Safety and Outcomes of Upfront Large-Size Rotational Atherectomy Burrs in Left Main Coronary Interventions
© 2026 HMP Global. All Rights Reserved.
Any views and opinions expressed are those of the author(s) and/or participants and do not necessarily reflect the views, policy, or position of the Journal of Invasive Cardiology or HMP Global, their employees, and affiliates.
J INVASIVE CARDIOL 2026. doi:10.25270/jic/26.00147. Epub July 1, 2026.
Abstract
Objectives. Data on the safety and efficacy of percutaneous coronary intervention (PCI) with adjunctive rotational atherectomy (RA) in left main (LM) disease are limited. Current guidelines recommend using a small-size RA burr initially, with upsizing if required. The safety of upfront use of a large-size RA burr (≥1.75 mm) is unknown. The authors assessed the safety of an upfront large rotablation burr in the treatment of LM calcification and the procedural and long-term outcome of this approach in comparison to a small-size burr.
Methods. Retrospective analysis of all patients undergoing PCI with adjunctive RA to LM disease. The study outcomes were all-cause mortality and repeat target lesion revascularization (TLR) at medium-term follow-up in patients treated with large burr size (≥1.75mm) compared to small burr size (<1.75mm).
Results. Two hundred forty-three patients (mean age 75 ± 9 years, 80% males) were included. Approximately half of the patients were treated with a large-size RA burr (≥1.75 mm). Most treated lesions were bifurcation lesions involving the 3 branches (86%) with SYNTAX score of 35 ± 11. Radial access was used in two-thirds of patients; 7F sheath was the most used. There was no difference between the small and large burr groups in procedural complications (11% vs 8%, P = .512), all-cause mortality (34% vs 28%, P = .267), and repeat TLR up to 4 years after PCI (2.9% vs 2.1%, P = .473).
Conclusions. Upfront use of a large-size RA burr is feasible and safe for treating calcified LM disease, with no increase in procedural complications, repeat TLR, or medium-term all-cause mortality.
Introduction
Coronary artery calcification is present in up to 25% of treated lesions, with an increased risk of complications during percutaneous coronary intervention (PCI).
Current guidelines recommend coronary artery bypass grafting (CABG) for heavily calcified LM lesions with a high SYNTAX score (≥33); however, in patients with increased surgical risk, PCI can be a reasonable alternative. Rotational atherectomy (RA), first introduced in 1978, remains one of the main calcium modification tools used in the treatment of heavily calcified lesions.
Current evidence from predominantly non-LM RA trials suggests that the use of a small burr/vessel ratio (<0.7) is associated with decreased risk of complications.
In this study, we compared the use of a large burr (≥1.75 mm) with a small burr (<1.75 mm) in the treatment of heavily calcified LM lesions, and assessed the immediate and medium-term outcomes including procedural complications, target lesion revascularization (TLR), and 4-year mortality.
Methods
Study design
A retrospective analysis of prospectively collected data on all LM PCI in a tertiary center: Freeman Hospital, Newcastle upon Tyne, United Kingdom. The study was conducted in accordance with the Declaration of Helsinki and Good Clinical Practice guidelines. Anonymized data were obtained from the institutional electronic database normally utilized for patient care; therefore, the need for informed consent was waived by the institution’s medical ethical committee.
All baseline, procedural, and outcome data are prospectively collected, validated, and entered into the electronic database, which was used to obtain all information for analysis.
Study population
All consecutive patients undergoing LM PCI with adjunctive RA that was performed with either the ROTAPRO system or the Rotablator (Boston Scientific) between June 2009 and June 2021 were included. Patients who had incomplete documentation of the procedure or outcome data were excluded.
PCI procedure
The PCI procedure was performed in line with approved standards practice in the United Kingdom. The vascular access site and LM bifurcation PCI strategy with adjunctive RA were left to the operator’s discretion. RA was performed upfront in cases of heavy calcification of the target lesion, or after failed PCI attempts due to non-dilatable lesions. Either ROTAWIRE Floppy or Extra Support guidewires (Boston Scientific) were used at the discretion of the operator. The selected burr size was less than 70% of the vessel diameter.
The burr size and ablation speed were also left to the operator’s discretion. Procedures were performed by experienced operators in RA. Temporary pacing wires were not routinely used unless indicated by significant bradycardia not responding to a conservative approach by short RA use and allowing time to recovery. Mechanical circulatory support devices were occasionally employed, as appropriate.
