2022 to November 2023.
Results. The study included 101 patients ranging in age from 6 months to 77 years, with a median age of 27.8 years. The highest incidence of burns was among the male patients (56.4%), followed by the female patients (43.6%). Children under 15 years old comprised 45.5% of the admitted patients, and scald burns were the most common cause of burns in this group. The incidence of flame burns was highest among the working-class population and older adults. The total body surface area of the admitted patients ranged from 5% to 90%, with a mean of 15.22%. A total of 46.5% of the patients underwent operative management, of whom 36.2% required multiple surgeries. Hospital-stay duration ranged from 1 to 83 days, with a mean stay of 13.9 days. The study showed a 7.9% mortality rate.
Conclusions. The number of patients hospitalized due to burns is increasing, especially in the winter season. It mostly affects younger age groups, with the most common cause being scald burn. The mortality rate is found to increase as the extent of burn increases.
Introduction
Burns are a global public health problem and countries in Southeast Asia, including Nepal, share a large burden of burn injuries among them.1 The World Health Organization estimates that about 180 000 deaths occur due to burn injuries every year throughout the world. Burns are the third most common cause of injury in Nepal overall, after fall injuries and road traffic accidents, which has led to disability-adjusted life-years (DALYs).1-3 Burns may result in long-term socioeconomic complications as well as physical complications such as scarring, contracture, and limb amputation.4-6
The treatment of burns varies greatly depending on the depth and extent. Deep and extensive burns may require surgeries, skin grafts, and flaps, which are very challenging in Nepal because of the lack of skilled manpower, resources, and timely intervention. However, with the gradual establishment of dedicated burn care units and extensive services, comprehensive burn care is being extended gradually throughout the tertiary Centre of Nepal. Our institution Pokhara Academy of Health Sciences is one of them.
Very little study has been done about the epidemiology and management of burns in Nepal. Thus, this study aimed to provide baseline data on the clinical profile and outcome of burns at our institution.
Methods and Materials
We conducted a retrospective, descriptive, cross-sectional study from September 2022 to November 2023 of patients with burn injuries at the Pokhara Academy of Health Sciences. Before the study, ethical approval was granted from the institutional review committee of the Pokhara Academy of Health Sciences. Entries of the clinical records of patients who had undergone treatment in the plastic surgery unit of the Department of Surgery at the Pokhara Academy of Health Sciences were reviewed. All patients who presented with burn injuries requiring admission to the burn unit were included in the study. Patients who refused treatment were excluded from the study. Information retrieved for the study included the patients’ demographics, extent of burns (calculated by the Wallace Rule of Nines), depth of burns, cause of burns, duration of hospital stays, number and nature of operative interventions performed, and outcomes, all of which were presented as percentages. Patients were placed in 3 groups by age. Group 1 was patients under 15 years old (pediatric), group 2 was patients 16 to 60 years old, and group 3 was patients older than 60 years. All the data were tabulated in an Excel sheet and analyzed using Microsoft Office Excel version 2402.
Results
Our study included a total of 101 patients who were admitted to the Burn Plastic Surgery unit; the patients ranged from 6 months to 77 years old, with a mean age of 27.8 years and a median of 22 years. Of the patients, 56.4% were male and 43.6% were female, with a male-to-female ratio of 1.30. The incidence of burns was highest amongst the pediatric population, 45.5%, while 19.8% of the admitted patients were older than 60 years. In the 0 to 15-year age group, 60.9% were male and 39.1% were female, with a male-to-female ratio of 1.5. In the 16 to 60-year age group, 62.9% of the admitted patients were male and 37.1% were female, with a male-to-female ratio of 1.7. Conversely, in the 60-year-plus age group, 65% of the patients were female and 35% were male, with a female-to-male ratio of 1.85 (Table 1). Of the patients, 47.5% were from Pokhara, the city where our institution is located, and 52.5% were from outside Pokhara Valley.
