Use of Continuous Topical Oxygen Therapy to Treat Lower-Extremity Surgical Wound Dehiscence: A Retrospective Review
© 2025 HMP Global. All Rights Reserved.
Any views and opinions expressed are those of the author(s) and/or participants and do not necessarily reflect the views, policy, or position of ePlasty or HMP Global, their employees, and affiliates.
Abstract
Background. There is not a singular “gold standard” therapy for managing surgical wound dehiscence (SWD); rather, the goal is expediting wound closure. This study examines the feasibility of using a continuous topical oxygen (cTOT) device as part of a treatment algorithm to treat SWD of the lower extremity.
Methods. A single-center, retrospective analysis of lower-extremity SWD treated with cTOT was conducted via a retrospective chart review. Data were collected for a period of 8 months from January to August 2024. All SWD received the standard of care in addition to cTOT. Patients were seen weekly for evaluation until complete wound closure.
Results. Nine patients were included in this case review. The mean patient age was 52.6 years. SWD occurred after a variety of interventions. All patients’ SWD grade was either 3 or 4 according to the World Union of Wound Healing Society Sandy Grading System. The average time from starting TOT to the SWD healing was 52.6 days. In addition, the average estimated SWD surface area based on the wound measurement at the start of delivering TOT was 19.5 cm2. The average time to wound healing for all patients was 70 days. After excluding 1 outlier, the average time to wound healing was 59.5 days.
Conclusions. The positive outcomes exhibited in this case series suggest that cTOT is an effective treatment in the management of SWD in patients, regardless of specific surgical intervention. Furthermore, all the SWDs treated with cTOT progressed to wound closure without further need for surgery, hospitalization, or other costly procedures.
Introduction
The term surgical wound dehiscence (SWD) has been defined as “separation of the margins of a closed surgical incision that has been made in skin, with or without exposure or protrusion of underlying tissue, organs, or implants.”1 Separation may occur at single or multiple regions or involve the full length of the incision and may affect some or all tissue layers. Thus, this term can pertain to any measure of detachment seen in the tissue edges of a primarily closed surgical incision. A dehisced incision may or may not display clinical signs and symptoms of infection.
SWD is most likely to occur within 5 to 8 days postoperative.2 After surgical intervention, skin strength gradually increases as the tissue repair process occurs. It has been estimated that, at 1-week postoperative, skin has only healed to the point of achieving 3% of its pre-incision breaking strength.3 Additionally, pre-incision breaking strength is noted to be 30% and 80% at weeks 3 and 12 postoperative, respectively.3 Therefore, monitoring the surgical site is most crucial in the first few weeks of the postoperative period for prevention and detection of SWD. Moreover, even after a wound is fully healed, its tensile strength is expected to reach only 80% of what it was before the injury.4
Three categories of causative factors for SWD have been identified by the World Union of Wound Healing Society (WUWHS). These include technical issues, mechanical stress, and disrupted healing (Figure 1). Some common causes of SWD in the lower extremity include poor tissue quality, ischemia, infection, inferior surgical technique, wound tension or pressure, diabetes, malnutrition, smoking, and obesity3-5 (Figure 1).