Study outcomes
The study outcomes were procedural complications, all-cause mortality, and repeat TLR up to a median follow-up of 4 years. Technical success was defined as successful revascularization of coronary lesions with achievement of less than 30% residual diameter stenosis within the treated segment and restoration or maintenance of Thrombolysis in Myocardial Infarction (TIMI) grade 3 antegrade flow.
Statistical analysis
Paired and unpaired t-tests were used for comparison of normally distributed variables, and the Wilcoxon rank-sum test was used for non-normally distributed variables. Data are presented as mean (standard deviation) or median and Q1 to Q3. Dichotomous variables were compared using chi-squared test or Fisher's exact test, as appropriate. The Kaplan-Meier survival methods with log-rank tests were used. Cox regression analysis was performed on all key risk factors in the baseline and procedural characteristics.
Results
A total of 243 patients who underwent RA to LM bifurcation disease were included. Overall, technical success was achieved in 96% of patients (233). The mean age was 74.7 ± 9 years, and males represented almost 80% of cases (194). Approximately half of the patients were treated with a burr sized greater than 1.75 mm (51.4%), and the majority of lesions were bifurcation lesions involving the 3 branches (85.6% [208]). Baseline and procedural characteristics are shown in Tables 1 and 2, respectively.
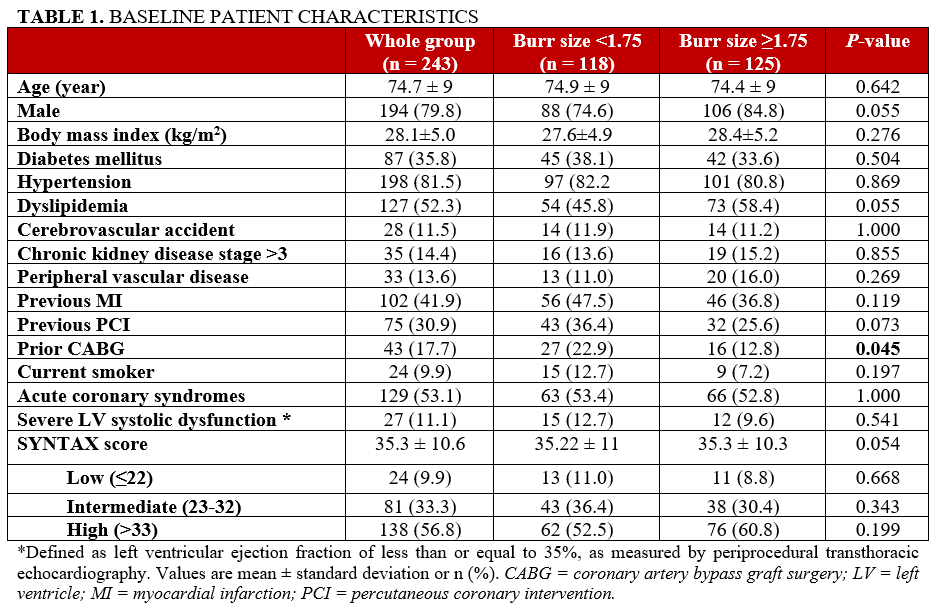
The mean SYNTAX score was 35.3 ± 10.6, reflecting the complex anatomy of patients undergoing RA. Male patients were more likely to be treated with a larger burr size. Hypercholesterolemia was more prevalent in the large-burr-size group, while there were fewer patients with previous CABG (Table 1).
