

Iliac Artery Stent Dislodgement: A Rare Transcatheter Aortic Valve Implantation Complication
© 2024 HMP Global. All Rights Reserved.
Any views and opinions expressed are those of the author(s) and/or participants and do not necessarily reflect the views, policy, or position of the Journal of Invasive Cardiology or HMP Global, their employees, and affiliates.
An 82-year-old male patient with severe, symptomatic aortic stenosis was referred for transcatheter aortic valve implantation (TAVI). His background included previous endovascular repair of the abdominal aorta and bilateral iliac artery angioplasty with stents 5 months prior due to abdominal aortic aneurysm and peripheral vascular disease (PAD).
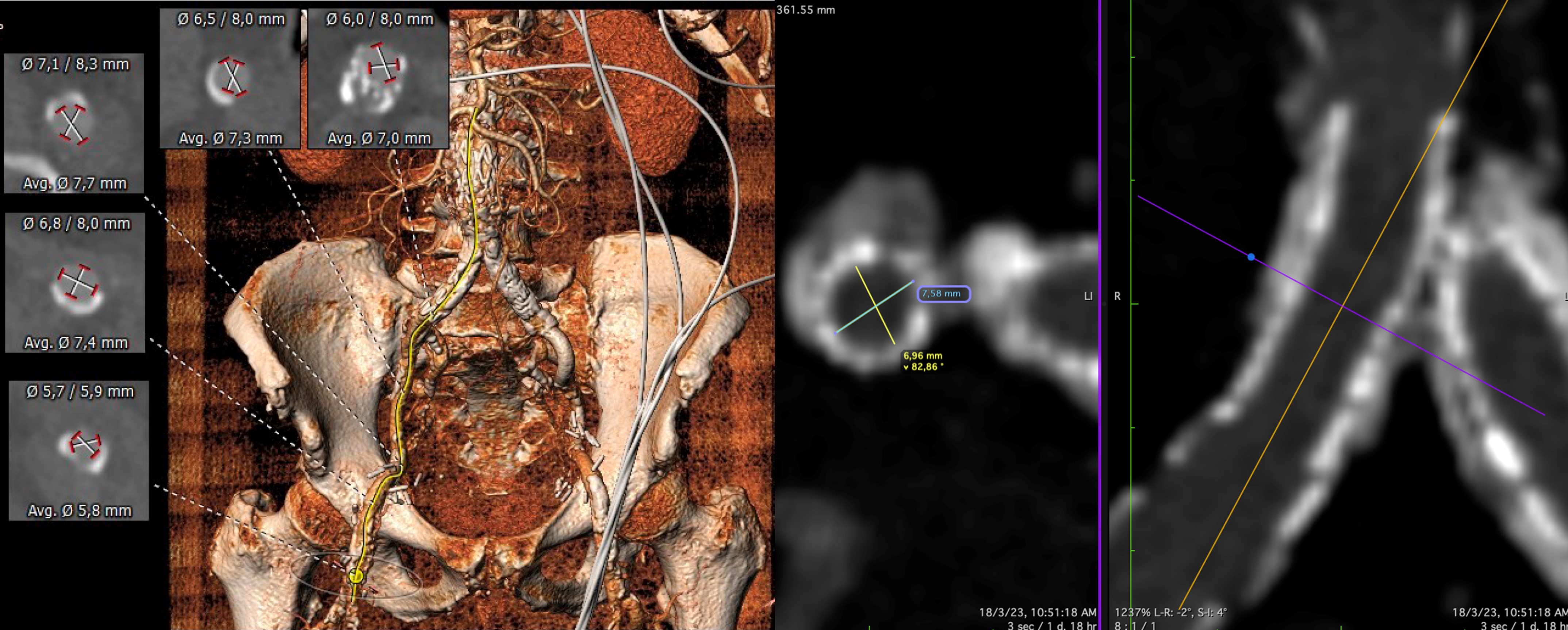
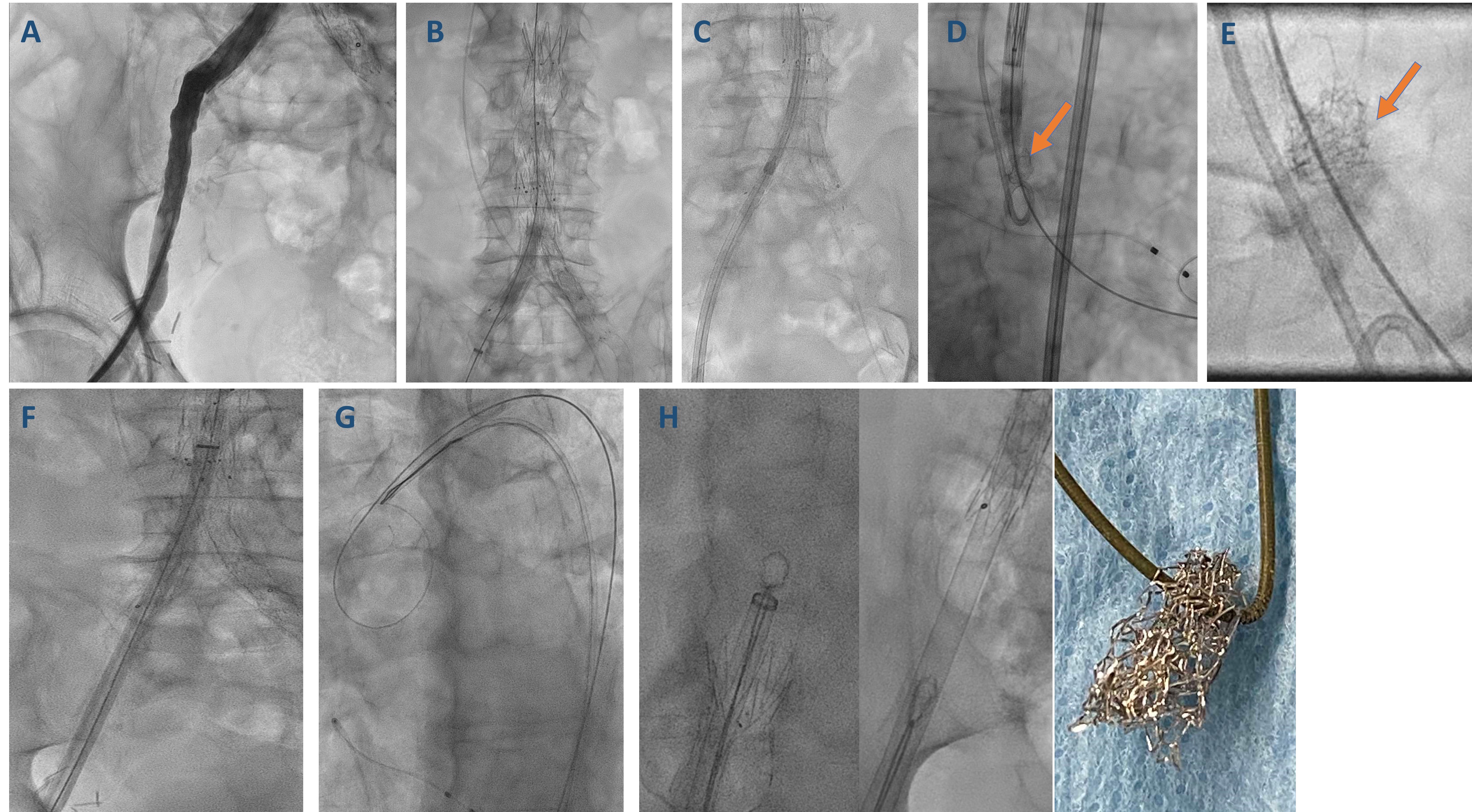
The patient underwent a TAVI computed tomography (CT)-angiography (Figure 1). The heart team decided that the patient was eligible for a right transfemoral TAVI with a 27-mm Navitor valve (Abbott). Right femoral access was gained under ultrasound guidance, and a 14-French (Fr) hydrophilic sheath was inserted after angiographic assessment to the right common iliac and femoral arteries (Figure 2A). The right iliac stents were dilated with an 8 x 40-mm balloon prior to advancement of the valve (Figure 2B). A 27-mm Navitor system was then advanced over a SAFARI 2 guidewire (Boston Scientific) (Figure 2C). After applying careful rotating maneuvers of the delivery system, the valve was advanced through the iliac stents and the aortic endograft to the ascending aorta. At that stage, an oscillating object moving over the guidewire, corresponding to a dislodged iliac artery stent, was noticed (Figure 2D and E; Video 1). The valve was then withdrawn, with further upgrade to a 20-Fr femoral sheath (Figure 2F).