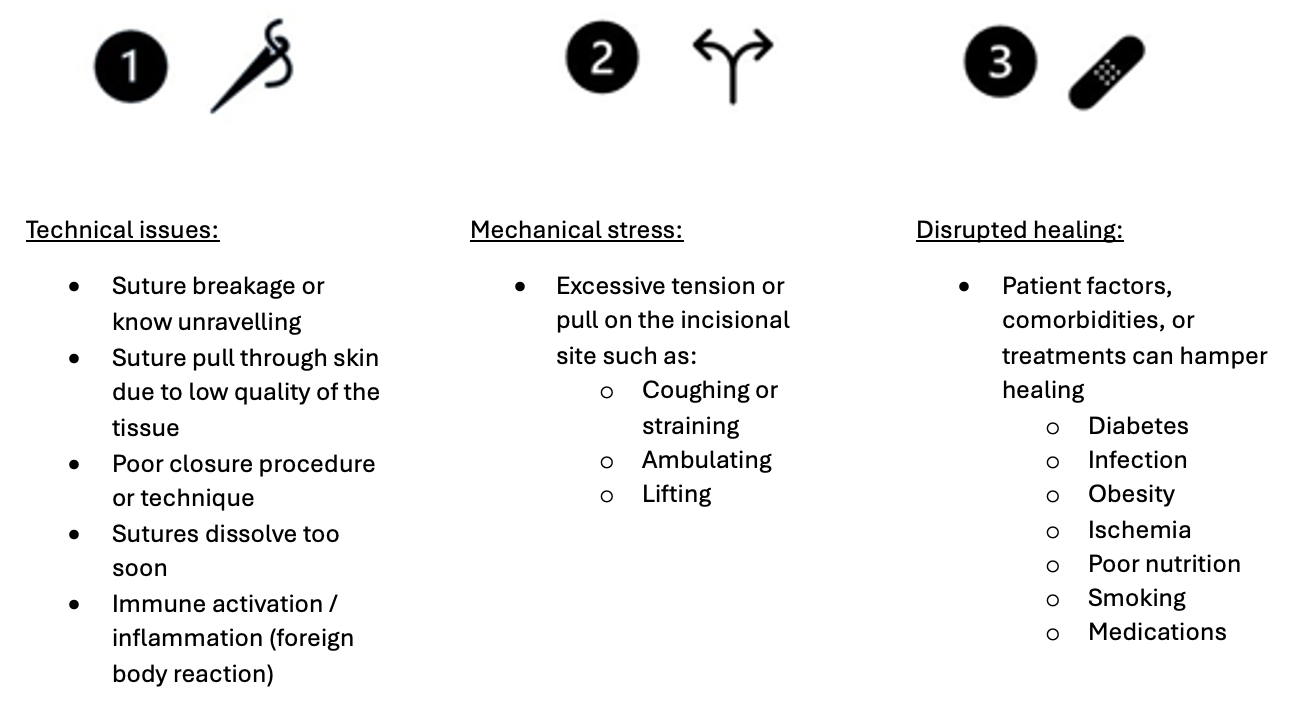
Figure 1. The 3 causes of surgical wound dehiscence.
Although underreporting and varying terminology make it difficult to effectively track the rate of SWD occurrence, studies have estimated that there is an incidence of 1.1% to 3.6% among orthopedic surgery.6,7 While not all occurrences of wound dehiscence are due to infection, there is a high likelihood that an infection can develop the longer the wound remains open; thus, SWD can increase patient morbidity and mortality. In a 2008 publication based on SWD database findings, Shanmugam et al reported a 9.6% mortality rate, an average hospital stay of 9.4 days, and an average cost of $40 323 per occurence.8 Additionally, the Veterans Health Administration has reported that patients with SWD have a 61% greater chance of hospital readmission vs patients without SWD.9
While there is not a singular “gold standard” therapy for managing SWD, the goal is expediting wound closure. Essential steps in this process include draining abscesses, seromas, or hematomas, debridement of nonviable tissue, cleansing the periwound area, reversing ischemia, treating infection, reducing tissue stresses, mitigating edema, and controlling patient factors and comorbidities.1 Clinicians should choose active wound therapies that promote an optimal wound healing environment, thus supporting the wound-healing cascade across the continuum.
Topical oxygen therapy (TOT) is an innovative way of administering oxygen to wounds to promote tissue healing.10 Continuous topical oxygen therapy (cTOT) is a form of TOT that delivers a continuous flow of low‑pressure oxygen to the wound 24 hours a day, 7 days a week. A growing body of high-level evidence advocates the use of cTOT as a beneficial adjunct to wound healing in complex, hypoxic wounds with substantive meta-analyses, randomized controlled trials, and real-world evidence across wound etiologies.11-16 Based on the authors' experience, cTOT has been a highly effective, noninvasive solution for chronic wound treatment. By enhancing microcirculation and elevating tissue oxygenation, cTOT can significantly accelerate the healing process. Therefore, it stands to reason that this therapy could play a transformative role in addressing SWD effectively. This report examines the feasibility of using a cTOT device (NATROX O2; NATROX Wound Care,) as part of a treatment algorithm to treat SWD of the lower extremity.
