

In Between the Cracks
© 2024 HMP Global. All Rights Reserved.
Any views and opinions expressed are those of the author(s) and/or participants and do not necessarily reflect the views, policy, or position of the Journal of Invasive Cardiology or HMP Global, their employees, and affiliates.
A 65-year-old man with end-stage renal failure, severe aortic stenosis, and triple vessel coronary artery disease was admitted for percutaneous coronary intervention (PCI) to the left anterior descending artery (LAD) prior to transcatheter aortic valve replacement (TAVR).
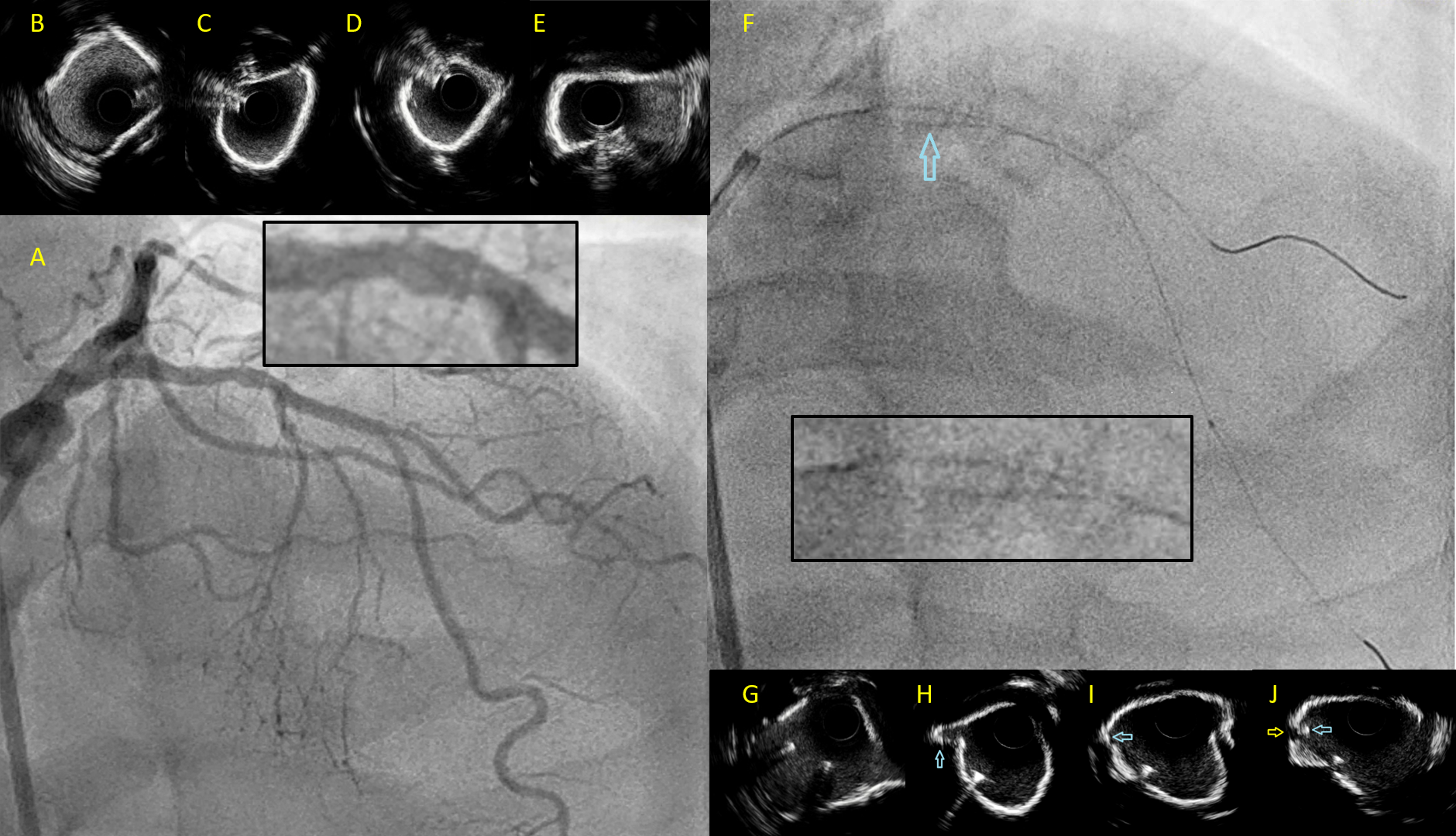
The proximal to mid-LAD had diffuse moderate to severe stenosis (Figure A), with intravascular ultrasound (IVUS) demonstrating eccentric superficial calcification of the proximal LAD followed by a short segment of near concentric calcification at the bifurcation with the major diagonal (Figure B-E).
After wiring both the LAD and the diagonal, the proximal LAD was pre-dilated with a 3.0-mm noncompliant balloon (Figure F). After balloon dilatation, we were unable to deliver any device (IVUS, balloon, guide extension catheter) over the diagonal wire due to heavy resistance at the proximal LAD.
IVUS interrogation over the LAD wire revealed a crack in the calcium parallel to the diagonal wire, with a short segment of the diagonal wire entrapped between 2 shelves of superficial calcium (Figure G-J; Video). The diagonal branch was rewired with a dual lumen microcatheter mounted on the LAD wire. There was no further resistance when delivering balloons on the new diagonal wire. The procedure was completed with 2 drug-eluting stents from the proximal to mid-LAD with a good result.
A common cause of difficulty in delivering devices when 2 or more wires are present is "wire wrapping." Our case illustrates another rare cause of device delivery failure over a guidewire, which can only be appreciated with intravascular imaging. The images in our case demonstrate how an additional wire in-situ acting as a scoring element (as in focused-force angioplasty) can be trapped in calcified plaques after balloon dilatation. A safe and effective bail-out technique using a dual lumen microcatheter was also demonstrated.
Affiliations and Disclosures
From the Department of Cardiology, National Heart Centre, Singapore.
Disclosures: The authors report no financial relationships or conflicts of interest regarding the content herein.
Address for correspondence: Soo Teik Lim, MBBS, National Heart Centre, 5 Hospital Drive, Singapore 169609. Email: lim.soo.teik@singhealth.com.sg