After unsuccessful attempts to entrap and retrieve the dislodged stent with an inflated 6-mm balloon, an Amplatz Goose Neck snare (Medtronic) was advanced to the thoracic aorta, snaring the SAFARI2 guidewire (Figure 2G). The snare with the guidewire and the entrapped stent were then pulled back as a single unit, allowing the successful retrieval of the stent (Figure 2H, Video 2). Finally, a 27-mm Navitor valve was successfully implanted. Final digital subtraction angiography (DSE) did not show any right iliac artery contrast extravasation or anatomy disruption (Video 3).
The transfemoral access route is the preferred option for patients undergoing TAVI since it is associated with improved outcomes. PAD is common amongst TAVI patients, increasing the risk for vascular complications.1 Peripheral artery stent dislodgement is a rare complication of TAVI of which interventional cardiologists should be aware. Snares that are used for retrieval of lost or entrapped equipment are useful to successfully tackle this clinical scenario.
Affiliations and Disclosures
From the 1Department of Cardiology, Mitera General Hospital, Hygeia Healthcare Group, Athens, Greece; 2Second Department of Cardiology, Attikon University Hospital, National and Kapodistrian University of Athens Medical School, Athens, Greece;3Department of Cardiology, Shaare Zedek Medical Center and Faculty of Medicine, Hebrew University of Jerusalem, Israel; 4Department of Cardiology St Thomas’ Hospital, Guy’s and St Thomas’ NHS Foundation Trust, London, United Kingdom.
Disclosures: Dr Dvir is a consultant for Edwards Lifesciences, Medtronic, Abbott, and Pi-Cardia. The remaining authors report no financial relationships or conflicts of interest regarding the content herein.
Address for correspondence: Andreas S. Kalogeropoulos MD, PhD, FRCP, FESC, Department of Cardiology, Mitera General Hospital, Hygeia Healthcare Group, Athens, Greece. Email: andkalog@gmail.com
Reference
1. Palmerini T, Saia F, Kim WK et al. Vascular access in patients with peripheral arterial disease undergoing TAVR: The hostile registry. JACC Cardiovasc Interv. 2023;16(4):396-411. doi: 10.1016/j.jcin.2022.12.009