Methods
This single-center, retrospective analysis of lower-extremity SWD treated with cTOT was conducted in accordance with the Health Portability and Accountability Act guidelines and in adherence to the tenets of the International Conference on Harmonization E6 Good Clinical Practice and the Declaration of Helsinki. This retrospective review was exempt from institutional review board approval. All patients provided written informed consent to publish the case details and associated deidentified images. No compensation was provided.
A third party, not associated with the physician group, performed a retrospective chart review to collect data on lower-extremity SWD for a period of 8 months from January to August 2024. Eligible patients were at least 18 years old and had a history of an SWD with a diameter of at least 1.0 cm that was treated with cTOT to the time of wound closure. Demographics, surgical intervention, and clinical course details were recorded without any identifying data. All patients’ past medical history, smoking status, date of surgery, date of wound dehiscence, date of initial application of cTOT, and time to wound closure were documented, as was the grade of dehiscence and infection status. Each dehiscence was graded using the WUWHS SWD Sandy Grading System.17 This system is a widely accepted, standardized way to assess the extent of an SWD, aiding in treatment decision making and communication between health care providers. The system utilizes a grading scale based on the depth of the wound disruption, including the exposure of subcutaneous tissue, fascia, and underlying organs. Wounds were considered infected if they showed 2 or more clinical signs and symptoms of wound infection per the Infectious Diseases Society of America guidelines18 and/or were prescribed oral or intravenous antibiotics to treat the surgical site during the postoperative period.
All dehisced surgical sites were treated with the standard of care including wound cleansing, debridement when indicated, and appropriate offloading. Additionally, cTOT was applied directly to the surgical site dehiscence per manufacturer guidelines and covered with a semipermeable dressing to maintain a moist wound environment. Patients were seen weekly for evaluation and assessment until complete wound closure.
Results
Nine patients, 4 men and 5 women, were included in this case review. The mean patient age was 52.6 years (range, 35-76 years). SWD occurred after a variety of interventions in the lower extremity, as listed in Table 1. The most common comorbidity reported in the patients was being a current smoker, accounting for 44.4% (4) of patients. This was followed by Type II diabetes mellitus, sleep apnea, and high cholesterol, each of which accounted for 33.3% (3) of patients. The authors were unable to make any correlation between comorbidities and SWD occurrence because of this small sample size. All demographic parameters are outlined in Table 1.
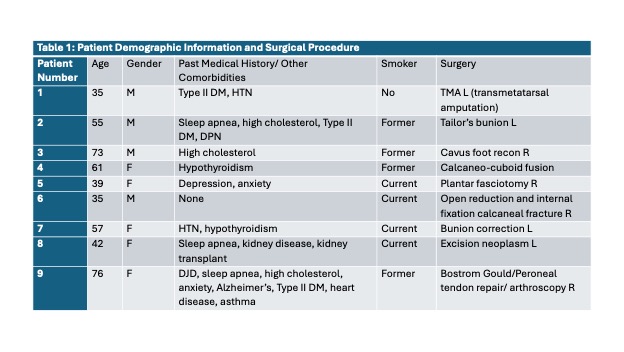
Abbreviations: DJD = degenerative joint disease; DM = diabetes mellitus; F = female; HTN = hypertension; L = left; M = male; R = right; TMA = transmetatarsal amputation.