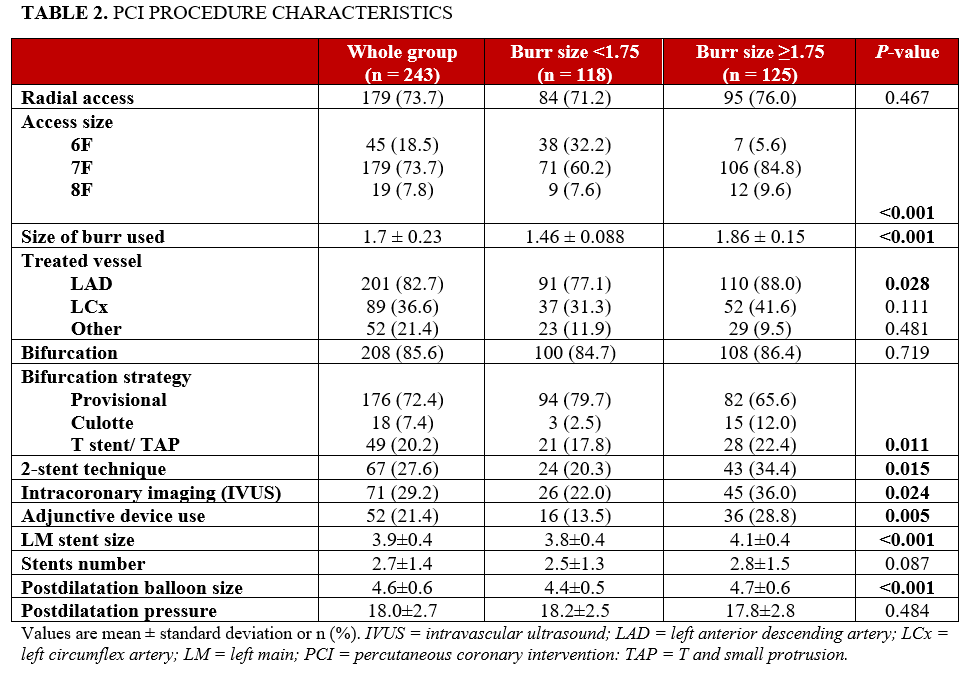
The majority of patients were treated via the radial approach (179 [73.7%]). A 7F compatible sheath (6F/7F Glidesheath Slender [Terumo]) was the most frequently used 179 cases (73.7%). Adjunctive devices such as cutting balloons and intracoronary imaging were used more often in conjunction with a burr sized greater than or equal to 1.75 mm (P = .004 and P = .017, respectively). Upsizing RA burr was only used in 9 patients (3.7%) of the small-burr-size group.
Provisional stenting technique was used more often in the small-burr-size group (94 [79.7%] vs 82 [65.6%]), and the 2-stent technique was employed much more in the large-burr-size group (43 [34.4%]); the Culotte technique used more frequently compared with