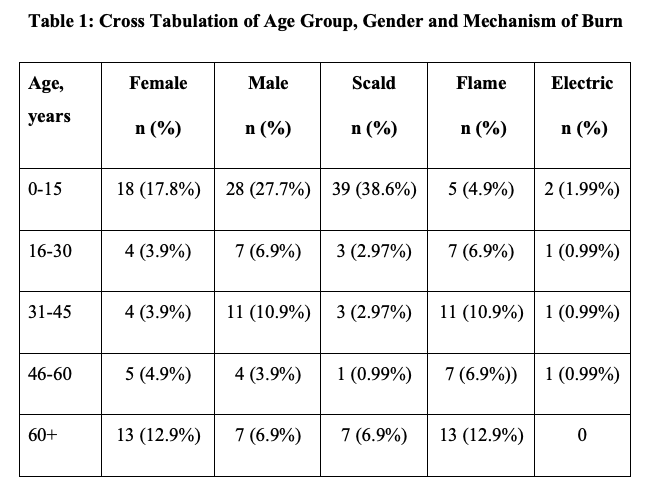
Our study showed that scald burn was the most common type of burn, followed by flame burn and electric burn, as shown in Figure 1. Scald burns were most common the pediatric population, followed by flame burns and electric burns (84.8%, 10.9%, and 4.3%, respectively). In the 60-year-plus age group, flame burns were the most common, followed by scald burns (65% and 35%, respectively) and none of the patients in this age group experienced an electric burn. In the 16 to 60-year age group, flame burns were also the most common, followed by scald burns and electric burns (70%, 31.4%, and 8.6%, respectively). Compared with males, females more frequently experienced flame burns, whereas electric burns occurred exclusively in the male population, as summarized in Table 1. The incidence of burns was most common in the winter season, with a maximum incidence of 40.5%, followed by spring with 23.8%, then autumn with 21.8%, and summer with 13.9%.
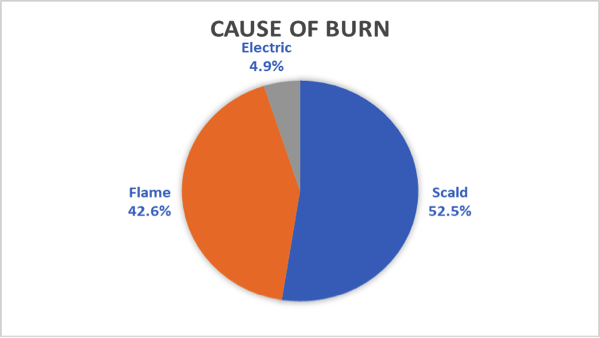
Figure 1. Mechanisms of burns.
The total body surface area (TBSA) involved ranged from 5.0% to 90.0%, with a mean TBSA of 15.2%. The majority (84.2%) of patients had second-degree burns, 13.9%, had third-degree burns, and only 1.9% had fourth-degree burns. The duration of hospital stay ranged from 1 to 83 days, with a mean stay of 13.9 days.
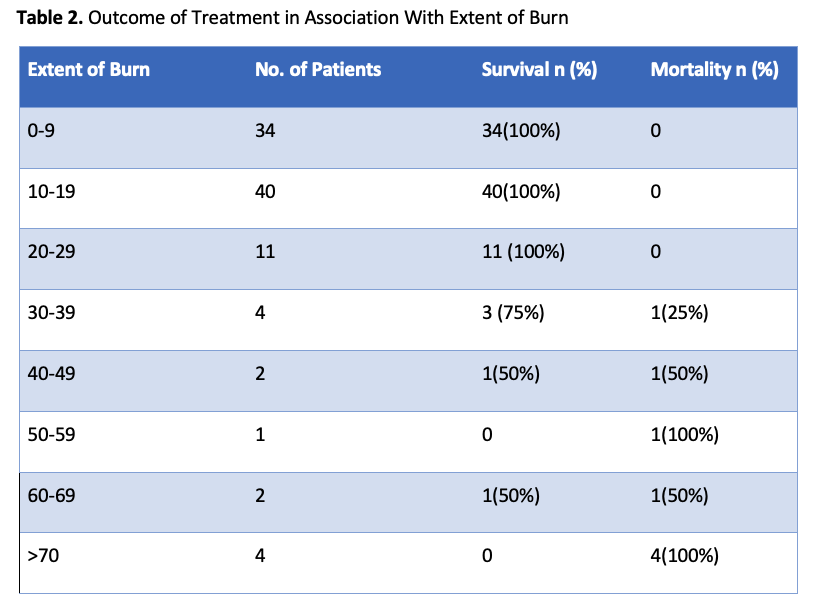
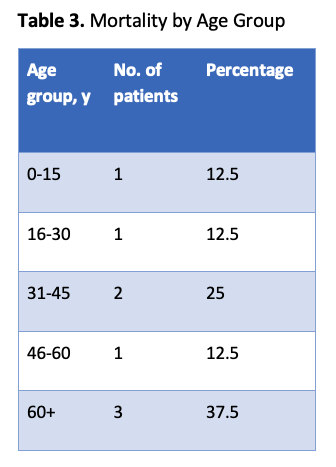
Of the total admitted patients, 46.5% underwent operative management, while 53.5% were managed nonoperatively. Of the patients undergoing surgical management, 63.8% underwent a single-sitting surgical approach, while 36.2% underwent multiple sittings—up to 4 surgeries—with a mean of 1.47 surgeries. Our study showed a 7.9% (n = 8) mortality rate of the total admitted cases of acute burn (Table 2). No patient with a TBSA of less than 29% died. Of the patients with a 30.0% to 59.0% TBSA, 42.8% died, and 83.3% of the patients with a TBSA greater than 60% died. One patient with a second-degree burn and a TBSA greater than 60.0% survived, as shown in Table 2. The 60-year-plus age group had the highest number of mortalities, as shown in Table 3.
