

When Spasm Mimics STEMI: A Post-PCI Surprise
© 2026 HMP Global. All Rights Reserved.
Any views and opinions expressed are those of the author(s) and/or participants and do not necessarily reflect the views, policy, or position of the Journal of Invasive Cardiology or HMP Global, their employees, and affiliates.
J INVASIVE CARDIOL 2026. doi:10.25270/jic/26.00154. Epub May 28, 2026.
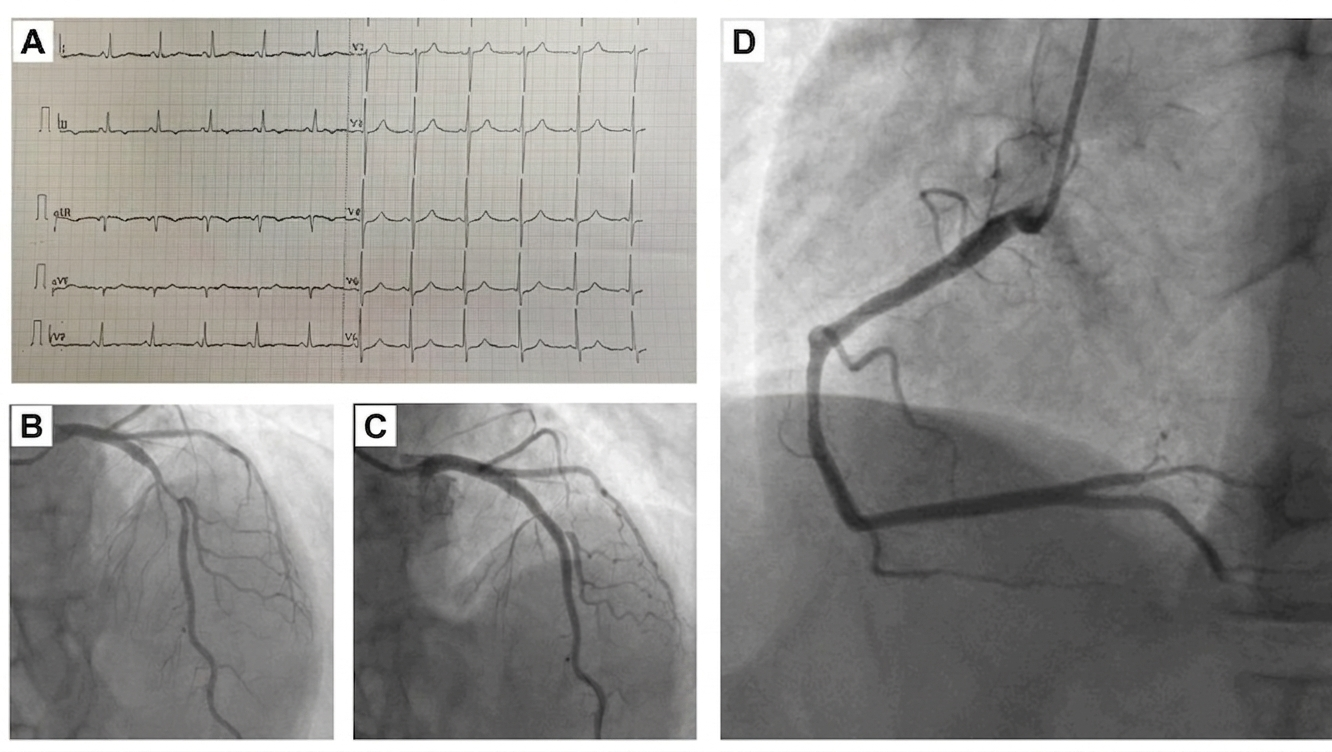
A 54-year-old man with a history of alcohol use, smoking, and hypertension presented with unstable angina. Baseline electrocardiogram and transthoracic echocardiography were unremarkable. Coronary angiography revealed double-vessel disease with critical stenosis of the left anterior descending artery (LAD) (90%) and intermediate stenosis of the right coronary artery (RCA) (60%-70%). Percutaneous coronary intervention (PCI) and stenting to the LAD was successfully performed (Figure 1).