All patients’ SWD grade was either 3 or 4, with some patients having subcategorizations of 3a. Of the wounds, 66.6% (6) were graded as a 3, 50% (3) of which had signs of infection. The other 33.3% (3) of wounds were graded as a 4. The mean number of days from starting TOT to the SWD healing was 52.6 (range, 22-154 days). In addition, the average estimated SWD surface area based on the wound measurement at the start of delivering TOT was 19.5 cm2 (range, 3-72 cm2). Wound characteristics and the healing timeline for each patient are shown in Table 2.
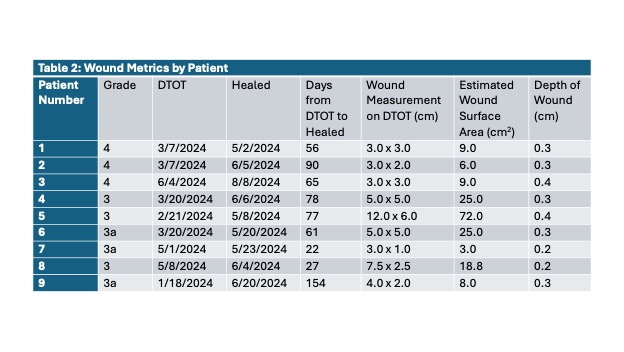
Wound metrics including surgical wound dehiscence (SWD) grade, date continuous topical oxygen was applied (DTOT), date SWD healed, days to healing after starting topical oxygen therapy, wound measurements, and depth on date topical oxygen was applied.
The average time to wound healing for all patients was 70 days. Patients 5 and 9 were noted as outliers, with patient 5 having a significantly larger wound measurement on the date cTOT was applied, and patient 9 having a longer wound healing time. Patient 9’s medical history included comorbidities that may have contributed to the protracted healing time observed. After excluding patient 9, the average time to wound healing was 59.5 days. Specific patient cases and wound healing photos are illustrated in Figure 2.
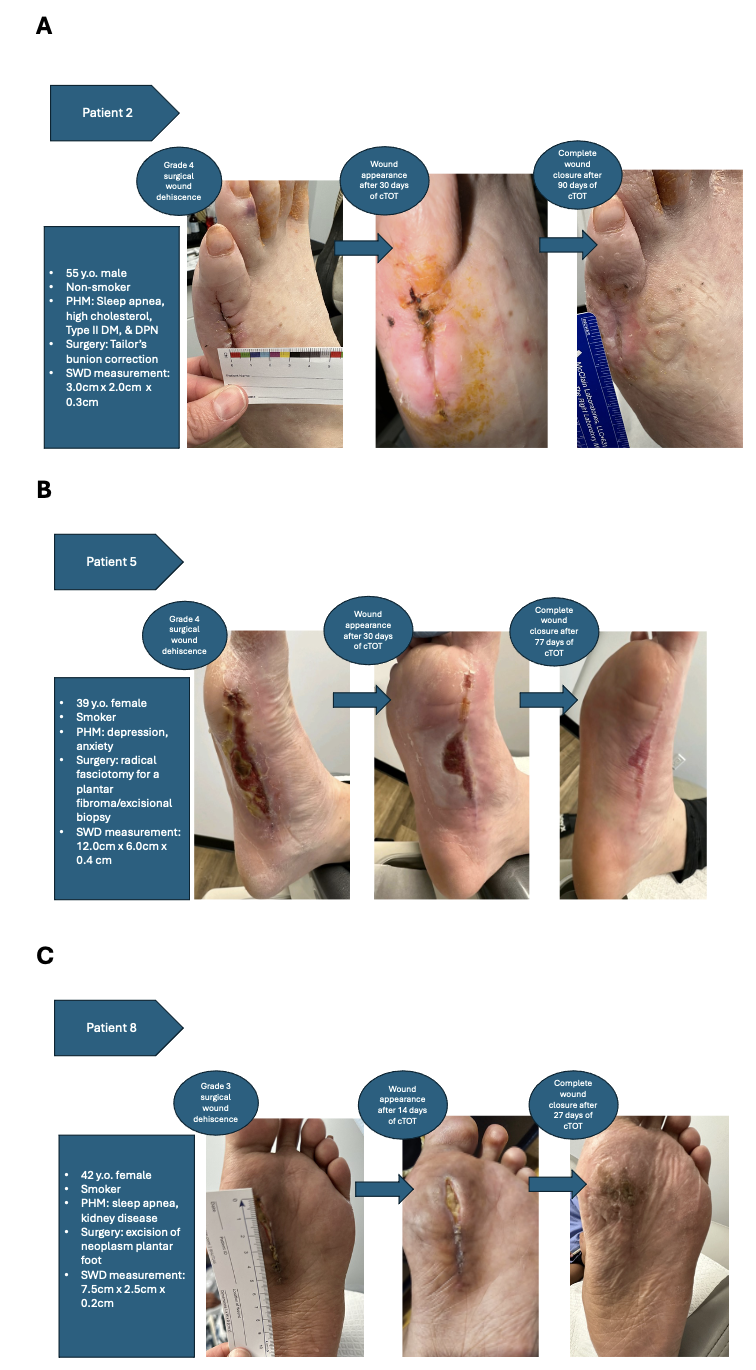
Figure 2. Case examples with wound progression photos: (A) patient 2, (B) patient 5, and (C) patient 8. cTOT = continuous topical oxygen therapy; DM = diabetes mellitus; DPN = diabetic peripheral neuropathy; PHM = past medical history; SWD = surgical wound dehiscence.
Discussion
Current options for SWD management include second intent healing, local tissue flaps, skin grafts, and direct primary closure. Secondary intention healing often results in a prolonged postoperative course with frequently seen wound infection. Thus, the complications of SWD can significantly burden patients and increase overall health care costs. cTOT was effective in decreasing SWD complications in study patients and no patient experienced wound infection or a “return to acute” after the therapy was initiated. Additionally, no patient in this study required additional surgical intervention.
