Modified Tunnel-in-Landslide Technique (TILT) Using Ping-Pong Guides
© 2026 HMP Global. All Rights Reserved.
Any views and opinions expressed are those of the author(s) and/or participants and do not necessarily reflect the views, policy, or position of the Journal of Invasive Cardiology or HMP Global, their employees, and affiliates.
J INVASIVE CARDIOL 2026. doi:10.25270/jic/26.00108. Epub April 17, 2026.
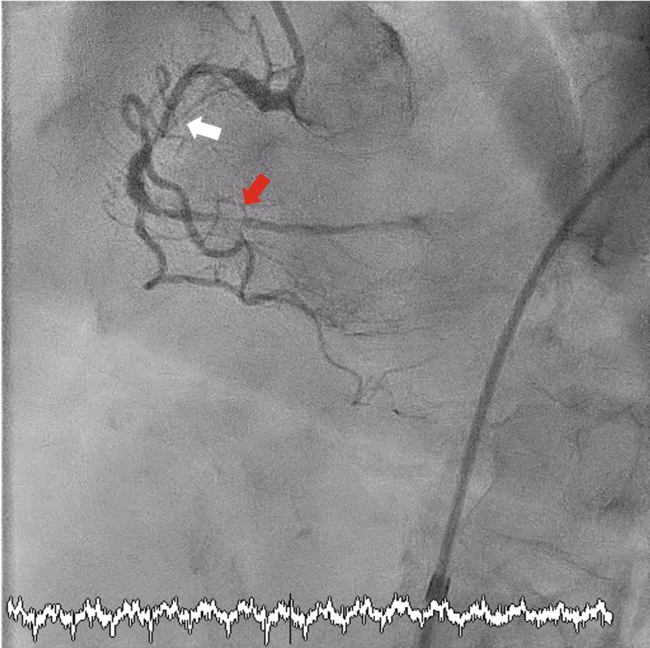
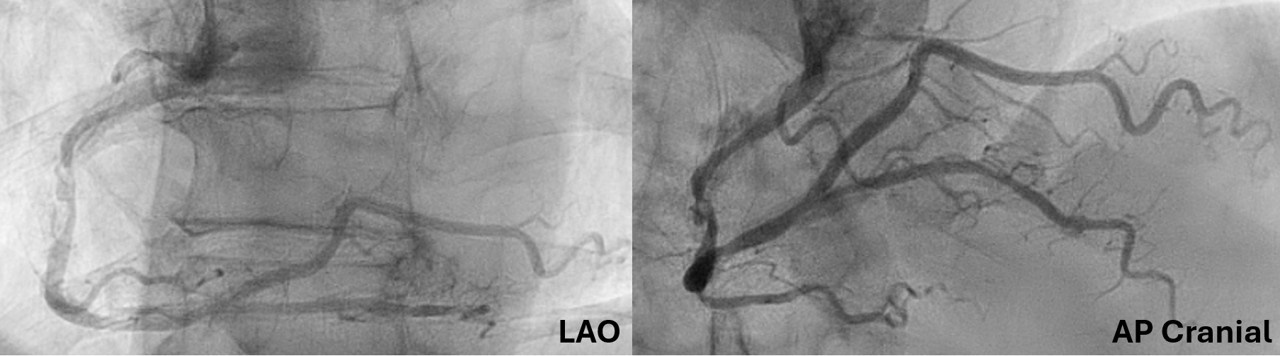
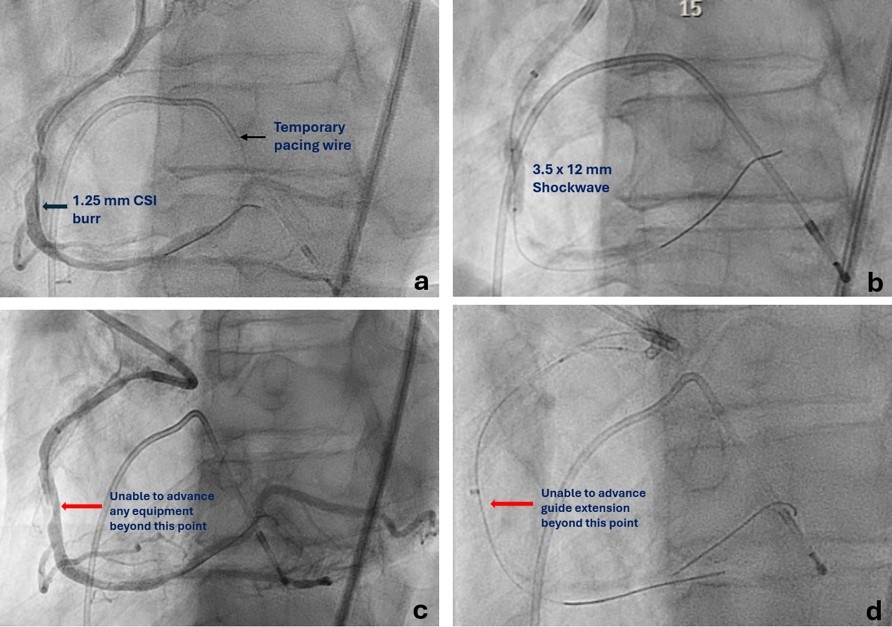
A 65-year-old man presented with unstable angina and calcified right coronary artery (RCA) stenosis (Figure 1) on diagnostic catheterization via radial approach. Percutaneous coronary intervention (PCI) was performed via 7F femoral access using a Judkin’s Right (JR) 4 catheter followed by an Amplatz Left 0.75 guide catheter. Orbital atherectomy (aborted after 6 runs at low-speed because of no-reflow) followed by intravascular lithotripsy (IVL) using a 3.5 mm Shockwave C2+ (Shockwave Medical) was performed. Following this, no equipment could be advanced beyond the mid-RCA calcified nodule (Figure 2).