Discussion
Burns are considered one of the major preventable and treatable public health problems, though they are still burdensome in many developing and underdeveloped countries. Southeast-Asian countries are under the biggest threat from the issue, and Nepal shares a large burden of it.1 Experts believe that burns are a major threat in developing and underdeveloped countries because of low literacy rates, lack of awareness, unavailability of a proper plan of action to control risk, and failure in the tabulation of the national registry.7
The incidence of burns in males is 57 per 1000 in high-income countries compared with 249 in 1000 in low-income countries; in females, the incidence is 106 per 1000 in high-income countries compared with 291 per 1000 in low-income countries.8 The 2016 to 2017 annual report from the Nepalese Department of Health and Population reports that 58.8% of burn injuries occur in people under 19 years old.9,10 However, for that age group, our study shows a much higher incidence (73.3%) than the annual health report. According to Gupta et al, 60.4% of total burns were due to scald burns, which is comparable to our study, as the majority of our cases (51.5%) were also due to scald burns.3
According to Smolle et al, since 2011 there has been an increase in burn admissions in Australia, Bulgaria, China, the Czech Republic, Finland, Iran, Israel, the Netherlands, Oman, and the United Kingdom; at the same time, there has been a decrease in burn incidence in Austria, Canada, Chile, China, Germany, Hong Kong, India, Japan, Mexico, and the United States.8 With proper prevention programs, workplace safety, and other legislative changes, the incidence of burns has decreased significantly in Australia.11 Similarly, the incidence of burns has been decreasing in India as the results of an elaborate burn prevention program.12
In our study, burn injuries were found to be more common among the pediatric population (age 0 to 15 years), which is comparable to studies done by Liu et al, Tripathee et al, and Sudhin et al.1,6,13 However, Gupta et al found the working-class population to be more susceptible to burn injuries than the pediatric population in Nepal.3
Our study shows an overall male predominance in burn admissions, with 56.4% male patients and 43.6% female patients. A similar pattern of burn injuries was seen in the study by Sudhin B et al; however, female predominance was seen in the study by Tripathee et al.1,6 When classified according to age groups, male predominance is observed in the 0 to 15-year age group, which is comparable to Thapa et al.5 There is a male predominance in the working-class population as well, which is comparable to a study by Smolle et al.8 Conversely, female predominance was observed in the 60-year-plus age group, which is supported by the study by Sudhin et al.6 However, Åkerlund et al showed that children of both genders are equally susceptible to burn injuries, and males in the working-class age group are more prone to burn injuries. In addition, as age increases, gender differences are narrow.14
Regarding the mechanism of burn injuries, the most common type of burn in the pediatric population was scald burn (83.3%), followed by flame burn (12.5%), which is supported by studies by Thapa et al, Liu et al, and Sudhin et al.5,6,13 The culture of firewood cooking, the obligation of sharing the same room for cooking and other daily activities, and children practicing household work may increase the risk for children to encounter scald, contact, and flame burns. In the 60-year-plus age group, 65% were found to have experienced flame burns, followed by 35% having experienced scald burns. Similar trends were depicted in the study by Sudhin et al.6 Older adults gather around the fire to keep themselves warm, especially during winter, which may increase the incidence of flame burn in this age group. Flame burn was also the most common cause of burn in the working-class population, which is supported by Karki et al.15 Our study showed that the female population was more susceptible to flame burns, while the male population more often experienced scald burns; this result is comparable to that of Liu et al. Also, electric burns occurred mostly in males, which is also supported by studies by Sharma et al and Liu et al.13,16
The TBSA of the admitted patients ranged from 5% to 90%, with a mean of 15.22%, which is comparable to those seen by Sudhin et al and Karki et al.6,15 The majority of patients had second-degree burns (84.2%), followed by third-degree burns (13.2%), and fourth-degree burns (1.9%), which is similar to a Cameroonian study by Forbinake et al.17 Depending on burn severity, requirements, and complications, the operator may choose a surgical or nonsurgical technique of management. Any deep partial- and full-thickness burns, except those that are less than 4 cm2, require surgery, and any burn of indeterminate depth should be assessed after 48 hours.18 We managed 46.5% of patients surgically and the remaining 53.5% of patients nonsurgically. Also, those patients with large-size partial- and full-thickness burns had to undergo multiple surgeries. The surgeries performed included debridement of the burn site, partial- and full-thickness skin grafts, and flap coverage, whereas nonsurgical treatment included the use of antimicrobial creams, occlusive dressings, and collagen dressings every alternate day or as required.