other techniques (15 [12%]). The use of the T-stent or T-TAP (T and Small Protrusion) technique was similar between groups. LM stent size and postdilatation balloon were significantly larger in the large-burr-size group (Table 2).
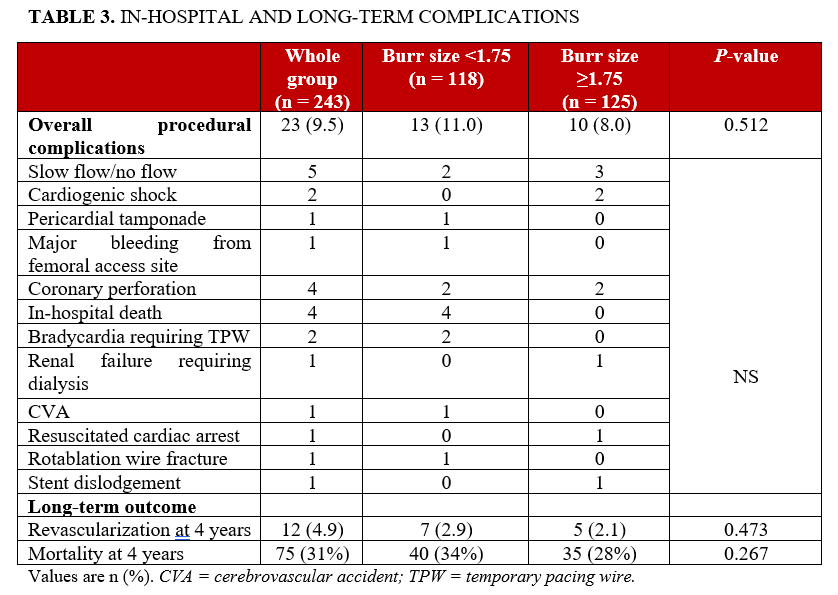
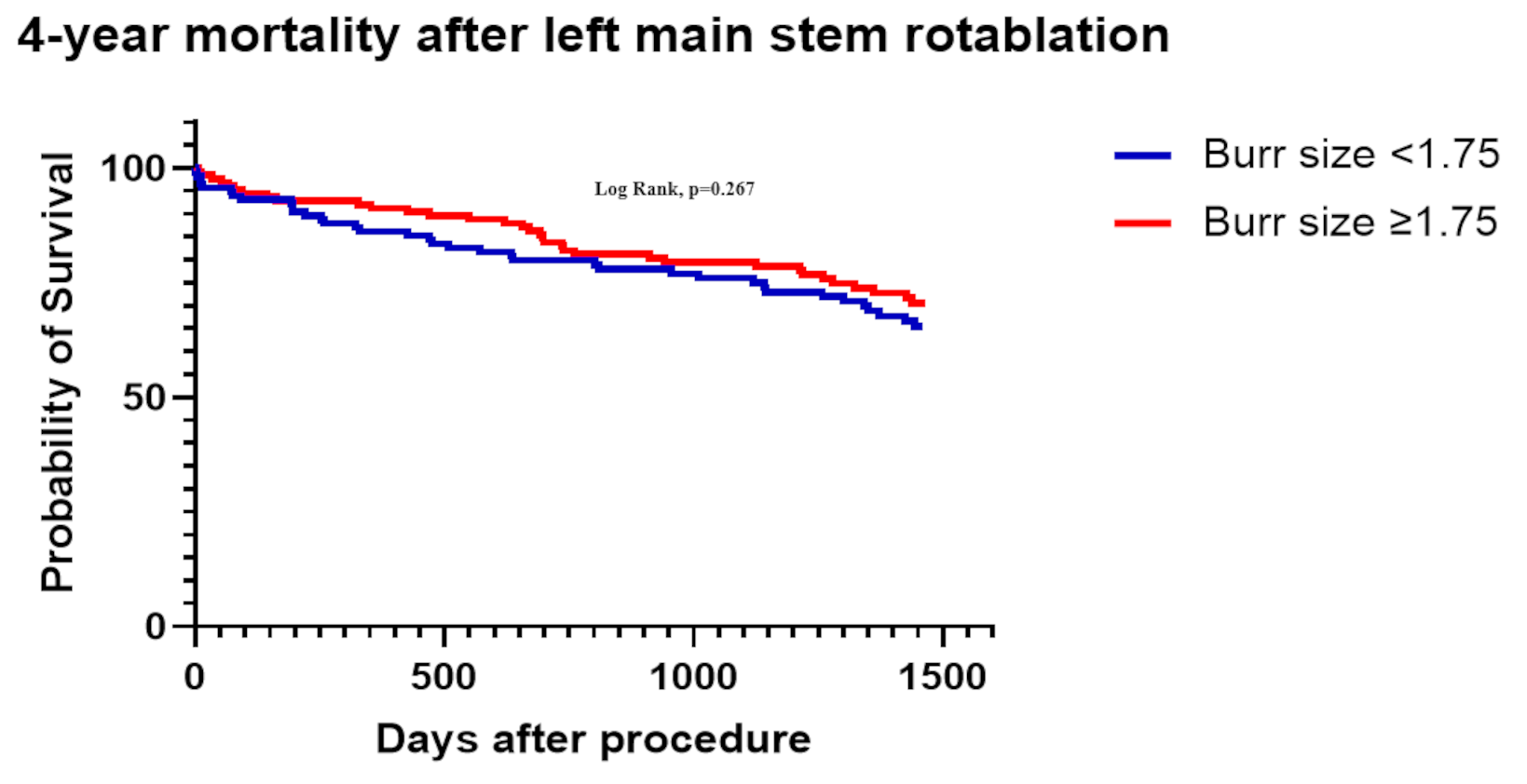
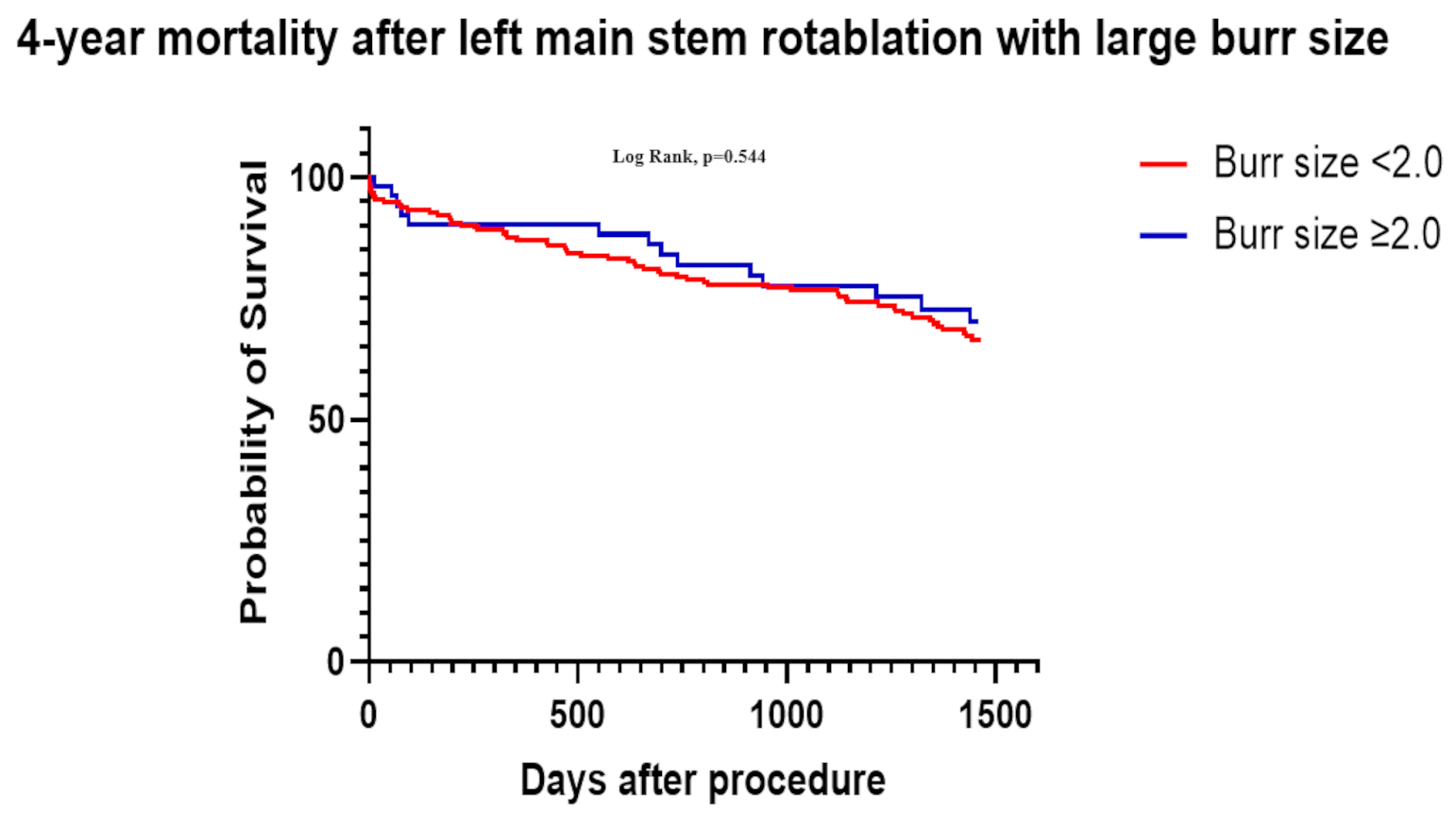
There was no increase in complications rate when a large burr (≥1.75 mm) was used upfront. The overall complications rate was not significantly different between the 2 groups; neither was repeat revascularization at 4 years (2.9% vs 2.1%, P = .487). While the in-hospital mortality was significantly higher in the small- vs large-burr group (1.6% vs 0%, P = .038) (Table 3). There was no significant difference