Certain patient factors and comorbidities can complicate wound healing. In a recently published literature review, Jenkins et al reported that age, gender, diabetes, smoking status, history of deep vein thrombosis, ulcer area, and ulcer duration at time of first assessment are prognostic factors contributing to wound healing delays.19 Additionally, risk factors for SWD include patients older than 65 years, hypertension, type of surgical procedure, extended operative time, wound infection, incision location, and suture material.20 The authors were unable to make any correlation between comorbidities, patient factors, and SWD occurrence because of this small sample size, but future investigations should continue to analyze comorbidities to determine if a correlation exists.
There is a paucity of epidemiological data regarding the healing rates of SWD. Thus, it is difficult to accurately predict the time for these wounds to heal. However, the UK National Health Service hospital audit reports estimate that up to 28% of all surgical wounds are receiving care for secondary wound healing in both in-patient and community settings.21,22 The standard of care for SWD involves regular dressing changes and often requires packing of the wound deficit. Again, the literature is lacking in what additional therapies are being used to treat SWD and how frequently they are being applied. A systematic review by Vermeulen et al of dressings and topical agents for the healing of surgical wounds by secondary intention concluded that only small, poor-quality trials exist, rendering the evidence insufficient.23 Therefore, with limited trials conducted on these wounds, a “gold standard” therapy has yet to emerge.
A strength of this review is the patient data, as it provides a useful baseline for relating cTOT and SWD healing in the patients included in the case review. The mean wound healing time for the whole cohort is 70 days, including both outliers. However, the adjusted mean time to wound healing, after removing patient 9, was only 59.5 days. Moreover, this cohort includes patients who were current smokers, had comorbid conditions such as diabetes, and had signs of postoperative infection. Uncomplicated healing outcomes were illustrated in all cases, suggesting that patients who do not have clinically significant hindrances in wound dehiscence healing may also benefit from cTOT. This method of cTOT (NATROX O2; NATROX Wound Care) consists of a battery-powered, lightweight, wearable device that generates pure oxygen from the environment and delivers it into the wounded tissue continuously at a rate of 11 mL per hour for 24 hours a day (Figure 3).