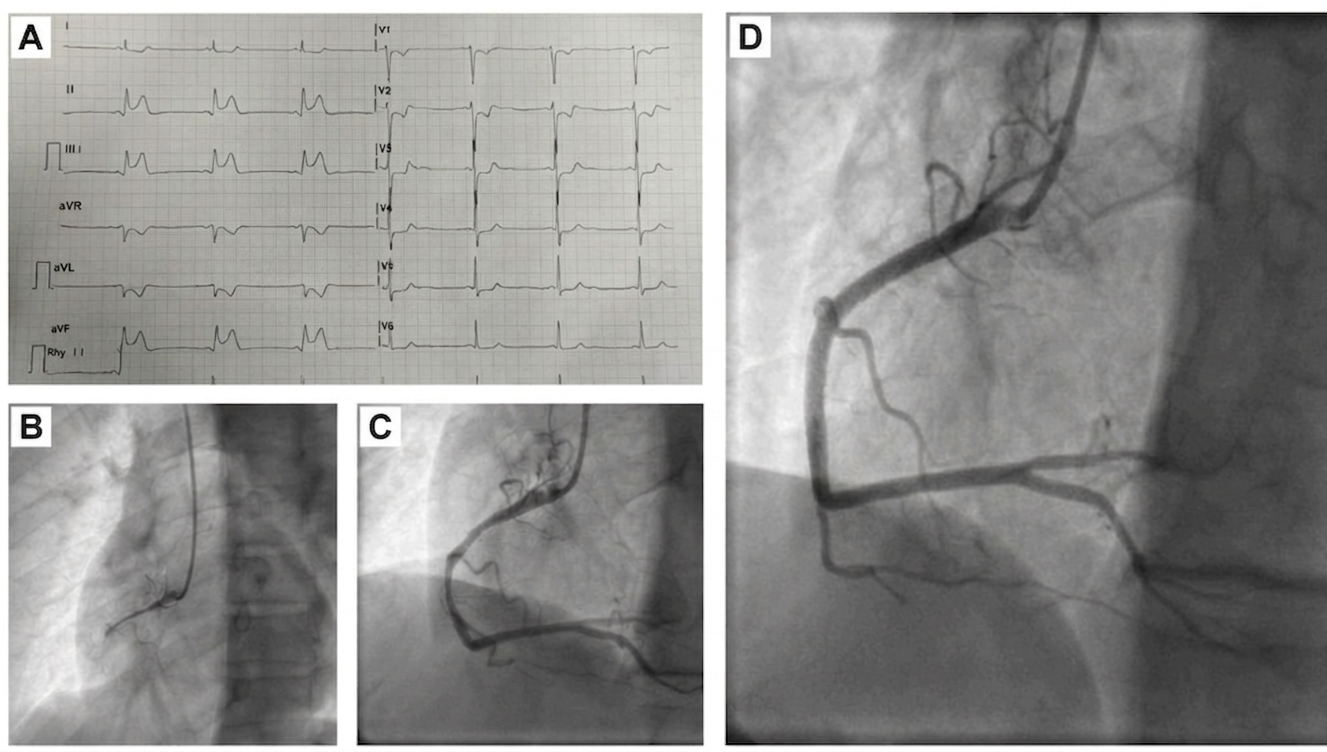
Within 24 hours, the patient developed acute chest pain with ST-segment elevation in the inferior leads (II, III, aVF) with reciprocal anterior changes. He was taken emergently for repeat angiography, which demonstrated severe diffuse spasm of the RCA without acute thrombotic occlusion. The spasm completely resolved following intracoronary nitroglycerin, with prompt relief of symptoms and normalization of the ST segments (Figure 2, Video).
However, recurrent episodes of RCA spasm requiring repeated intracoronary vasodilator therapy were observed, and a residual fixed atherosclerotic lesion persisted (Video). Given the presence of an underlying significant atherosclerotic lesion and recurrent vasospasm, PCI with stent implantation to the mid-RCA was performed with a good angiographic result (Figure 2, Video).
This case represents vasospastic angina presenting as transient ST-elevation myocardial infarction in the early post-PCI period. The possibility of Kounis syndrome type II was also considered; however, in the absence of clinical features of hypersensitivity, it was less likely. Recognition of coronary vasospasm as a cause of acute ST-segment elevation is essential, as it is rapidly reversible with intracoronary nitrates; however, coexistent fixed coronary disease may warrant revascularization in selected cases.
Affiliations and Disclosures
Keshav Sachdeva, MD, DM; Vandeep Basra, MD, DM; Suraj Kumar, MD, DM; Bhupinder Singh, MD, DM; Tejinder Singh Malhi, MD, DM
From the Department of Cardiology, All India Institute of Medical Sciences, Bathinda, India.
Disclosures: The authors report no financial relationships or conflicts of interest regarding the content herein.
Consent statement: The authors confirm that informed consent was obtained from the patient and family for the intervention described in the manuscript and for the publication of thereof, including photographs.
Address for correspondence: Tejinder Singh Malhi, MD, DM, Department of Cardiology, All India Institute of Medical Sciences, Bathinda 151001, India. Email: tejimalhi@gmail.com












