

Left Ventricular Contrast Staining During Venoarterial Extracorporeal Membrane Oxygenation
© 2026 HMP Global. All Rights Reserved.
Any views and opinions expressed are those of the author(s) and/or participants and do not necessarily reflect the views, policy, or position of the Journal of Invasive Cardiology or HMP Global, their employees, and affiliates.
J INVASIVE CARDIOL 2026. doi:10.25270/jic/26.00200. Epub July 8, 2026.
A 72-year-old woman with a recent history of stent implantation in the left anterior descending (LAD) and circumflex (Cx) arteries, as well as a known inferior left ventricular (LV) aneurysm (Figure A, asterisk) secondary to previous myocardial infarction, presented with out-of-hospital cardiac arrest requiring venoarterial extracorporeal membrane oxygenation (VA-ECMO) support.
Emergency coronary angiography revealed acute in-stent thrombosis of both the LAD and Cx, which was successfully treated with balloon angioplasty.
During the procedure, a progressively increasing extracoronary contrast blush was observed (Figure B and C, arrows), raising concern for a mechanical complication. However, urgent transthoracic echocardiography showed no pericardial effusion. Computed tomography (CT) subsequently excluded hemopericardium and active contrast extravasation, ruling out LV free-wall rupture. Instead, CT demonstrated localized contrast pooling at the site of the pre-existing inferior ventricular aneurysm (Figure D-F, arrows).
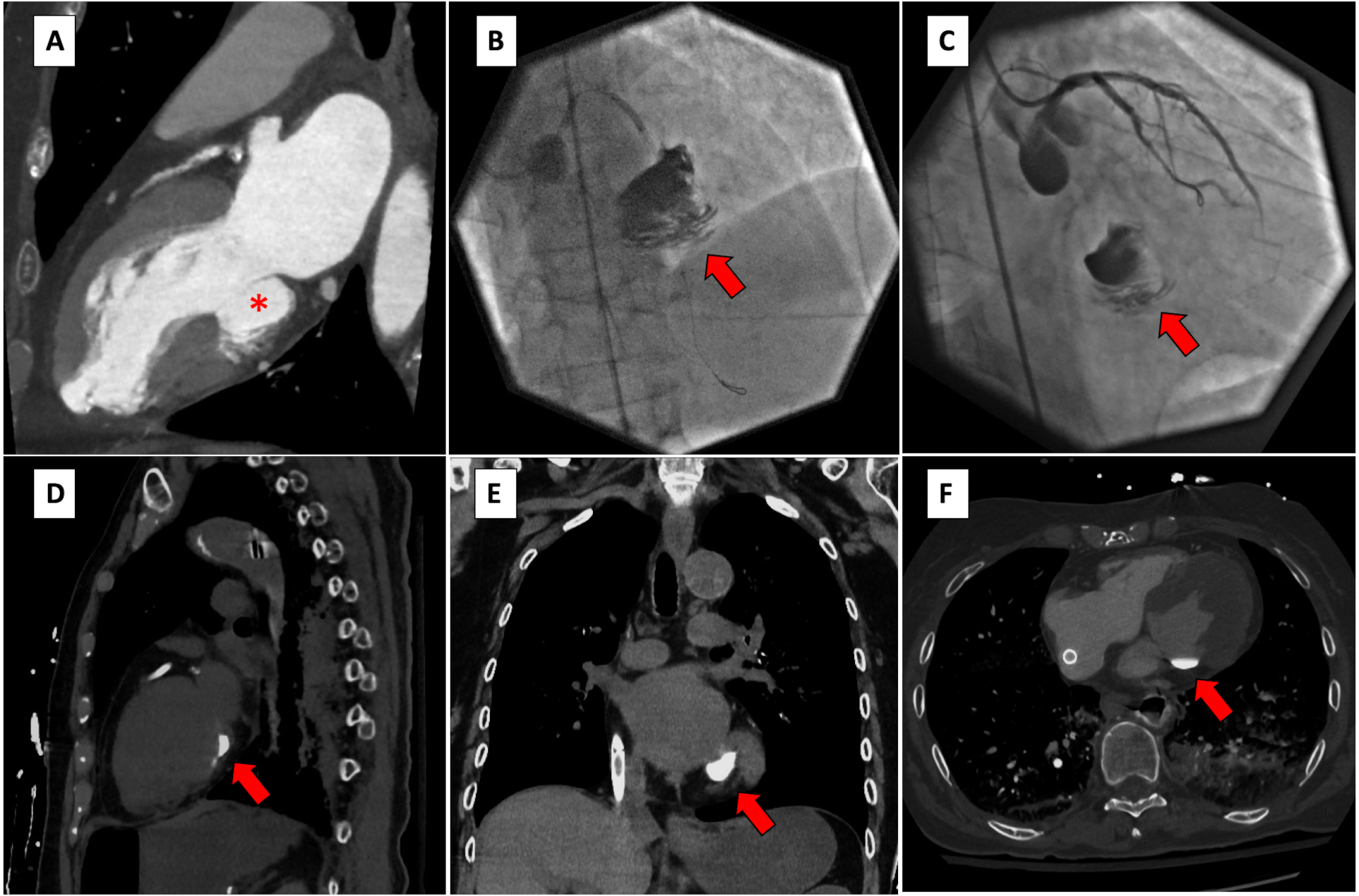
The imaging findings were interpreted in the context of VA-ECMO-related hemodynamics. Mechanical circulatory support, combined with absent aortic valve opening and negligible native LV ejection, promoted contrast stagnation within the LV cavity, particularly in gravity-dependent regions and within the aneurysmal segment. Minimal aortic regurgitation may have facilitated retrograde contrast entry into the LV, while the absence of effective ventricular ejection allowed persistent contrast retention (Video). Despite successful coronary revascularization, the patient subsequently died following an intestinal hemorrhagic complication.
These images highlight how VA-ECMO can markedly impair LV emptying, generating imaging findings that mimic acute mechanical complications. Recognition of this phenomenon is important to avoid misdiagnosis during percutaneous coronary intervention performed under VA-ECMO support. In this setting, contrast staining within the LV should be interpreted cautiously, as it may represent absent or minimal native ventricular ejection rather than mechanical complications.
These images also reinforce the importance of considering active LV unloading strategies during VA-ECMO, such as percutaneous mechanical support with a microaxial flow pump, to reduce intracavitary stasis and improve ventricular unloading.
Affiliations and Disclosures
Enrico Fabris, MD, PhD1; Gloria Lorenzon, MD1,2; Giancarlo Vitrella, MD1; Andrea Perkan, MD1; Gianfranco Sinagra, MD1,3
From the 1Cardiothoracovascular Department, University of Trieste, Trieste, Italy; 2Postgraduate School of Cardiovascular Medicine, University of Trieste, Trieste, Italy; 3European Reference Network for Rare, Low Prevalence and Complex Diseases of the Heart-ERN GUARD-Heart.
Disclosures: The authors report no financial relationships or conflicts of interest regarding the content herein.
Consent statement: The intervention was performed as an emergency, life-saving procedure following cardiac arrest under conditions of medical necessity; therefore, informed consent could not be obtained prior to treatment. The patient is deceased. The images have been fully anonymized to ensure that the patient cannot be identified.
Address for correspondence: Gianfranco Sinagra, MD, FESC, FHFA, Cardiothoracovascular Department, University of Trieste, Trieste, Italy. Email: gianfranco.sinagra@asugi.sanita.fvg.it