Figure 3. Components of the continuous topical oxygen device: (A) battery-powered oxygen generator and (B) oxygen delivery system.
Oxygen is an essential part of wound healing, including the process of oxidative killing of bacteria, cellular signaling through growth factors and cytokines and proliferation, collagen deposition, and angiogenesis.
Limitations
The major limitation of this study is that it is a single-center, retrospective case series. Additionally, the sample size is small, making it difficult to arrive at conclusive determinations on the overall effectiveness of cTOT on SWD. However, the results of this retrospective case series are compelling enough to support future studies of cTOT in the treatment of SWD in a broader population.
Conclusions
To the author’s knowledge, this is the only patient-cohort study assessing the utility of cTOT in treating surgical dehiscence of the lower extremity. The positive outcomes exhibited in this case series suggest that cTOT is an effective treatment in the management of SWD in patients, regardless of specific surgical intervention. Furthermore, all the SWDs treated with cTOT progressed to wound closure without further need for surgery, hospitalization, or other costly procedures. Thus, using cTOT as an early intervention for SWD in the lower extremity can potentially lessen the overall cost of care in this patient population.
Acknowledgments
Authors: Edward Kormylo, DPM1; Windy Cole, DPM2; Jacob Wielgomas, MSII2
Affiliations: 1Suffolk Foot and Ankle Clinic, Patchogue, New York; 2Kent State University College of Podiatric Medicine, Independence, Ohio
Correspondence: Windy Cole, DPM, Director of Wound Care Research, Kent State University College of Podiatric Medicine, 7000 Euclid Avenue, Suite 101, Cleveland, OH 44103, USA. E-mail: Wcole4@kent.edu
Ethics: The retrospective case study was conducted in accordance with Health Insurance Portability and Accountability Act guidelines, adhered to tenets of the International Conference on Harmonization E6 Good Clinical Practice (ICH GCP) and the Declaration of Helsinki. This retrospective review was exempt from IRB approval. All patients provided written informed consent to publish the case details and associated de-identified image assessments. No compensation was provided for participation.
Disclosures: Dr Cole is a member of the NATROX Wound Care Clinical Advisory Board. The remaining authors disclose no financial or other conflicts of interest.
References
1. Sandy-Hodgetts K, Leung E, Andrews E, et al. Surgical wound dehiscence (SWD): International consensus statement on assessment, diagnosis and management. London: Wounds International; 2023. Accessed June 23, 2025. https://www.woundsinternational.com.
2. Wernick B, Nahirniak P, Stawicki SP. Impaired Wound Healing. [Updated 2023 Aug 28]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK482254/
3. Janis JE, Kwon RK, Lalonde DH. A practical guide to wound healing. Plast Reconstr Surg. 2010;125(6): 230e-244e. doi:10.1097/PRS.0b013e3181d9a0d1
4. Rosen RD, Manna B. Wound Dehiscence. [Updated 2023 May 1]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK551712/
5. Riou JP, Cohen JR, Johnson H Jr. Factors influencing wound dehiscence. Am J Surg. 1992;163(3):324-330. doi:10.1016/0002-9610(92)90014-i
6. Kim KY, Anoushiravani AA, Long WJ, Vigdorchik JM, Fernandez-Madrid I, Schwarzkopf R. A meta-analysis and systematic review evaluating skin closure after total knee arthroplasty-what is the best method? J Arthroplasty. 2017;32(9):2920-2927. doi:10.1016/j.arth.2017.04.004