in 4-year mortality between the small- and the large-burr groups (34% vs 28%, P = .267) (Figure 1). Similarly, when we assessed a burr-size threshold of less than 2.0 mm vs greater than or equal to 2.0 mm, there was no significant difference on 4-year mortality (P = .544) (Figure 2).
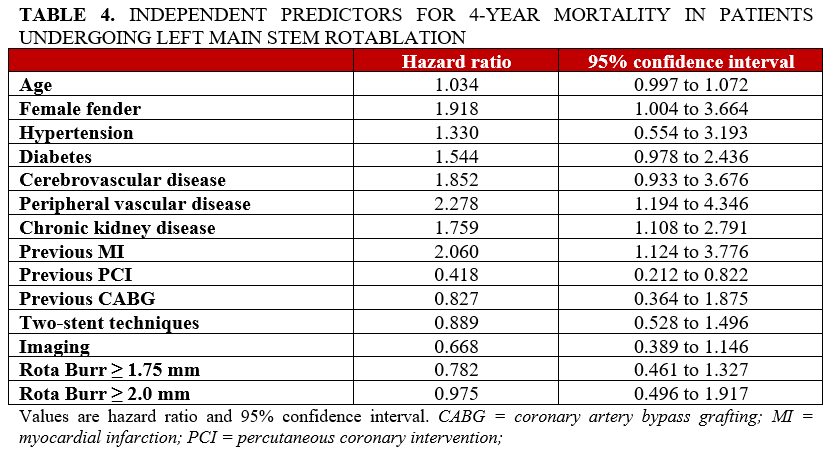
A Cox proportional hazard model showed no effect of large burr size on mortality (hazard ratio, 0.975; 0.496-1.917). The primary factors, which influenced mortality according to the Cox proportional hazard model, were the traditional risk factors for mortality in coronary artery disease (CAD): female gender, peripheral vascular disease, diabetes mellitus, chronic kidney disease, and previous myocardial infarction (MI) (Table 4).