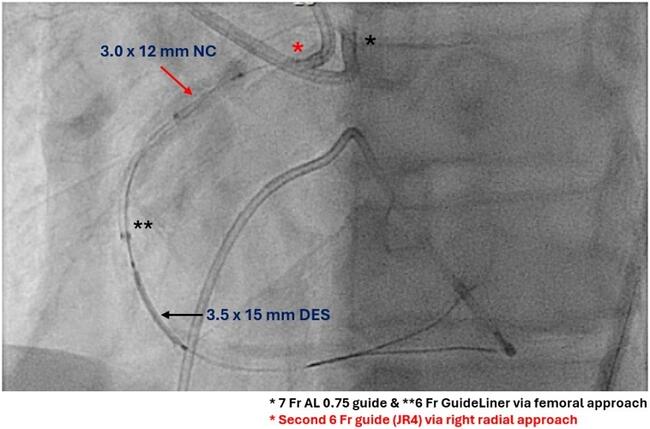
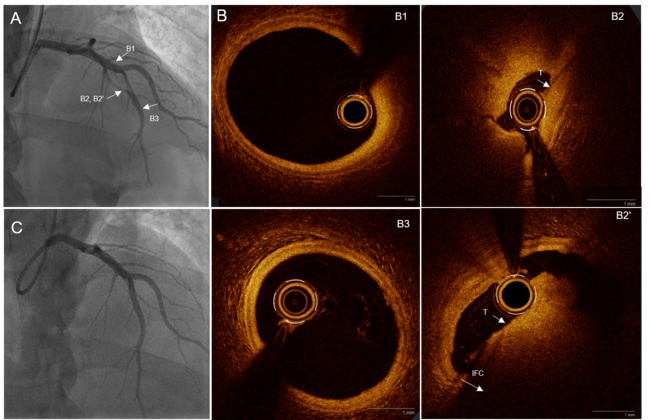
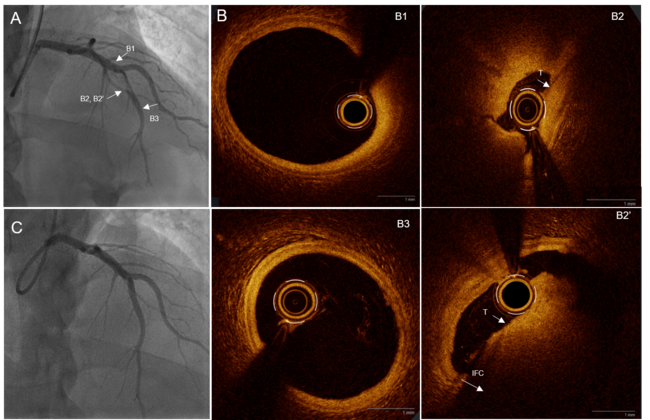
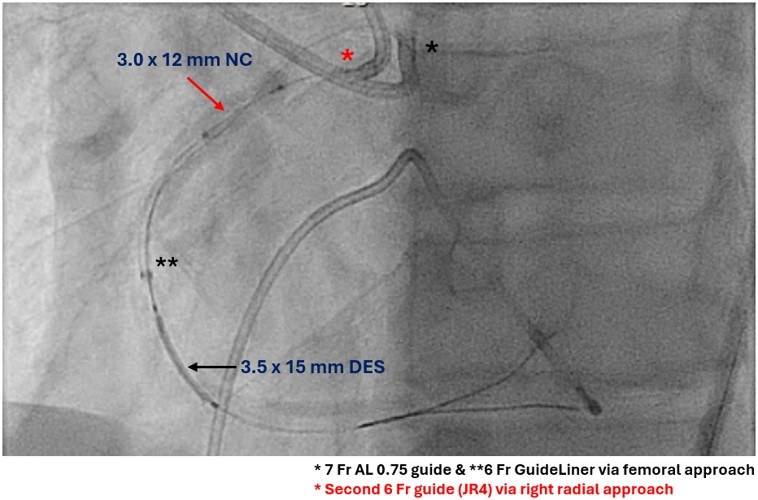
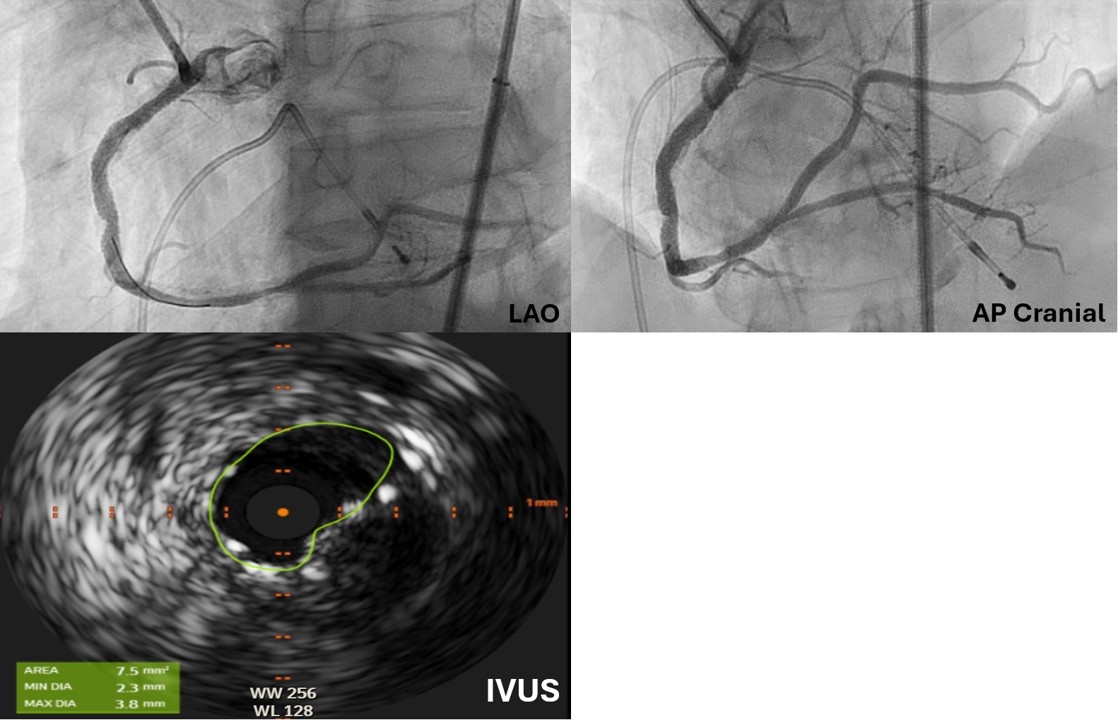
It was decided to use ping-pong guides for the modified tunnel-in-landslide technique (TILT). A second guide (6F JR4) engaged the RCA from the radial approach, and a 3.0-mm balloon was inflated in the proximal RCA to trap the 6F guide extension (GE) (Figure 3). With this maneuver, the operator was successfully able to deliver the balloons and stent (Figure 3, Video 1), followed by a larger (4.0-mm) IVL balloon. The final angiogram (after stenting the remaining RCA) showed a good result, with an intravascular ultrasound minimal stent area of 7.5 mm² (Figure 4, Video 2).
TILT facilitates equipment delivery through a GE (“tunnel”) pinned by inflating a balloon between the vessel wall and the GE (“landslide”).1 The original technique used single 8F arterial access with a 5F GE,1 which can be modified using ping-pong guides (the second guide is used to deliver the “blocking” balloon), both of which can be 6F or 7F.2,3 This requires dual arterial access that is either already in place (eg, chronic total occlusion PCI) or can be obtained (eg, radial-to-femoral for complex ad-hoc PCI). This technique facilitates equipment delivery when conventional approaches fail.