7. Krishnan R, MacNeil SD, Malvankar-Mehta MS. Comparing sutures versus staples for skin closure after orthopaedic surgery: systematic review and meta-analysis. BMJ Open. 2016;6(1):e009257. doi:10.1136/bmjopen-2015-009257
8. Shanmugam VK, Fernandez SJ, Evans KK, et al. Postoperative wound dehiscence: predictors and associations. Wound Repair Regen. 2015;23(2):184-190. doi:10.1111/wrr.12268
9. Rosen AK, Loveland S, Shin M, et al. Examining the impact of the AHRQ Patient Safety Indicators (PSIs) on the Veterans Health Administration: the case of readmissions. Med Care. 2013;51(1):37-44. doi:10.1097/MLR.0b013e318270c0f7
10. Frykberg R, Andersen C, Chadwick P, et al. Use of topical oxygen therapy in wound healing. J Wound Care. 2023;32(Sup8b):S1-S32. doi:10.12968/jowc.2023.32.Sup8b.S1
11. Serena T, Andersen C, Cole W, Garoufalis M, Frykberg R. Guidelines for the use of topical oxygen therapy in the treatment of hard-to-heal wounds based on a Delphi consensus. J Wound Care. 2021;30(Sup9):S30-S34. doi:10.12968/jowc.2021.30.Sup9.S30
12. Gottrup F, Dissemond J, Baines C, et al. Use of oxygen therapies in wound healing. J Wound Care. 2017;26(Sup5):S1-S43. doi:10.12968/jowc.2017.26.Sup5.S1
13. Serena TE, Bullock NM, Cole W, et al. Topical oxygen therapy in the treatment of diabetic foot ulcers: a multicentre, open, randomised controlled clinical trial. J Wound Care. 2021;30(Sup5):S7-S14. doi:10.12968/jowc.2021.30.Sup5.S7
14. Kaufman H, Gurevich M, Tamir E, Keren E, Alexander L, Hayes P. Topical oxygen therapy stimulates healing in difficult, chronic wounds: a tertiary centre experience. J Wound Care. 2018;27(7):426-433. doi:10.12968/jowc.2018.27.7.426
15. Keren E, Tamir E, Edward G, Kaufman H, Alexander L, Gurevich M. Topical oxygen therapy used to improve wound healing in a large retrospective study of wounds of mixed aetiology. Wounds International. 2021;12(2):63-68.
16. Sen CK. Wound healing essentials: let there be oxygen. Wound Repair Regen. 2009;17(1):1-18. doi:10.1111/j.1524-475X.2008.00436.x
17. Sandy-Hodgetts K. Clinical innovation: the Sandy Grading System for surgical wound dehiscence classification-a new taxonomy. Wounds International. 2017;8(4):6-11.
18. Practice guidelines. Infectious Diseases Society of America (IDSA). Accessed September 9, 2024. https://www.idsociety.org/practice-guideline/practice-guidelines
19. Jenkins DA, Mohamed S, Taylor JK, Peek N, van der Veer SN. Potential prognostic factors for delayed healing of common, non-traumatic skin ulcers: a scoping review. Int Wound J. 2019;16(3):800-812. doi:10.1111/iwj.13100
20. Chun JJ, Yoon SM, Song WJ, Jeong HG, Choi CY, Wee SY. Causes of surgical wound dehiscence: a multicenter study. J Wound Manag Res. 2018;14(2):74-79. doi:10.22467/jwmr.2018.00374
21. Srinivasaiah N, Dugdall H, Barrett S, Drew PJ. A point prevalence survey of wounds in north-east England. J Wound Care. 2007;16(10):413-416, 418-419. doi:10.12968/jowc.2007.16.10.27910
22. Vowden KR, Vowden P. The prevalence, management and outcome for acute wounds identified in a wound care survey within one English health care district. J Tissue Viability. 2009;18(1):7-12. doi:10.1016/j.jtv.2008.11.004
23. Vermeulen H, Ubbink DT, Goossens A, de Vos R, Legemate DA. Systematic review of dressings and topical agents for surgical wounds healing by secondary intention. Br J Surg. 2005;92(6):665-672. doi:10.1002/bjs.5055
24. Frykberg RG. Topical wound oxygen therapy in the treatment of chronic diabetic foot ulcers. Medicina (Kaunas). 2021;57(9):917. doi:10.3390/medicina57090917