Endograft-Facilitated Overexpansion of a Calcified Right Ventricle-to-Right Pulmonary Artery Contegra Conduit for Transcatheter Pulmonary Valve Replacement
© 2026 HMP Global. All Rights Reserved.
Any views and opinions expressed are those of the author(s) and/or participants and do not necessarily reflect the views, policy, or position of the Journal of Invasive Cardiology or HMP Global, their employees, and affiliates.
J INVASIVE CARDIOL 2026. doi:10.25270/jic/26.00168. Epub July 7, 2026.
A 34-year-old woman with truncus arteriosus type A3 status post 4 prior sternotomies and failed unifocalization presented with severe stenosis of a heavily calcified 22-mm Contegra right ventricle-to-right pulmonary artery (RV-RPA) conduit (Medtronic). The left lung was supplied by aortopulmonary collaterals. She was referred for transcatheter conduit rehabilitation and pulmonary valve replacement.
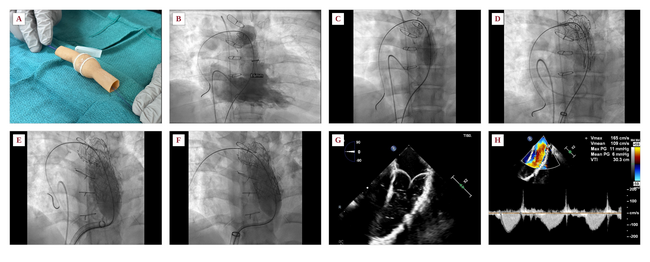
Benchtop testing demonstrated that a Contegra conduit could be substantially overdilated (Figure A, Video). Angiography confirmed severe conduit stenosis (Figure B). After predilation with a 14-mm Atlas Gold balloon (BD) (Figure C), a 31 × 10-cm GORE TAG Conformable Thoracic Endograft (W.L. Gore & Associates) was deployed to mitigate the risk of conduit disruption and bleeding during aggressive expansion. Despite marked initial underexpansion within the calcified conduit, the graft maintained patency and allowed serial dilation to 28 mm using a 28-mm True balloon (BD) (Figure D). Persistent proximal recoil was treated with Palmaz XL 5010 bare-metal stent (Cordis) reinforcement until trivial recoil remained (Figure E). A 29-mm SAPIEN S3 valve (Edwards Lifesciences) was then implanted with full expansion and no recoil (Figure F). Intracardiac echocardiography demonstrated thin mobile leaflets without valvular or paravalvular regurgitation (Figure G), and Doppler showed a mean systolic gradient of 6 mm Hg (Figure H).
This case demonstrates the first reported use of a full-length self-expanding thoracic endograft for RV-RPA conduit rehabilitation and successful implantation of a fully expanded 29-mm SAPIEN S3 valve within a 22-mm Contegra conduit. These findings highlight the expandable nature of Contegra conduits and reinforce that valve sizing should be determined after endovascular conduit revision rather than by the original surgical conduit diameter alone.
Affiliations and Disclosures
Pradyumna Agasthi, MD1; Kaitlyn Krebushevski, MD2,3; Allison K. Cabalka, MD2,3; Jason H. Anderson, MD2,3
From the 1Department of Cardiology, Saint Francis Heart and Vascular Institute, Tulsa, Oklahoma; 2Department of Pediatric and Adolescent Medicine, Division of Pediatric Cardiology, Mayo Clinic, Rochester, Minnesota; 3Department of Cardiovascular Medicine, Division of Structural Heart Diseases, Mayo Clinic, Rochester, Minnesota.
Disclosures: Dr Cabalka is a consultant for Edwards Lifesciences and B. Braun Medical, Inc. Dr Anderson is on the cardiac advisory board for W.L. Gore & Associates and is a consultant for Edwards Lifesciences and Medtronic. The remaining authors report no financial relationships or conflicts of interest regarding the content herein.
Consent statement: Informed consent was obtained for the intervention and publication of this report, including all images.
Address for correspondence: Jason H. Anderson, MD, Mayo Clinic, Rochester, MN 55905, USA. Email: Anderson.Jason@mayo.edu; X: @Dr_JHAnderson, @PradyAgasthiMD