The duration of hospital stay ranged from 1 to 83 days, with a mean stay of 13.9 days and a median of 8.5 days; this is comparatively less than reported by the studies of Rai et al and Karki et al, which showed the range of hospital stay to be 1 to 105 days with a median of 17 and 13.3 days, respectively.15,19 However, a systemic review of the epidemiology of burn injuries in Nepal showed that the average length of hospital stay of burn victims ranges from 13 to 60 days.1
The incidence of burns is highest in the winter season and least common in the summer. Similar seasonal variations were noted in the study of Liu et al.13 A mortality rate of 7.9% was seen in our 15-month-long study, which is lower than other studies published in Nepal.1,6,15,19 The mortality rate was highest in the 60-year-plus age group (37.5%). There was an increase in mortality rate as the extent of burn increased, and the rate of third-degree burn was higher, which is similar to the findings in the study by Sakya et al.20 Rai et al also reported an increase in the mortality rate correlating with the increase in the TBSA of the burn victims, which is comparable to our study.19
Through this study, we are now able to identify the major risk factors, mechanisms, and other associated problems related to burns. This clinical profile could be used as a reference database for future studies and problems to be addressed, which may help reduce the burden of burns and the associated problems. A few ways to minimize the burden of burns could be raising awareness about the risk factors, education about the first-aid treatment, and immediate presentation to the health care center. Also, this study could be used as a sample tool for the government and other authorities to work further in extending dedicated burn-care centers to other rural areas across the country.
Limitations
The main limitation of our study is that it is a single-center study with a small number of treated patients, and there were missing data in the record files during the study period.
Conclusions
Burns have been one of the major causes of public health problems, mostly affecting young age groups and most commonly in the form of a scald burn. The mortality rate is found to increase as the extent of burn increases. To minimize the incidence and improve the consequences of acute burns, it is essential to spread proper awareness regarding the main causes of burns, focus on the people with the greatest risk factors (ie, older adults and young children), and educate these populations on how to stay aware and away from the source of the burn. Early medical attention, proper first-aid treatment, sterile techniques, and timely referral will improve treatment outcomes.
Acknowledgments
Authors: Piyush Giri, FCPS; Sushma Kunwar, MBBS; Karuna Khadka, MBBS; Pratishtha Pandey, MBBS; Shrinkhala Pokhrel, MBBS; Devendra Shrestha, MS; David Shrestha, MS; Narendra Vikram Gurung, MS
Affiliation: Department of Surgery, Pokhara Academy of Health Sciences, Pokhara, Nepal.
Correspondence: Piyush Giri, FCPS; dr.piyushgiri@gmail.com
Ethics: Institutional Review Committee (IRC) ref no: 212/080. Decision of providing ethical clearance decided by IRC –PoAHS meeting on February 20, 2024.
Disclosures: The authors disclose no relevant financial or nonfinancial interests.