Discussion
This study shows that the use of a large burr size in LM PCI as an initial strategy is safe and effective with a low complication rate, which was not different between groups when using a burr-size threshold of greater than or equal to 1.75 mm. Furthermore, procedure-related complications, repeat revascularization, and mortality were not different between the 2 groups.
To our knowledge, this is the largest cohort of such an approach. The use of larger burr sizes is perceived to be associated with increased risk of complications; hence, the current recommendation by expert consensus documents is the use of small burr size to treat calcified LM disease.
The femoral route was used less often in this study compared with previous ones. While femoral access use was high, ranging from 57% to 80.3%
The Instructions for Use recommendations from Boston Scientific are to use a 7F guide catheter for a 1.75-mm burr and an 8F guide catheter for a 2.0-mm burr. However, the current 6F Launcher guide catheters (Medtronic) can accommodate up to a 1.7-mm burr, and the 7F catheters can accommodate up to a 2.0-mm burr, which allows for the use of larger-size burrs through a smaller arterial access. This is enhanced by the use of the 6F/7F Glidesheath Slender sheaths from the radial and femoral approach, which was adopted by the senior author.
An 8F sheath was used via the radial route in about 50% of our cases (3.7% of the total), suggesting the feasibility of using larger sheath sizes via the radial access route in suitable patients. The use of 8F from the radial artery was done in a sheathless manner, where the initial approach would be 5F/6F, then exchanged for a sheathless 8F. The use of radial access is encouraged, as it has been associated with a lower incidence of complications in the context of rotablation.
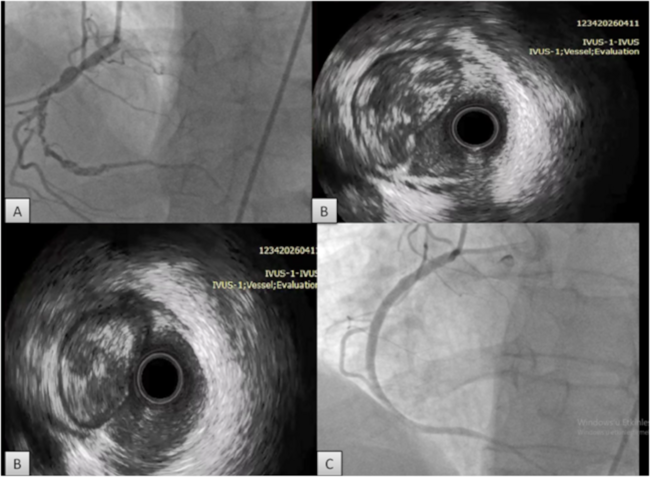
Intracoronary imaging (mostly intravascular ultrasound [IVUS]) was used in 29.7% of our patients, which is higher than reported in previous studies. The European Society of Cardiology gives a class IIa recommendation for the use of IVUS in PCI of unprotected LM lesions,
Prior to the era of coronary stents, the use of RA was associated with an increased risk of complications.
The repeat revascularization rate was low, 4.9%, in the present study compared with higher rates reported historically.
In the context of previous UK experience, we report similar complication rates (9.5%) compared with a large study from 2014 that included patients with both LM and non-LM disease treated with RA; this study reported a complication rate of 9.7%.
There was a low overall in-hospital mortality of 1.6%. Previous studies of RA have reported in-hospital mortality rates of 7.7%.
The 4-year mortality was 31%. Although this rate appears high, previous evidence have suggested a significant survival benefit in high-risk patients undergoing LM RA in comparison with no RA, with an in-hospital mortality of 8.3% vs 29%, respectively.
Mortality risk related to the use of RA in the context of calcific LM disease is difficult to determine, as mortality can also be influenced by other patient-related factors such as complex anatomy, advanced age, and significant comorbidities.
The upfront use of larger burr size as an initial strategy was not associated with worse outcomes in this study. The CARAT
Almost half of the patients in this study were treated with an initial large burr (≥1.75 mm) with a low overall complication rate. This can be explained by the low burr-to-vessel size ratio in our group, which was 0.4 and 0.5 in the small and large groups, respectively. This is consistent with the current expert guidelines from Europe and the United States, which recommend using a burr size of 0.4 to 0.6 for LM intervention.