Affiliations and Disclosures
Neeraj Shah, MD, MPH
From the Independence Health Westmoreland Hospital, Greensburg, Pennsylvania.
Disclosures: The author reports no financial relationships or conflicts of interest regarding the content herein.
Consent statement: The authors confirm that informed consent was obtained from the patient(s) for the intervention(s) described in the manuscript and for the publication thereof, including any and all images.
Address for correspondence: Neeraj Shah, MD, Independence Health Westmoreland Hospital, 532 W Pittsburgh St, Greensburg, PA 15601, USA. Email: neerajshah86@gmail.com; X: @NeerajShahMD
References
1. Santiago R, Moroni F, Del Rio V, Rodriguez-Escudero J, Azzalini L. The guide extension tunnel in landslide technique (TILT) for equipment delivery in severely tortuous or uncrossable lesions during percutaneous coronary intervention. EuroIntervention. 2021;17(11):e923-e924. doi:10.4244/EIJ-D-21-00454
2. Allana SS, Kostantinis S, Simsek B, Karacsonyi J, Rempakos A, Brilakis ES. Tunnel in landslide technique to "block and deliver": a novel method to deliver covered stent for coronary perforation. JACC Cardiovasc Interv. 2023;16(6):730-733. doi:10.1016/j.jcin.2023.01.368
3. Smith D, Koshy S, Allana SS. Getting the stent to deliver: strategies for PCI in calcified and tortuous vessels. Cardiac Interventions Today. 2025;19(1):30-33.