

A Tale of Two States: Examining the Best and Worst Performing States for HPV Vaccination
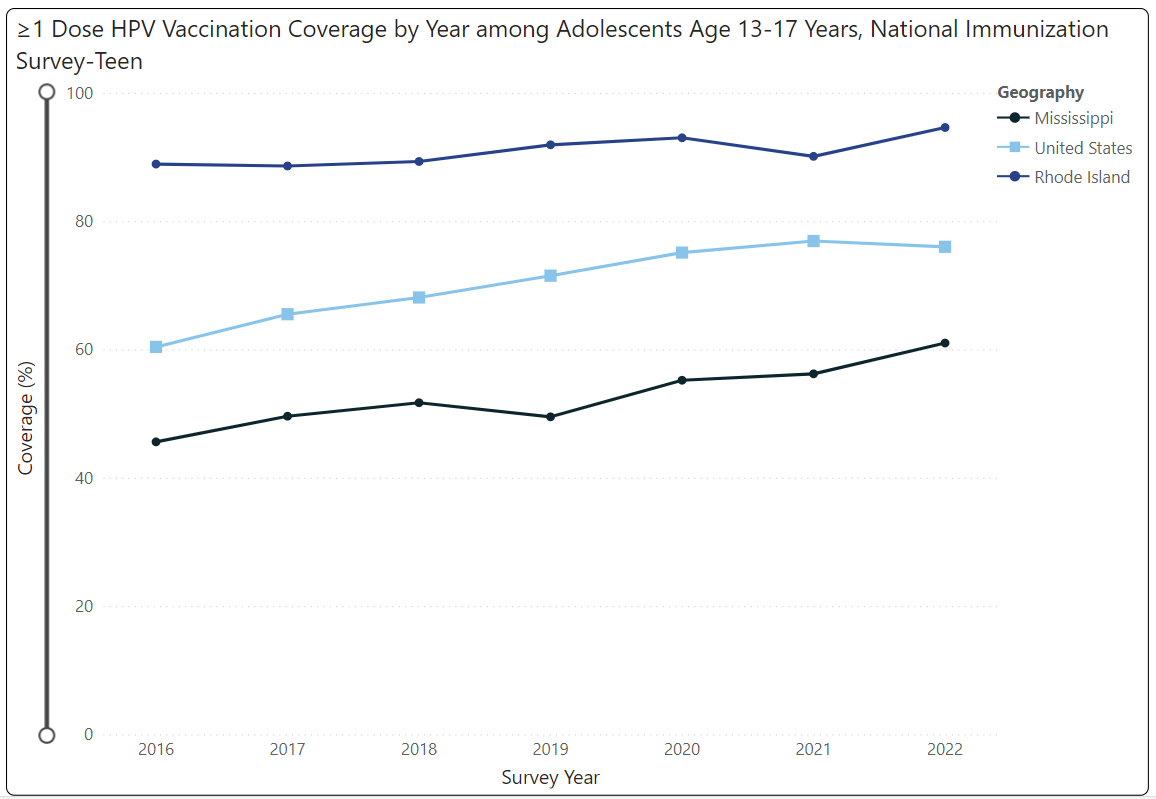
This blog post is the last in a three-part series exploring the disparities related to human papilloma virus (HPV) vaccination rates in the US. Throughout this series, we have shed light on the geographic and racial/ethnic disparities that paint a complex picture of our nation’s battle against HPV. We now turn our attention to two emblematic states: Rhode Island (RI) and Mississippi (MS). These states stand at opposite ends of the spectrum; RI leads the charge with an impressive 95% HPV vaccination coverage (one or more doses) among adolescents aged 13-17, and MS trails with just 61% coverage for the same population. Through this post, we aim to identify the factors that contribute to the stark contrast in HPV vaccination status between the best performing and worst performing state. By understanding these differences, we can glean insights to bolster HPV vaccination rates, thereby mitigating the devastating impacts of HPV infection and related cancers.
Rhode Island
As the nation’s smallest state by land area, RI lacks local public health departments, positioning the RI Department of Health (RIDOH) as the singular public health authority. Consequently, RIDOH collaborates with primary care providers, pharmacies, and community organizations to promote vaccine accessibility for their residents.