It is suggested that 1.25 and 1.5 burrs are safer initial burr size options to reduce complications,24 and this is reflected in the current guidelines. It has also been suggested that the use of 1.75-mm burrs could result in more complications,24 which is contrary to our findings. Conversely, it is also known that the use of small burr sizes can be associated with a higher risk of burr entrapment;
Taking all of the data into consideration, we recommend starting with a burr size that is at a 0.5 ratio to the vessel size and following with intravascular imaging; subsequently, a determination can be made as to whether the burr size should be upgraded or whether the starting burr has achieved enough calcium modification. However, the decision to start with a large burr size (≥1.75 mm) appears to be a safe approach in such cases.
Limitations
This is a single-center, retrospective study with all inherent limitations of such studies. The number of operators performing these interventions was low, particularly for the large-burr-size group. Additionally, procedures in this cohort were performed in a high-volume center, which may not apply to other centers. High-volume centers and operators have been shown to be associated with better outcomes compared with lower-volume centers.
Conclusions
An upfront large burr (≥1.75 mm or ≥2.0 mm) in calcified LM interventions is effective, safe, and was not associated with an increased risk of in-hospital complications, need for revascularization, or mortality at 4 years compared with small burr sizes.
Affiliations and Disclosures
Hilal Khan, MD1; Ayman Al-Atta, MD1; Mohamed Farag, MD1,2; Ibrahem Abdalazeem, MD1,2; Fatih Gungoren, MD1; Mohammad Alkhalil, MD1; Ahmed Abdalwahab, MD1; Mia Holley, MD3; Scott Wilkes, MD3; Bilal Bawamia, MD1; Mohaned Egred, MD1,3,4
From the 1Cardiothoracic Department, Freeman Hospital, Newcastle upon Tyne, United Kingdom; 2School of Life and Medical Sciences, University of Hertfordshire, Hertfordshire, United Kingdom; 3School of Medicine, University of Sunderland, United Kingdom; 4Translational and Clinical Research Institute, Newcastle University, Newcastle upon Tyne, United Kingdom.
Dr Khan and Dr Al-Atta served as joint first authors.
Address for correspondence: Mohaned Egred, MD, Cardiothoracic Department, Freeman Hospital, Newcastle, NE7 7DN, United Kingdom. Email: m.egred@nhs.net; X: @mohanedegred
References
1. Copeland-Halperin RS, Baber U, Aquino M, et al. Prevalence, correlates, and impact of coronary calcification on adverse events following PCI with newer-generation DES: findings from a large multiethnic registry. Catheter Cardiovasc Interv. 2018;91(5):859-866. doi:10.1002/ccd.27204
2. Fitzgerald PJ, Ports TA, Yock PG. Contribution of localized calcium deposits to dissection after angioplasty. An observational study using intravascular ultrasound. Circulation. 1992;86(1):64-70. doi:10.1161/01.cir.86.1.64
3. D'Ascenzo F, Elia E, Marengo G, et al. Long-term (≥15 years) follow-up of percutaneous coronary intervention of unprotected left main (from the GRAVITY registry). Am J Cardiol. 2021;156:72-78. doi:10.1016/j.amjcard.2021.06.008
4. Angsubhakorn N, Kang N, Fearon C, et al. Contemporary management of severely calcified coronary lesions. J Pers Med. 2022;12(10):1638. doi:10.3390/jpm12101638
5. Fajadet J, Chieffo A. Current management of left main coronary artery disease. Eur Heart J. 2012;33(1):36-50b. doi:10.1093/eurheartj/ehr426
6. Whitlow PL, Bass TA, Kipperman RM, et al. Results of the study to determine rotablator and transluminal angioplasty strategy (STRATAS). Am J Cardiol. 2001;87(6):699-705. doi:10.1016/s0002-9149(00)01486-7
7. Safian RD, Feldman T, Muller DW, et al. Coronary angioplasty and Rotablator atherectomy trial (CARAT): immediate and late results of a prospective multicenter randomized trial. Catheter Cardiovasc Interv. 2001;53(2):213-20. doi:10.1002/ccd.1151
8. Barbato E, Carrié D, Dardas P, et al; European Association of Percutaneous Cardiovascular Interventions. European expert consensus on rotational atherectomy. EuroIntervention. 2015;11(1):30-36. doi:10.4244/EIJV11I1A6