References
1. Tripathee S, Basnet SJ. Epidemiology of burn injuries in Nepal: a systemic review. Burns Trauma. 2017;5:10. doi:10.1186/s41038-017-0075-y
2. Burns. World Health Organization. October 13, 2023 [Accessed 10 May 2024]. https://www.who.int/news-room/fact-sheets/detail/burns
3. Gupta S, Wong EG, Nepal S, et al. Injury prevalence and causality in developing nations: results from a countrywide population-based survey in Nepal. Surgery. 2015;157(5):843-849. doi:10.1016/j.surg.2014.12.020
4. Roy A, Mallick B, Ghosh R, Mallik S. A clinico-epidemiological study among burn injury patients in a tertiary care hospital of eastern India. J Med Sci Heal. 2022;8(2):139-144. doi:10.46347/jmsh.v8i2.21.206
5. Thapa B, Chapagain RH, Kayastha A. Epidemiology, clinical pattern and management outcome of paediatric burn injuries in Nepal. J Nepal Paediatr Soc. 2021;41(3):387-394. doi:10.3126/jnps.v41i3.30828
6. Sudhin BNA, Adhikari S, Khatiwada S. Epidemiology and outcome of acute burn patients at a new dedicated burn centre in Nepal. J Soc Surg Nepal. 2020;23(1):19-29. doi:10.3126/jssn.v23i1.33522
7. Forjuoh SN. Burns in low- and middle-income countries: a review of available literature on descriptive epidemiology, risk factors, treatment, and prevention. Burns. 2006;32(5):529-537. doi:10.1016/j.burns.2006.04.002
8. Smolle C, Cambiaso-Daniel J, Forbes AA, et al. Recent trends in burn epidemiology worldwide: a systematic review. Burns. 2017;43(2):249-257. doi:10.1016/j.burns.2016.08.013
9. Department of Health Services. Annual Report 2078/79. Government of Nepal, Ministry of Health and Population; 2023 [Accessed 10 May 2024]. http://dohs.gov.np/wp-content/uploads/Annual_Report.pdf
10. Phuyal K, Ogada EA, Bendell R, Price PE, Potokar T. Burns in Nepal: a participatory, community survey of burn cases and knowledge, attitudes and practices to burn care and prevention in three rural municipalities. BMJ Open. 2020;10(2):e033071. doi:10.1136/bmjopen-2019-033071
11. Duke J, Wood F, Semmens J, Edgar DW, Spilsbury K, Rea S. An assessment of burn injury hospitalisations of adolescents and young adults in western Australia, 1983-2008. Burns. 2012;38(1):128-135. doi:10.1016/j.burns.2011.02.008
12. Sarma BP. Prevention of burns: 13 years’ experience in northeastern India. Burns. 2011;37(2):265-272. doi:10.1016/j.burns.2010.08.003
13. Liu EH, Khatri B, Shakya YM, Richard BM. A 3 year prospective audit of burns patients treated at the Western Regional Hospital of Nepal. Burns. 1998;24(2):129-133. doi:10.1016/s0305-4179(97)00103-4
14. Åkerlund E, Huss FRM, Sjöberg F. Burns in Sweden: an analysis of 24,538 cases during the period 1987-2004. Burns. 2007;33(1):31-36. doi:10.1016/j.burns.2006.10.002
15. Karki B, Rai SM, Nakarmi KK, et al. Clinical epidemiology of acute burn injuries at Nepal Cleft and Burn Centre, Kathmandu, Nepal. Ann Plast Surg. 2018;80(3 Suppl 2):S95-S97. doi: 10.1097/SAP.0000000000001270
16. Sharma NP, Duke JM, Lama BB, et al. Descriptive epidemiology of unintentional burn injuries admitted to a tertiary-level government hospital in nepal: gender-specific patterns. Asia Pac J Public Health. 2015;27(5):551-560. doi:10.1177/1010539515585386
17. Forbinake NA, Dongmo G, Ohandza CS, Chichom-Mefire A, Fokam P, Beyiha G. Epidemiologic and clinical profile of burns in a tertiary hospital in sub-Saharan Africa. Burns Open. 2020;4(1):22-27. doi:10.1016/j.burnso.2019.10.001
18. Papini R. Management of burn injuries of various depths. BMJ. 2004;329(7458):158-160. doi:10.1136/bmj.329.7458.158
19. Rai SM, Karki B, Nakarmi K, et al. Retrospective study on early outcome of acute burn injuries treated at Nepal Cleft and Burn Centre of Public Health Concern Trust-Nepal. J Nepal Health Res Counc. 2014;12(28):195-199.
20. Sakya J, Sah SK, Bhandari KB, et al. Perception of community and hospital personnel on burn treatment and outcome in Nepal. JNMA J Nepal Med Assoc. 2018;56(214):924-930. doi:10.31729/jnma.3889