RI teens are either at or above the national average for every vaccine type. RIDOH attributes this to their community partners, health care workforce, and child and adult immunization registry. This registry serves as a single source of data that can be accessed by health care professionals across the state to coordinate care and ensure individuals receive the recommended vaccinations. Additionally, RI’s universal vaccine policy stipulates that RIDOH purchase all ACIP (Advisory Committee on Immunization Practices) recommended vaccines for children, adolescents, and most adults at a discounted rate through a CDC federal contract. Vaccines are then provided to immunization-administering clinicians at no cost. Removing the cost barrier for providers to procure vaccines ensures more equitable access to immunizations.
Beginning in 2015, RI’s Vaccine Advisory Committee voted to recommend HPV vaccination as a mandatory requirement for school attendance, with a corresponding public health educational campaign on the importance of HPV vaccination. Support for this initiative was critical. The primary advocate of this policy was the Ocean State Immunization Collaborative, a nonprofit organization dedicated to enhancing vaccine rates. This collaborative consists of several organizations, including the American Cancer Society, the American Academy of Pediatrics, and the Academy of Family Physicians. The collaborative engaged its community partners in advocacy efforts at the local level by partnering with clinicians and initiating a grassroots campaign to bolster support for the HPV vaccine. Results from this initiative indicated that among both males and females 13-17 years of age, there was a notable increase in one or more doses of the HPV vaccine in 2015.
To enhance immunization coverage and identify and reduce instances of missed vaccination opportunities, state immunization programs and other public health entities employ the CDC’s quality-improvement program, AFIX (Assessment, Feedback, Incentives, and eXchange). AFIX is a continuous quality improvement process grounded in research that aims to elevate the rates and standards of immunizations at the provider level. The program’s framework emphasizes the importance of direct, in-person engagement with vaccine-administering health care staff. RIDOH’s goal is to conduct an AFIX site visit at half of the pediatric practices in the state each year, exceeding the CDC recommendation of 25% of practices each year.
RIDOH applied for and received a Prevention and Public Health Fund (PPHF) cooperative agreement award with CDC in 2014. This award supported the development and implementation of an “enhanced AFIX visit,” the goal of which is to add physician-to-physician education with a special focus on HPV disease and vaccination. RIDOH contracted with an OB/GYN and reproductive endocrinologist to conduct these site visits, prioritizing 50 pediatric practices that had the lowest rates of HPV vaccination among their patient population. This PPHF funding was also used to support HPV vaccination clinics in public middle schools, and a public health education campaign. This campaign included television, radio, social media, and print ads in addition to community information sessions at various locations around the state to address parental concerns.
Mississippi
MS is ranked the lowest in the nation for rates of HPV vaccination coverage (one or more doses) among adolescents aged 13-17. Only 61% of teens were covered as of 2022, though the rate has increased markedly over the past several years from 46% in 2016. As previously explored in this blog series, geographic disparities in HPV vaccination rates exist across the US, and southern states generally have lower rates. This is likely attributable in part to lower rates of provider recommendation for the HPV vaccine for adolescents in southern regions, and to many southern states (including MS) not adopting Medicaid expansion. We’ve previously shared that provider recommendation is generally established as the strongest driver of vaccination uptake, and there is a positive correlation between state Medicaid expansion and HPV vaccination.
The low HPV vaccination rate in MS is not unique among other poor health outcomes in the state. MS is consistently ranked as one of the least healthy states in the US, based on several health outcomes, stemming from a combination of socioeconomic, environmental, and political factors. The state has high rates of chronic conditions, such as obesity, diabetes, and heart disease, which are exacerbated by widespread poverty, limited access to nutritious food, and lower levels of physical activity. Additionally, MS faces significant health care delivery challenges, including a shortage of health care providers, especially in rural areas, and a high uninsured rate, which impedes residents’ access to timely and appropriate medical care. Educational disparities and low health literacy also contribute to the prevalence of unhealthy lifestyles and the underutilization of preventive care services. Furthermore, systemic issues, such as underfunded public health infrastructure, perpetuate the cycle of poor health outcomes within the state.