9. Sharma SK, Tomey MI, Teirstein PS, et al. North American expert review of rotational atherectomy. Circ Cardiovasc Interv. 2019;12(5):e007448. doi:10.1161/CIRCINTERVENTIONS.118.007448
10. Bouisset F, Barbato E, Reczuch K, et al. Clinical outcomes of PCI with rotational atherectomy: the European multicentre Euro4C registry. EuroIntervention. 2020;16(4):e305-e312. doi:10.4244/EIJ-D-19-01129
11. Iannaccone M, Barbero U, D'ascenzo F, et al. Rotational atherectomy in very long lesions: results for the ROTATE registry. Catheter Cardiovasc Interv. 2016;88(6):E164-E172. doi:10.1002/ccd.26548
12. Rola P, Kulczycki JJ, Włodarczak A, et al. Intravascular lithotripsy as a novel treatment method for calcified unprotected left main diseases-comparison to rotational atherectomy-short-term outcomes. Int J Environ Res Public Health. 2022;19(15):9011. doi:10.3390/ijerph19159011
13. Kübler P, Zimoch W, Kosowski M, Tomasiewicz B, Telichowski A, Reczuch K. In patients undergoing percutaneous coronary intervention with rotational atherectomy radial access is safer and as efficient as femoral access. J Interv Cardiol. 2018;31(4):471-477. doi:10.1111/joic.12496
14. Kotowycz MA, Khan SQ, Freixa X, et al. Rotational atherectomy through the radial artery is associated with similar procedural success when compared with the transfemoral route. Coron Artery Dis. 2015;26(3):254-258. doi:10.1097/MCA.0000000000000198
15. Sakakura K, Yamamoto K, Taniguchi Y, Tsurumaki Y, Momomura SI, Fujita H. Intravascular ultrasound enhances the safety of rotational atherectomy. Cardiovasc Revasc Med. 2018;19(3 Pt A):286-291. doi:10.1016/j.carrev.2017.09.012
16. Park SJ, Kim YH, Park DW, et al; MAIN-COMPARE Investigators. Impact of intravascular ultrasound guidance on long-term mortality in stenting for unprotected left main coronary artery stenosis. Circ Cardiovasc Interv. 2009;2(3):167-177. doi:10.1161/CIRCINTERVENTIONS.108.799494
17. Ellis SG, Popma JJ, Buchbinder M, et al. Relation of clinical presentation, stenosis morphology, and operator technique to the procedural results of rotational atherectomy and rotational atherectomy-facilitated angioplasty. Circulation. 1994;89(2):882-892. doi:10.1161/01.cir.89.2.882
18. Warth DC, Leon MB, O'Neill W, Zacca N, Polissar NL, Buchbinder M. Rotational atherectomy multicenter registry: acute results, complications and 6-month angiographic follow-up in 709 patients. J Am Coll Cardiol. 1994;24(3):641-648. doi: 10.1016/0735-1097(94)90009-4
19. Kawamoto H, Latib A, Ruparelia N, et al. In-hospital and midterm clinical outcomes of rotational atherectomy followed by stent implantation: the ROTATE multicentre registry. EuroIntervention. 2016;12(12):1448-1456. doi:10.4244/EIJ-D-16-00386
20. Bouisset F, Ribichini F, Bataille V, et al. Euro4C Registry Investigators. Clinical outcomes of left main coronary artery PCI with rotational atherectomy. Am J Cardiol. 2023;186:36-42. doi:10.1016/j.amjcard.2022.09.031
21. Cockburn J, Hildick-Smith D, Cotton J, et al. Contemporary clinical outcomes of patients treated with or without rotational coronary atherectomy--an analysis of the UK central cardiac audit database. Int J Cardiol. 2014;170(3):381-387. doi:10.1016/j.ijcard.2013.11.018
22. Dahdouh Z, Roule V, Dugué AE, Sabatier R, Lognoné T, Grollier G. Rotational atherectomy for left main coronary artery disease in octogenarians: transradial approach in a tertiary center and literature review. J Interv Cardiol. 2013;26(2):1731-1782. doi:10.1111/joic.12026
23. Cuenza LR, Jayme AC, Khe Sui JH. Clinical outcomes of patients undergoing rotational atherectomy followed by drug-eluting stent implantation: a single-center real-world experience. Heart Views. 2017;18(4):115-120. doi:10.4103/1995-705X.221231
24. Sakakura K, Taniguchi Y, Yamamoto K, et al. Comparison of complications with a 1.25-mm versus a 1.5-mm burr for severely calcified lesions that could not be crossed by an intravascular ultrasound catheter. Cardiovasc Interv Ther. 2020;35(3):227-233. doi:10.1007/s12928-019-00606-9
25. Sakakura K, Ako J, Momomura S. Successful removal of an entrapped rotablation burr by extracting drive shaft sheath followed by balloon dilatation. Catheter Cardiovasc Interv. 2011;78(4):567-570. doi:10.1002/ccd.22957