While MS has efforts underway to tackle some of these health disparities, there is at least one key gap in the movement to improve HPV vaccination rates: mandating vaccination for school entry. Though MS does have an immunization registry where providers and parents can access childhood vaccination records, the Mississippi State Department of Health indicates HPV as a recommended, but not required, vaccination for students from pre-kindergarten to 12th grade. When students miss this critical opportunity to become vaccinated, a significant proportion of them remain at risk for HPV infections and associated cancers. Research suggests that policies around vaccine exemption and abstinence-only education have minimal impact on vaccine rates, while states with sex education polices and an HPV vaccine mandate have higher completion rates. Requiring HPV vaccination for MS students would be an important step toward improving statewide vaccination coverage.
In one promising initiative, MS is involved in the HPV Vaccination Roundtable of the Southeast. Beginning in 2022, representatives of southeastern states where HPV vaccination has historically been the lowest joined forces with St. Jude Children’s Research Hospital, the American Cancer Society, and the National HPV Vaccination Roundtable. The purpose of the Roundtable is to discuss improving HPV vaccination rates in the southeast to prevent HPV cancers through participants’ discussion of their shared challenges and opportunities in vaccination coverage. Additionally, the program’s MS state profile lists advocating for HPV vaccine mandates as a priority action step, demonstrating their evidence-based approach to improving vaccination rates in MS. The Mississippi HPV Roundtable is another initiative aiming to increase HPV vaccination rates in the state. The statewide collaboration of health care providers, academic researchers, nonprofits, and other organizations is dedicated to increasing HPV vaccination through data and technology, strategic planning, education, public awareness, research, and collaboration. While it is still a relatively new group launched in 2020, the Roundtable shows promise with its comprehensive approach to HPV vaccination.
Comparing Disparities in RI and MS
Demographic disparities within RI and MS may further influence their vastly different HPV vaccination rates. In our previous blog, we highlighted potential explanations for the racial and ethnic disparities affecting HPV vaccination initiation and completion rates, including frequency of contact with providers/health system, insurance coverage, and provider recommendation. Vaccine mistrust and lack of information among Black and Latino teens, as well as minority parents, also led to HPV vaccine hesitancy. In comparing demographics of RI and MS, it is evident that some of these factors may be at play. As of 2022, RI’s population of about 1.1 million was 83% White and 9% Black, while MS’s population of about 2.9 million was more diverse, with 59% White residents and 38% Black. The Hispanic population in RI and MS is 18% and 4% respectively, while 4% of the RI population and 1% of the MS population are Asian.
The geographic differences between RI and MS are notable; RI is comparatively homogenous (mostly urban), while MS contains both sparsely populated rural areas and urban centers. Regarding health care access, MS has the lowest number of primary care physicians (PCPs) per capita in the nation, with only 49.1 PCPs per 100,000 residents, in stark contrast to RI, which ranks seventh highest with 88.7 PCPs per 100,000. The ratio of pediatricians per 100,000 children follows a similar trend, with 45.9 and 106.3 pediatricians per 100,000 in MS and RI, respectively. This significant difference in numbers of PCPs and pediatricians could be an important contributing factor to the differing HPV vaccination rates between the two states.
There is also a stark difference in median household income between the two states, with $81,370 in RI and $52,985 in MS, and double the percentage of people in poverty in MS as compared with RI. Similarly, RI has higher rates of individuals with post–high school education, which evidence suggests is associated with higher levels of awareness of HPV and the HPV vaccine. Variations in cultural attitudes toward vaccines, socioeconomic status, and other health infrastructure may be driving differing rates of HPV vaccination between RI and MS.
Lessons Learned from Comparison
Although there are significantly different rates of adolescent HPV vaccination between RI and MS, these best and worst performing states do have several similarities relevant to vaccination coverage. Both states have vaccine registries accessible to patients and providers, which can support HPV vaccination data analysis and trend tracking. Additionally, RI and MS are involved in multiple public health initiatives aimed at improving HPV vaccination rates through collaboration.
Still, the states differ widely in two key areas: vaccine mandates and social determinants of health. RI’s high vaccine rate is likely attributable in part to their HPV vaccination requirement for school entry. The few statewide collaborative efforts toward HPV vaccination mandates in MS are still relatively new and do not yet have the political strength of those seen previously in RI.
Furthermore, RI’s universal vaccine policy—which mandates that RIDOH purchase all ACIP-recommended vaccines for children, adolescents, and most adults at a discounted rate through a CDC federal contract and provide to clinicians at no cost—is also likely highly important to RI’s HPV vaccination success. One must also wonder if RIDOH, as a singular coordinating entity, provides benefits that otherwise wouldn’t be available through individual local health departments. While local customization might be lost, the benefits of consistent messaging and single point of reference might be gained.
As discussed, social determinants of health have an undeniable impact on vaccination knowledge, attitudes, and access. In MS, where accessible, affordable, quality health care is impeded by fewer PCPs and widespread poverty, limited access to nutritious food, and lower educational attainment, HPV rates are significantly lower than RI, where such socioeconomic barriers are not as prevalent.
Looking Ahead
In concluding our three-part journey through the disparities in HPV vaccination rates, the case study of Rhode Island and Mississippi underscores the multifaceted nature of public health interventions, where policy, education, socioeconomic factors, and health care infrastructure collectively influence outcomes. Rhode Island’s success is rooted in a comprehensive strategy that includes a vaccine mandate for school entry, a universal vaccine policy, proactive public health campaigns, and robust health care partnerships that ensure equitable access to immunizations. Mississippi’s struggle, on the other hand, highlights the profound impact of social determinants of health and the need for stronger advocacy, policy change, and community engagement to overcome barriers to vaccination.
The disparities in HPV vaccination rates between RI and MS serve as a reminder that while vaccines are a powerful tool in preventing disease, their effective deployment requires a tailored approach that addresses the unique needs and challenges of each community. To bridge the gap in HPV vaccination coverage, it is imperative that states like MS learn from the successful strategies of states like RI. This involves not only implementing vaccine mandates and enhancing public health campaigns, but also tackling the broader social determinants that hinder access to health care services. As our blog series shows, it is clear that the battle against HPV and related cancers is far from over. However, with informed strategies, collaborative efforts, and a commitment to equity, it is a battle that can be won, ensuring a healthier future for all adolescents across the US.
About the Quality Outlook Commentary Series
Breakthrough treatments in cancer care, including precision therapies tailored to specific patient factors, are driving rapid changes in the definitions of oncology quality and value. Efforts to implement value-based care models in oncology must meet the demands of evolving science, new best care practices, and shifting patient priorities. Quality measures must be up-to-date and relevant. Payment models must recognize the challenges and costs of managing complex patient populations with diverse needs. In this JCP blog series, Quality Outlook, Real Chemistry will explore key issues in oncology quality and value through posts focused on measurement, value-based payment, and quality improvement.
 Kendall Logan
Kendall Logan
Kendall Logan, MPH, a Manager at Real Chemistry, brings a public health and health equity perspective to her work. In her role, she manages and supports client projects in the quality and value-based care space across a variety of therapeutic areas. Her recent work involved analyses of the oncology quality landscape and quality measurement, utilizing her experience in qualitative research and stakeholder engagement. With a commitment to client success, Kendall strives to provide comprehensive support and guidance to meet clients’ unique needs within the value-based marketplace.

Anne DiSalvo
Anne DiSalvo, MPH, MBA, is a Director at Real Chemistry. She has a background in Medicaid policy and quality improvement, and currently applies her passion for public health and business within Real Chemistry’s Market Access Strategy division. Anne helps clients convey the value of their therapeutics by leading the development of payer value propositions and crafting access strategies. She also oversees and conducts work related to state-level analysis of trends in access, policy, and health inequities.

Erik Muther
Erik Muther, a Senior Vice President at Real Chemistry, is a thought leader and subject matter expert in value-based care and healthcare performance measurement. Erik leads strategy and implementation projects related to primary care transformation, real-world evidence generation, provider engagement, quality measurement and multi-stakeholder collaboration with clients in the health and life sciences industry.

Tom Valuck
Tom Valuck, MD, JD, is a Partner at Real Chemistry. He is a thought leader on health care system transformation and helps lead the firm’s focus on achieving better health and health care outcomes at a lower cost. Tom’s work at Real Chemistry includes facilitating the exploration of next-generation measurement and accountability models for health care delivery systems. He also helps clients develop strategies to achieve success within the value-based marketplace.



